Circle of willis
Reading File
Finding Sources
Searching the Web
Circle of Willis anatomy components clinical significance
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a comprehensive overview of the Circle of Willis based on medical textbooks:
Circle of Willis (Circulus Arteriosus Cerebri)
Anatomy
The Circle of Willis is an anastomotic arterial ring located at the base of the brain (on the ventral surface), sitting within the subarachnoid space of the interpeduncular cistern. It connects the two major blood supplies to the brain - the anterior circulation (internal carotid arteries) and the posterior circulation (vertebrobasilar system).
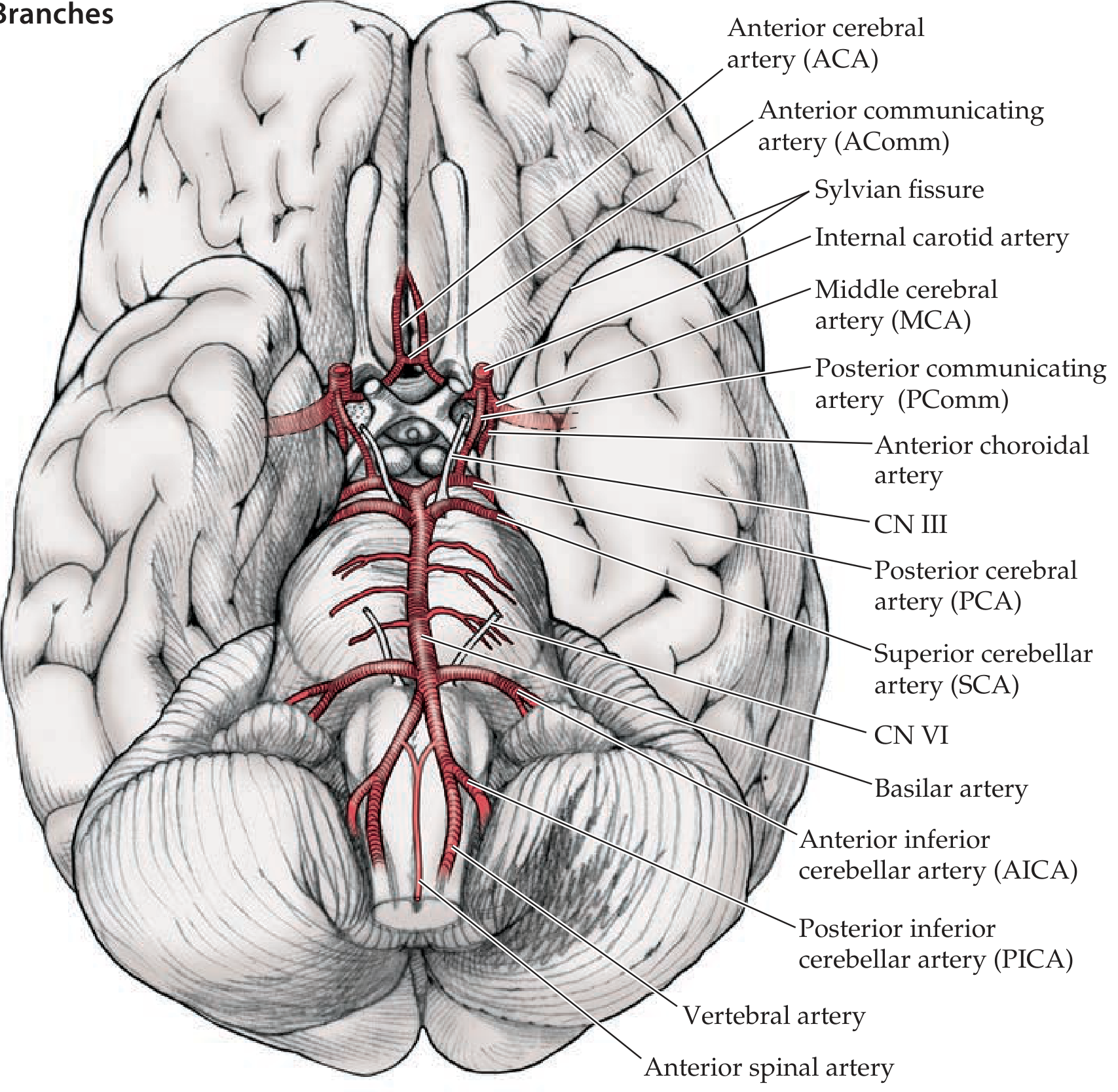
(Neuroanatomy through Clinical Cases, 3rd Ed. - Circle of Willis and Its Main Branches)
Components
The ring is typically described as having anterior and posterior portions:
Anterior Part (Carotid-derived)
| Vessel | Notes |
|---|---|
| Right & Left Internal Carotid Arteries (ICA) | Enter the cranial cavity; each divides into ACA and MCA |
| Right & Left Anterior Cerebral Arteries (ACA) | Terminal branches of the ICA; supply medial frontal/parietal lobes |
| Anterior Communicating Artery (AComm) | Single vessel connecting the two ACAs; completes the anterior ring |
Posterior Part (Vertebrobasilar-derived)
| Vessel | Notes |
|---|---|
| Basilar Artery | Formed by union of two vertebral arteries at the pontomedullary junction |
| Right & Left Posterior Cerebral Arteries (PCA) | Arise from the top of the basilar artery; supply occipital lobes and parts of the thalamus |
| Right & Left Posterior Communicating Arteries (PComm) | Connect the ICAs to the PCAs, joining anterior and posterior circulations |
The Middle Cerebral Arteries (MCA) are branches of the ICA that arise at the circle but are not technically part of the ring itself - they exit laterally into the Sylvian fissure.
Diagrams
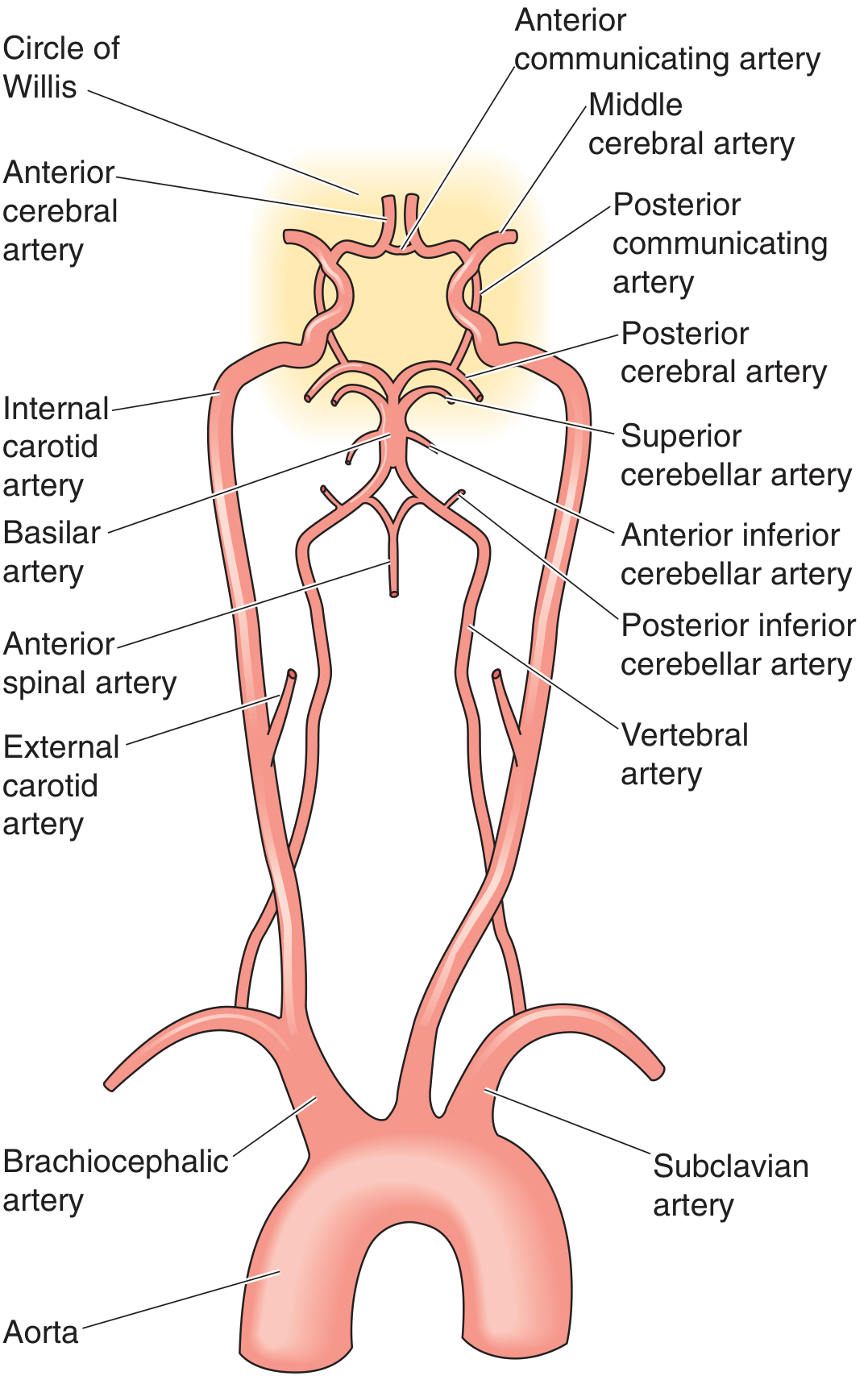
(Medical Physiology - Vascular anatomy showing the Circle of Willis and its major arterial supply from aorta to brain)
Collateral Function
The primary role of the Circle of Willis is to act as a collateral anastomosis: if one feeding vessel becomes occluded (e.g., a carotid artery), blood can theoretically be redistributed from the opposite side or from the posterior circulation to compensate. The circle connects:
- Right and left carotid systems (via AComm)
- Each carotid to the vertebrobasilar system (via PComms)
- Posterior circulation to anterior circulation bilaterally
As stated in Schwartz's Principles of Surgery: "The circle of Willis provides extensive collateral circulation, as it connects the right and left carotid arteries to each other and each to the vertebrobasilar system."
Sources of brain collateral beyond the circle include anastomoses between extracranial and intracranial arteries, and leptomeningeal anastomoses between terminal branches of cerebral and cerebellar arteries. - Localization in Clinical Neurology, 8e
Anatomical Variations (Very Common)
A complete, full-caliber ring is present in only approximately 34% of individuals (Neuroanatomy through Clinical Cases) - other sources cite <50%. Common variations include:
- Hypoplastic or absent PComm - most common variant; reduces posterior-anterior collateral
- Hypoplastic A1 segment of ACA - reduces communication between hemispheres anteriorly
- Fetal-type PCA - PCA arises predominantly from the ICA rather than the basilar artery (in ~20-25% of people)
- Aplasia of entire segments
These variations are clinically significant: hypoplasia of communicating arteries means decreased collateral supply and increased risk of infarction when a parent vessel is occluded.
Clinical Relevance
1. Stroke & Ischemia
The circle governs collateral flow in acute and chronic cerebrovascular occlusive disease. Patients with complete occlusion proximal to the circle may survive without infarction if collaterals are robust; those with incomplete circles are more vulnerable. It is well visualized on MR angiography (MRA) and CT angiography (CTA). - Grainger & Allison's Diagnostic Radiology
2. Berry (Saccular) Aneurysms
The bifurcation points of the circle are the most common sites for intracranial aneurysms. The turbulent flow at junctions creates wall stress predisposing to aneurysm formation. Classic sites:
- AComm - most common (~30-35%)
- ICA-PComm junction - second most common; can compress CN III causing a "blown pupil"
- MCA bifurcation
- Basilar tip
Rupture causes subarachnoid hemorrhage (SAH) - presenting as the classic "thunderclap headache" / "worst headache of life." - Robbins & Cotran Pathologic Basis of Disease
3. Carotid Endarterectomy
During carotid clamping, blood supply to the ipsilateral hemisphere depends entirely on collateral flow from an intact circle of Willis. Autopsy studies show the majority of specimens have anatomic anomalies in the circle, making neurophysiologic monitoring essential. - Barash, Cullen & Stoelting's Clinical Anesthesia, 9e
4. Watershed Infarcts
When global perfusion drops (e.g., cardiac arrest, hypotension), the most vulnerable areas are the watershed zones between adjacent arterial territories - the borders between ACA/MCA and MCA/PCA territories.
Memory Aid
A common mnemonic for the components (going around the circle):
"2 ACAs, 1 AComm, 2 ICAs, 2 PComms, 2 PCAs" - 9 vessels total in the complete ring.
Sources: Neuroanatomy through Clinical Cases 3rd Ed. | Medical Physiology (Boron & Boulpaep) | Miller's Anesthesia 10e | Barash's Clinical Anesthesia 9e | Localization in Clinical Neurology 8e | Schwartz's Principles of Surgery 11e | Grainger & Allison's Diagnostic Radiology | Robbins & Cotran Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.