Aqueous humour production drainage and passage
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I have comprehensive, well-illustrated content from four major textbooks. Here is the complete answer:
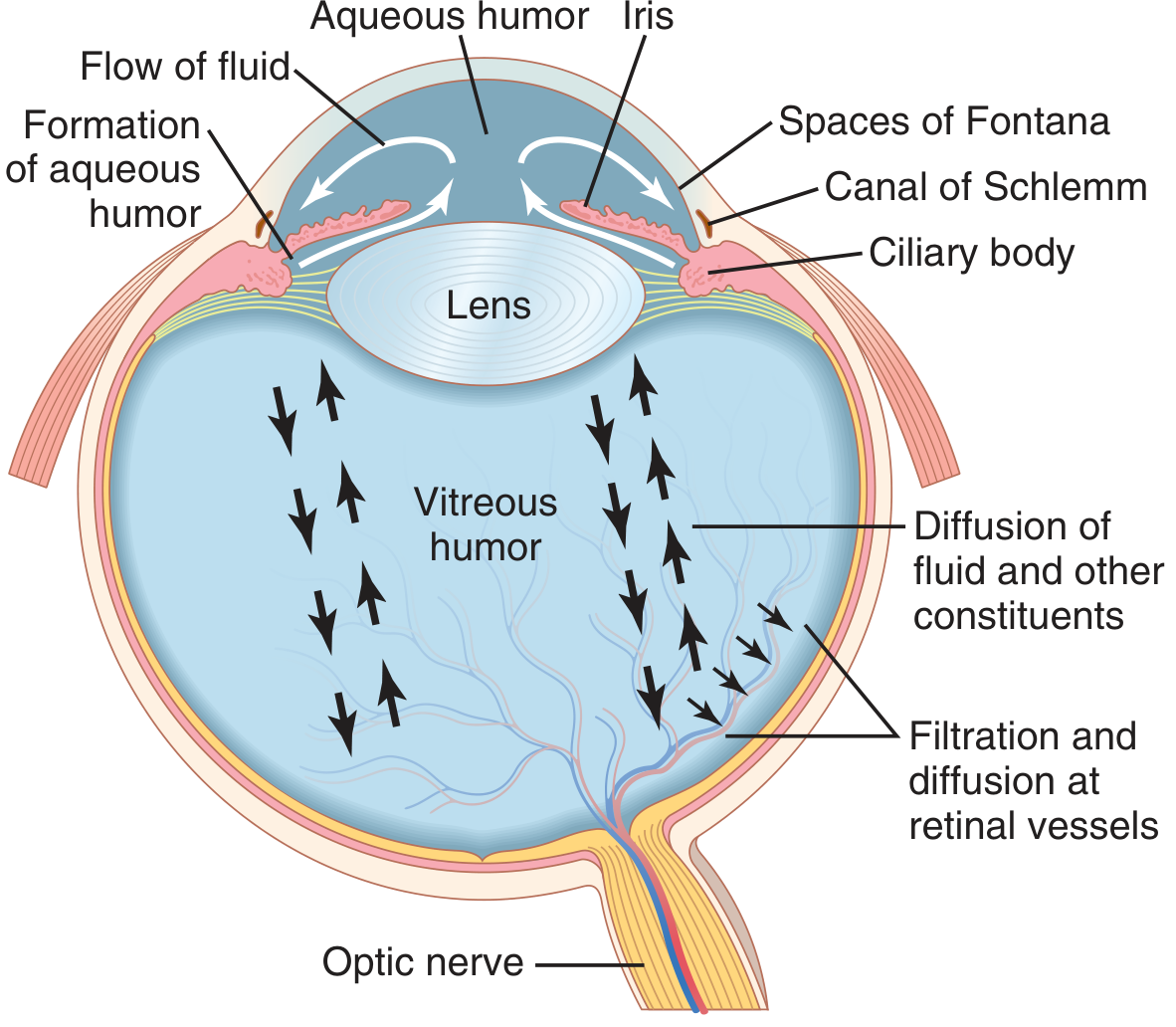
Aqueous Humour - Production, Passage, and Drainage
1. Production (Formation)
Aqueous humour is produced by the ciliary processes of the ciliary body, which project into the posterior chamber. Two mechanisms contribute:
Active Secretion (2/3 of total)
The ciliary body epithelium actively secretes aqueous into the posterior chamber via a two-step process:
- Sodium ions are actively transported into the intercellular spaces of the ciliary epithelium
- Chloride and bicarbonate ions passively follow sodium to maintain electrical neutrality
- This ionic gradient drives osmosis of water from the underlying capillaries into those spaces, which then washes into the posterior chamber
Two enzyme systems are critical to this active process: carbonic anhydrase and cytochrome oxidase. Because of the active secretory mechanism, the osmotic pressure of aqueous humour is many times greater than that of plasma.
Additional nutrients transported by facilitated mechanisms include amino acids, ascorbic acid, and glucose.
Passive Filtration (1/3 of total)
The remaining one-third is formed by passive ultrafiltration from the vessels on the anterior surface of the iris.
Rate of production: ~2 µL/min, which is relatively constant under normal conditions.
2. Passage (Circulation)
Once formed in the posterior chamber, aqueous humour follows a well-defined path:
Posterior chamber (where it is produced, ~50 µL volume)
↓
Through the pupillary aperture (between iris and lens)
↓
Anterior chamber (~250 µL volume) - here it mixes with aqueous from the iris and bathes the avascular lens and the corneal endothelium
↓
Peripheral anterior chamber angle (the iridocorneal angle - angle between the iris root and peripheral cornea)
↓
Outflow pathways (see below)
↓
Through the pupillary aperture (between iris and lens)
↓
Anterior chamber (~250 µL volume) - here it mixes with aqueous from the iris and bathes the avascular lens and the corneal endothelium
↓
Peripheral anterior chamber angle (the iridocorneal angle - angle between the iris root and peripheral cornea)
↓
Outflow pathways (see below)
During this journey, aqueous humour serves two key functions:
- Provides nutrition to avascular structures (lens, corneal endothelium)
- Maintains intraocular pressure (IOP)
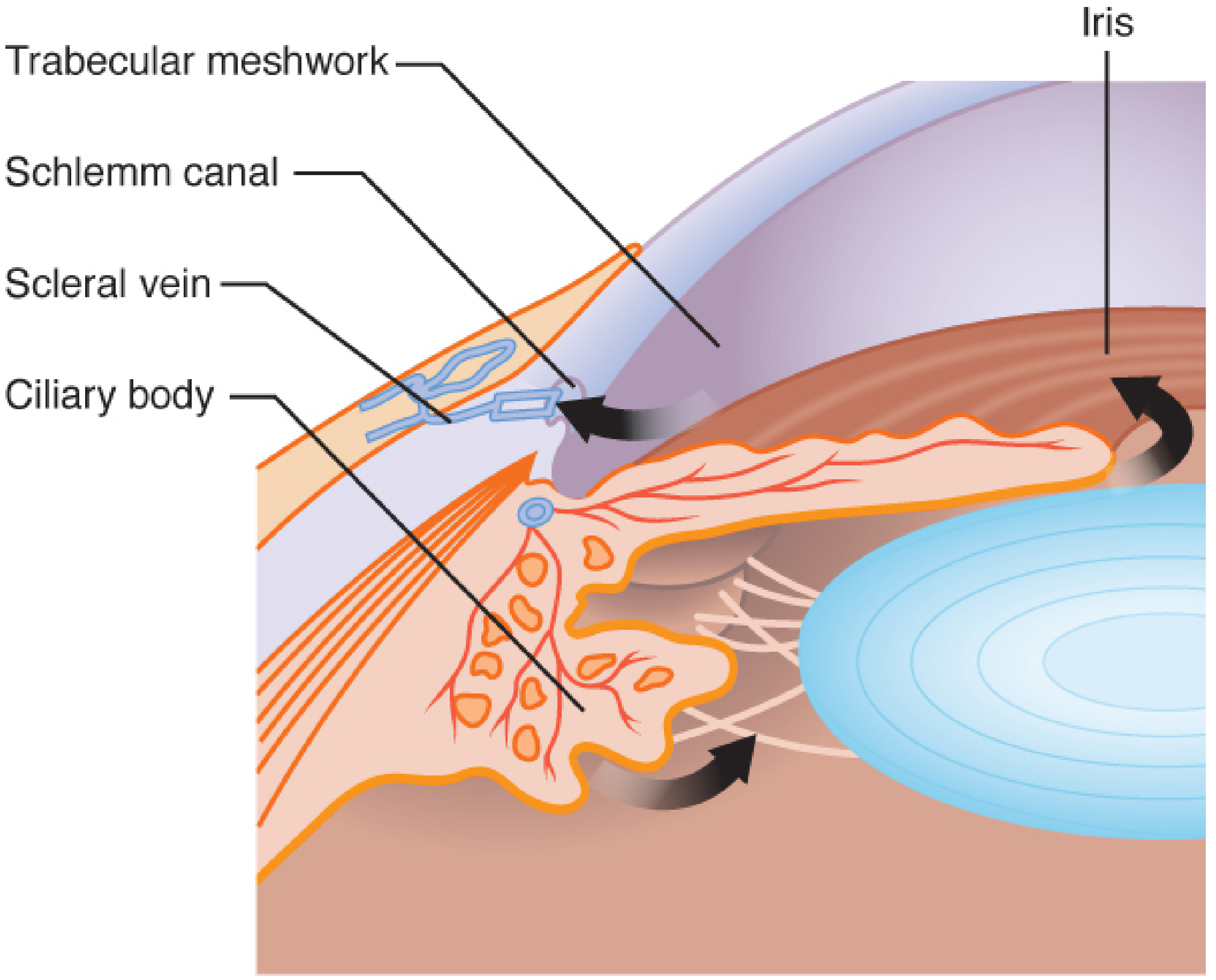
3. Drainage Pathways
Primary (Conventional) Pathway - 80-95% of outflow
Trabecular meshwork → Canal of Schlemm → Episcleral venous plexus → Systemic circulation
Step by step:
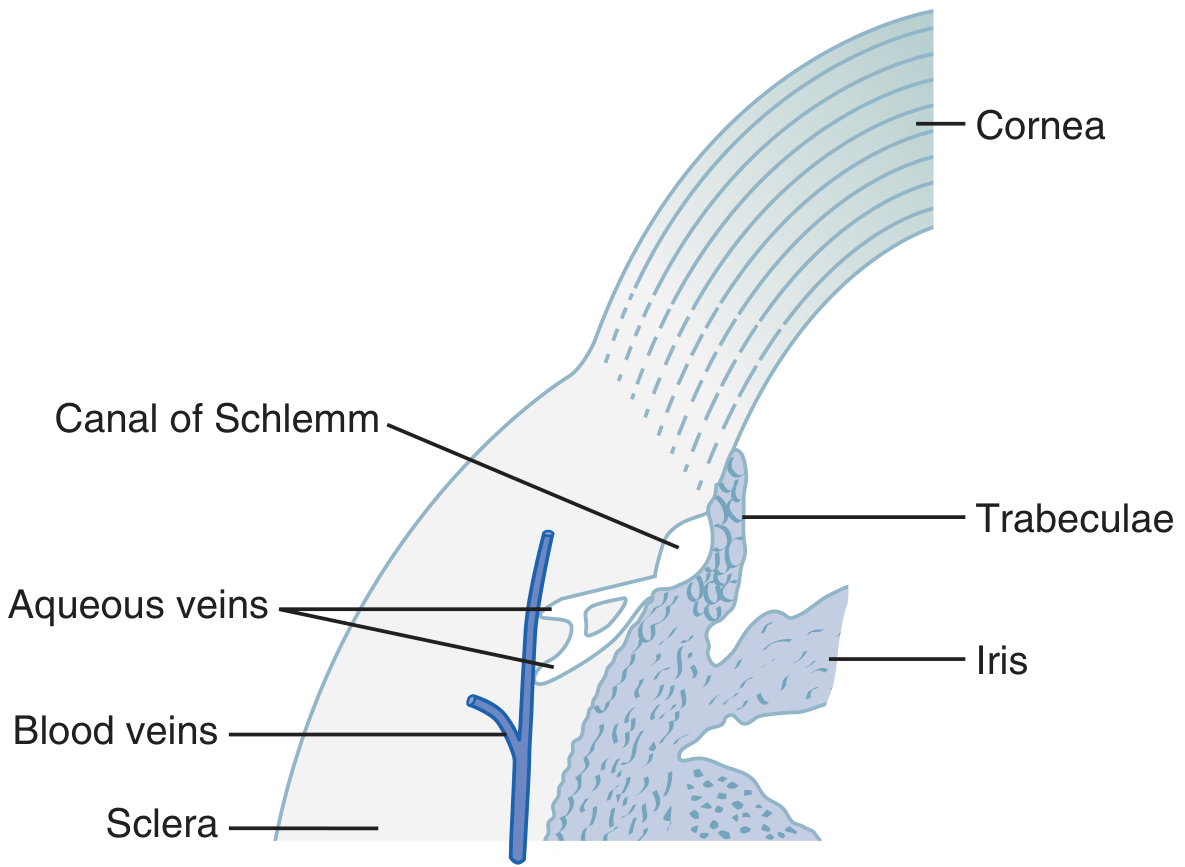
- Aqueous flows into the trabecular meshwork (a cobweb-like porous structure at the iridocorneal angle, also called the Spaces of Fontana)
- Passes through the trabecular spaces into the canal of Schlemm - a thin-walled, circumferential vein that runs 360° around the eye. Its endothelium is highly porous, permitting even large protein molecules and particles up to the size of red blood cells to pass through. It normally contains only aqueous (not blood)
- From Schlemm's canal, fluid drains into aqueous veins (small veins that carry only aqueous) and then into episcleral veins
- Ultimately drains into the superior vena cava and right atrium
Clinical implication: Obstruction of venous return at any point from the eye to the right heart can impede aqueous drainage and raise IOP.
Secondary (Uveoscleral) Pathway - 5-20% of outflow
Fluid flows through the ciliary muscle into the suprachoroidal space, bypassing the trabecular meshwork. This is the primary target of prostaglandin analogue drugs (e.g., latanoprost) used in glaucoma therapy.
4. Intraocular Pressure (IOP)
The balance between production and drainage determines IOP:
| Parameter | Normal Value |
|---|---|
| Normal IOP | 10-21 mmHg (Bailey & Love); average ~15 mmHg (Guyton) |
| Abnormal threshold | >22 mmHg |
| Diurnal variation | 2-5 mmHg (higher on awakening) |
| Cardiac cycle variation | 1-2 mmHg per beat |
5. Summary Flowchart
Ciliary processes (active secretion + iris filtration)
↓
POSTERIOR CHAMBER
↓
Pupillary aperture
↓
ANTERIOR CHAMBER
(bathes lens + corneal endothelium)
↓
Iridocorneal angle
↓
┌────────────────────────────┐
│ │
Trabecular meshwork Uveoscleral route
(80-95%) (5-20%)
↓ ↓
Canal of Schlemm Suprachoroidal space
↓ ↓
Aqueous veins Choroidal vessels
↓
Episcleral veins
↓
Superior vena cava → Right atrium
6. Clinical Relevance - Glaucoma
Disruption of this system causes glaucoma:
- Open-angle glaucoma - increased resistance to outflow through an anatomically open trabecular meshwork (most common type in Western populations). Treated by drugs that reduce production (beta-blockers, carbonic anhydrase inhibitors) or increase outflow (prostaglandins, pilocarpine)
- Angle-closure glaucoma - the iris root physically covers the trabecular meshwork. In pupillary block, aqueous cannot pass from the posterior to anterior chamber, causing pressure build-up, forward bowing of the iris (iris bombé), and angle closure. Treated with laser iridotomy or surgical iridectomy to create a new passage
- Neovascular glaucoma - fibrovascular membranes (often from VEGF upregulation in retinal ischemia) grow over the iris and trabecular meshwork, blocking outflow
Sources:
- Guyton and Hall Textbook of Medical Physiology, Chapter 50 - The Eye
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9e - Formation and Drainage of Aqueous Humor
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Aqueous Humor Dynamics
- Robbins & Kumar Basic Pathology - Glaucoma
- Bailey and Love's Short Practice of Surgery, 28e - The Globe
Causes of sudden loss of vision and gradual loss of vision And painless and pain in case of loss of vision Refer ak kurana opt ha tb
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative ophthalmology sources. Let me compile the full answer now, structured in the AK Khurana style (which classifies vision loss by onset + pain):
Causes of Loss of Vision
Classification as per Ophthalmology (AK Khurana style)
Note: AK Khurana's Comprehensive Ophthalmology is not directly available in this library. The answer below is structured exactly as Khurana classifies it - by onset (sudden vs gradual) and by pain (painful vs painless) - synthesized from Kanski's Clinical Ophthalmology 10th ed., Wills Eye Manual, Tintinalli's Emergency Medicine, and Bailey & Love's Surgery, all of which follow the same standard ophthalmological classification.
CLASSIFICATION OF LOSS OF VISION
Loss of vision is classified on two axes:
- By onset - Sudden vs Gradual
- By pain - Painful vs Painless
A. SUDDEN (ACUTE) LOSS OF VISION
I. SUDDEN PAINLESS LOSS OF VISION
These are the most urgent emergencies - vision loss occurs without any pain:
| Condition | Key Features |
|---|---|
| Central Retinal Artery Occlusion (CRAO) | Sudden, complete, monocular. Pale retina + cherry red spot at fovea. Afferent pupillary defect (APD). Embolic cause (carotid, cardiac) |
| Central Retinal Vein Occlusion (CRVO) | Sudden monocular. "Blood and thunder" / "ketchup" fundus - flame haemorrhages in all 4 quadrants, disc oedema |
| Vitreous Haemorrhage | Sudden onset, floaters/cobwebs/haze. History of diabetes, sickle cell. Fundus obscured |
| Retinal Detachment | "Curtain coming down" field defect. Preceded by floaters + flashes (photopsia). APD if macula involved |
| Ischaemic Optic Neuropathy (AION) | Arteritic (GCA) or non-arteritic. Sudden monocular vision loss, swollen pale disc, APD |
| Giant Cell Arteritis (Temporal Arteritis) | Elderly patient. Headache, jaw claudication, tender temporal artery. Most feared cause - can cause bilateral blindness |
| Macular Hole / Haemorrhage / Cyst | Central vision loss, metamorphopsia |
| Cystoid Macular Oedema | Often post-surgical |
| Amaurosis Fugax | Transient monocular vision loss ("like a curtain"). Resolves within minutes. Due to carotid emboli. TIA equivalent |
| Hysterical (Functional) Blindness | Diagnosis of exclusion |
| Ophthalmic Artery Occlusion | More severe than CRAO; entire retina and choroid infarcted |
II. SUDDEN PAINFUL LOSS OF VISION
| Condition | Key Features |
|---|---|
| Acute Angle-Closure Glaucoma | Severe eye pain, headache, nausea/vomiting. Red eye, hazy cornea, mid-dilated fixed pupil, raised IOP (>40 mmHg), firm globe, shallow anterior chamber. Halos around lights |
| Corneal Ulcer / Abrasion | Foreign body sensation, watering, photophobia. Fluorescein staining positive |
| Acute Uveitis (Iritis/Iridocyclitis) | Deep aching pain, photophobia, ciliary flush, keratic precipitates, cells and flare in anterior chamber |
| Endophthalmitis | Severe pain, hypopyon, vitritis. Usually post-operative or traumatic |
| Optic Neuritis | Pain on eye movement (retrobulbar). Sudden central visual loss, dyschromatopsia, APD. Young females. ~90% painful, ~10% painless |
| Corneal Hydrops (in keratoconus) | Sudden pain + vision loss due to Descemet's membrane rupture |
| Pituitary Apoplexy | Binocular. Sudden severe headache, bitemporal hemianopia, ophthalmoplegia |
B. GRADUAL (CHRONIC) LOSS OF VISION
I. GRADUAL PAINLESS LOSS OF VISION
The "big four" causes of chronic visual impairment worldwide:
| Condition | Key Features |
|---|---|
| Cataract | Most common cause of reversible blindness worldwide. Gradual, painless, hazy vision. Glare, reduced contrast |
| Open-Angle Glaucoma | Insidious onset, peripheral field loss first ("tunnel vision"), raised IOP, cupped disc. Painless until advanced |
| Diabetic Retinopathy | Background → proliferative. Microaneurysms, haemorrhages, exudates, new vessels. Bilateral |
| Age-Related Macular Degeneration (AMD) | Dry (gradual, geographic atrophy, drusen) or Wet (faster, CNVM, metamorphopsia). Central vision loss |
| Refractive Error | Most common cause overall of reduced vision. Correctable |
| Corneal Scar/Opacity | Trachoma, old infection, trauma |
| Chronic Angle-Closure Glaucoma | Creeping angle closure without acute attack |
| Optic Atrophy | Secondary to any cause - tumour, demyelination, ischaemia |
| Retinitis Pigmentosa | Hereditary. Night blindness + progressive peripheral field loss. Bone-spicule pigmentation |
| Optic Nerve Tumours / Glioma | Slow compression |
II. GRADUAL PAINFUL LOSS OF VISION
(Less common - pain accompanying chronic visual deterioration)
| Condition | Key Features |
|---|---|
| Dry Eye Syndrome / SPK | Aching, grittiness, burning. Vision blurs then clears with blinking |
| Chronic Uveitis | Low-grade aching, photophobia, recurrent |
| Scleritis | Deep boring pain, tenderness on palpation, associated systemic disease (RA, etc.) |
| Thyroid Eye Disease | Proptosis, exposure keratopathy, compressive optic neuropathy |
| Chronic Angle-Closure Glaucoma | Intermittent aching |
| Optic Neuritis (subacute) | Gradual over days-weeks with retroorbital pain |
QUICK MEMORY TABLE (AK Khurana Framework)
PAINFUL PAINLESS
┌─────────────────┬──────────────────────┐
SUDDEN │ Acute ACG │ CRAO │
(Acute) │ Optic neuritis │ CRVO │
│ Corneal ulcer │ Retinal detachment │
│ Uveitis │ Vitreous haemorrhage │
│ Endophthalmitis │ AION / GCA │
│ │ Macular pathology │
│ │ Amaurosis fugax │
├─────────────────┼──────────────────────┤
GRADUAL │ Dry eye/SPK │ Cataract │
(Chronic) │ Scleritis │ Open-angle glaucoma │
│ Chronic uveitis │ Diabetic retinopathy │
│ Thyroid eye dis. │ AMD │
│ │ Refractive error │
│ │ Retinitis pigmentosa │
└─────────────────┴──────────────────────┘
CLINICAL APPROACH TO VISUAL LOSS
A few key differentiators help narrow the diagnosis immediately:
- APD (afferent pupillary defect) present → retinal or optic nerve pathology (CRAO, CRVO, optic neuritis, retinal detachment)
- Red eye + pain → consider corneal pathology, uveitis, acute ACG
- Fundus not visible → vitreous haemorrhage, dense cataract
- Cherry red spot → CRAO
- "Blood and thunder" fundus → CRVO
- Elderly + temporal headache → Giant cell arteritis (treat with steroids urgently)
- Young female + pain on EOM → Optic neuritis (rule out MS)
- Floaters + flashes + curtain → Retinal detachment (surgical emergency)
Temporal arteritis / Giant cell arteritis deserves special emphasis - it is the most important diagnosis not to miss in elderly patients with sudden visual loss. Immediate high-dose systemic steroids can prevent blindness in the fellow eye. - Bailey & Love's Surgery, 28e
Sources:
- Wills Eye Manual - Classification of Decreased Vision (Monocular/Binocular, Acute/Chronic, Painful/Painless)
- Tintinalli's Emergency Medicine - Differential Diagnosis Table for Acute Visual Loss
- Kanski's Clinical Ophthalmology 10th ed. - Retinal vascular occlusions, optic neuropathy
- Bailey and Love's Short Practice of Surgery, 28e - Painless loss of vision
- Roberts & Hedges' Clinical Procedures in Emergency Medicine - Unilateral vision loss
Can you change the pattern of memory table I can’t understand it Same thing happened last time Use different one in future Now give me better one
Got it - no more ASCII box tables. Here is the memory table redone as a clean, readable format:
QUICK MEMORY TABLE - Loss of Vision
🔴 SUDDEN + PAINFUL
- Acute Angle-Closure Glaucoma
- Optic Neuritis (pain on eye movement)
- Corneal Ulcer / Abrasion
- Acute Uveitis (Iritis)
- Endophthalmitis
- Corneal Hydrops
🟡 SUDDEN + PAINLESS
- Central Retinal Artery Occlusion (CRAO)
- Central Retinal Vein Occlusion (CRVO)
- Retinal Detachment
- Vitreous Haemorrhage
- Ischaemic Optic Neuropathy (AION)
- Giant Cell Arteritis (Temporal Arteritis)
- Macular Hole / Haemorrhage
- Amaurosis Fugax (transient)
- Hysterical Blindness
🟠 GRADUAL + PAINFUL
- Dry Eye Syndrome / SPK
- Scleritis
- Chronic Uveitis
- Thyroid Eye Disease
- Subacute Optic Neuritis
🟢 GRADUAL + PAINLESS
- Cataract (most common reversible cause worldwide)
- Open-Angle Glaucoma
- Diabetic Retinopathy
- Age-Related Macular Degeneration (AMD)
- Refractive Error (most common overall)
- Retinitis Pigmentosa
- Corneal Scar / Opacity
- Optic Atrophy
Going forward - I'll use this bullet-list format under colour-coded headings instead of ASCII box tables. Much easier to read and revise from.

IMG_0207.jpg
I am sending photo of flow chart u generated I think u understand and correct yourself
I can see the problem clearly - the ASCII table is rendering as misaligned text on your screen. Understood completely. Here is the same information as a proper markdown table which renders cleanly:
QUICK MEMORY TABLE - Loss of Vision
| PAINFUL | PAINLESS | |
|---|---|---|
| SUDDEN (Acute) | Acute Angle-Closure Glaucoma | CRAO |
| Optic Neuritis | CRVO | |
| Corneal Ulcer / Abrasion | Retinal Detachment | |
| Acute Uveitis (Iritis) | Vitreous Haemorrhage | |
| Endophthalmitis | AION / GCA | |
| Corneal Hydrops | Macular Hole / Haemorrhage | |
| Amaurosis Fugax (transient) | ||
| Hysterical Blindness | ||
| GRADUAL (Chronic) | Dry Eye Syndrome / SPK | Cataract |
| Scleritis | Open-Angle Glaucoma | |
| Chronic Uveitis | Diabetic Retinopathy | |
| Thyroid Eye Disease | Age-Related Macular Degeneration | |
| Subacute Optic Neuritis | Refractive Error | |
| Retinitis Pigmentosa | ||
| Corneal Scar / Opacity | ||
| Optic Atrophy |
This is a proper markdown table - it should render as a clean grid with clear rows and columns. Going forward I will always use this format for memory tables, never ASCII boxes.
Mydriatic and miotic agents optha
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I have all the content I need. Here is the complete answer:
Mydriatic and Miotic Agents - Ophthalmology
UNDERSTANDING THE BASICS
Pupil size is controlled by two muscles:
| Muscle | Nerve | Action |
|---|---|---|
| Sphincter pupillae | Parasympathetic (CN III) | Constriction (miosis) |
| Dilator pupillae | Sympathetic | Dilation (mydriasis) |
So:
- Mydriatics = block parasympathetics (anticholinergics) OR stimulate sympathetics (adrenergics)
- Miotics = stimulate parasympathetics (cholinergics) OR block sympathetics
PART 1 - MYDRIATIC AGENTS
Mydriatics cause pupil dilation (mydriasis). They are divided into two groups:
A. Pure Mydriatics (No Cycloplegia)
These dilate the pupil WITHOUT affecting accommodation
| Drug | Class | Onset | Duration | Uses |
|---|---|---|---|---|
| Phenylephrine 2.5%, 10% | Sympathomimetic (α1 agonist) | 20 min | 3 hours | Fundus examination, breaks posterior synechiae |
- Acts on dilator pupillae muscle
- Does NOT paralyse ciliary muscle - no cycloplegia
- Preferred when dilation is needed without cycloplegia
- Contraindicated in angle-closure glaucoma
B. Cycloplegic Mydriatics (Mydriasis + Cycloplegia)
These dilate pupil AND paralyse ciliary muscle (block accommodation)
All are Anticholinergic (Antimuscarinic) agents blocking M3 receptors on sphincter pupillae and ciliary muscle.
| Drug | Concentration | Onset | Duration of Mydriasis | Cycloplegia Duration |
|---|---|---|---|---|
| Tropicamide | 0.5%, 1% | 20-30 min | 3-6 hours | ~6 hours |
| Cyclopentolate | 0.5%, 1%, 2% | 20-45 min | 24 hours | 24 hours |
| Homatropine | 2%, 5% | 20-90 min | 2-3 days | 2-3 days |
| Scopolamine (Hyoscine) | 0.25% | 20-45 min | 4-7 days | 4-7 days |
| Atropine | 0.5%, 1%, 2% | 30-40 min | 1-2 weeks | 1-2 weeks |
Key Points:
- Atropine = longest acting, strongest cycloplegic. Used for refraction in children (especially for squint/amblyopia workup). Now largely replaced by shorter-acting agents for routine dilation
- Tropicamide = most commonly used for routine fundus examination (short duration, quick recovery)
- Cyclopentolate = preferred for refraction in children (complete cycloplegia within 45 min)
- Cycloplegia = paralysis of ciliary muscle → loss of accommodation → used to measure true refractive error
Routine Dilated Exam Regimen (Wills Eye):
- Adults: Phenylephrine 2.5% + Tropicamide 1%
- Children: Above + Cyclopentolate 1-2%
- Neonates/Preterm: Lower concentrations (Phenylephrine 1%, Tropicamide 1%, Cyclopentolate 0.2-0.5%)
Clinical Uses of Cycloplegic Mydriatics:
- Fundus examination
- Refraction (especially in children - to eliminate accommodative spasm)
- Treatment of uveitis - to prevent/break posterior synechiae, relieve ciliary spasm pain
- Penalisation therapy in amblyopia (atropine to better eye)
PART 2 - MIOTIC AGENTS
Miotics cause pupil constriction (miosis). Divided into:
A. Direct-Acting Miotics (Cholinergic Agonists)
| Drug | Mechanism | Uses |
|---|---|---|
| Pilocarpine 1-4% | Muscarinic agonist (M3) | Glaucoma (open-angle + acute angle-closure), reversing mydriasis |
| Carbamylcholine (Carbachol) | Muscarinic + nicotinic agonist | Wide-angle glaucoma, intraoperative miosis |
| Aceclidine | Muscarinic agonist | Glaucoma |
Pilocarpine - Most Important Miotic:
- Acts on sphincter pupillae → miosis
- Acts on ciliary muscle → contraction → opens trabecular meshwork → increased aqueous outflow → reduced IOP
- Onset: minutes; Duration: 4-8 hours
- Drug of choice to reduce IOP emergently in both open-angle and angle-closure glaucoma
- Also used to reverse atropine-induced mydriasis
- Adverse effects: Blurred vision (especially near), night blindness (small pupil), brow ache (ciliary spasm), headache
B. Indirect-Acting Miotics (Anticholinesterase Agents)
These inhibit acetylcholinesterase → accumulation of ACh → enhanced miosis
| Drug | Type | Duration | Uses |
|---|---|---|---|
| Physostigmine (Eserine) | Reversible, carbamate | Short-acting | Glaucoma, reversal of atropine mydriasis |
| Neostigmine | Reversible | Short-acting | Rarely used topically |
| Echothiophate iodide (Phospholine iodide) | Irreversible organophosphate | Very long-acting (days-weeks) | Refractory glaucoma, accommodative esotropia in children |
| DFP (Diisopropyl fluorophosphate) | Irreversible organophosphate | Very long-acting | Rarely used now |
Echothiophate - Key Points:
- Long-acting anticholinesterase miotic
- Lowers IOP by decreasing resistance to aqueous outflow
- Used in glaucoma refractory to other therapies
- Risk: Prolongs action of succinylcholine (avoid in patients needing general anaesthesia - can cause prolonged apnoea)
QUICK MEMORY TABLE
| Mydriatics | Miotics | |
|---|---|---|
| Effect on pupil | Dilation (mydriasis) | Constriction (miosis) |
| Effect on IOP | Raises (dangerous in ACG) | Lowers |
| Mechanism | Anticholinergic / Sympathomimetic | Cholinergic / Anticholinesterase |
| Pure mydriatic | Phenylephrine | - |
| Cycloplegic mydriatics | Atropine, Scopolamine, Homatropine, Cyclopentolate, Tropicamide | - |
| Direct miotics | - | Pilocarpine, Carbachol |
| Indirect miotics | - | Physostigmine, Echothiophate |
| Shortest acting mydriatic | Tropicamide (3-6 hrs) | - |
| Longest acting mydriatic | Atropine (1-2 weeks) | - |
| Emergency glaucoma | Contraindicated | Pilocarpine (drug of choice) |
CONTRAINDICATIONS
- Mydriatics are contraindicated in angle-closure glaucoma (dilation blocks trabecular meshwork → precipitates acute attack)
- Echothiophate - avoid before general anaesthesia (prolongs succinylcholine effect)
- Darkly pigmented irides require higher concentrations or repeated dosing for adequate dilation
Sources:
- Wills Eye Manual - Mydriatic and Cycloplegic Agents table
- Lippincott Illustrated Reviews: Pharmacology - Atropine, Pilocarpine
- Goodman & Gilman's Pharmacological Basis of Therapeutics - Ophthalmic pharmacology
- Barash Clinical Anesthesia 9e - Ophthalmic agents
Causes of red eye
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I have comprehensive content. Now compiling the complete answer:
Causes of Red Eye
CLASSIFICATION
Red eye is best classified by severity and whether it is painful or painless, since pain + visual loss + pupil change = danger signs requiring urgent specialist referral.
A. PAINFUL RED EYE (Serious - Refer Urgently)
1. Acute Angle-Closure Glaucoma
- Severe ocular pain, headache, nausea/vomiting (can mimic acute abdomen)
- Hazy cornea, mid-dilated fixed oval pupil, very hard eye, poor vision
- Halos around lights
- More common in older, hypermetropic (far-sighted) patients and Asian populations
- Emergency - treat with pilocarpine, acetazolamide, mannitol → YAG laser iridotomy
2. Keratitis (Corneal Inflammation)
- Painful, photophobic, watering eye
- Herpes Simplex Keratitis - dendritic (branching) ulcer, seen on fluorescein staining. Treat with aciclovir. Steroid drops strictly contraindicated
- Bacterial Keratitis - corneal ulcer, hypopyon possible. Common in contact lens wearers
- Herpes Zoster Ophthalmicus - shingles of ophthalmic division of CN V; keratitis + uveitis
- Marginal ulceration, foreign body, abrasions
3. Anterior Uveitis (Iritis / Iridocyclitis)
- Deep aching pain, photophobia, visual blurring
- Ciliary (circumcorneal) flush - ring of injection around limbus
- Small/irregular pupil (posterior synechiae - adhesion of iris to lens)
- Keratic precipitates on corneal endothelium
- Cells and flare in anterior chamber on slit-lamp
- Associated with HLA-B27 conditions, sarcoidosis, Behçet's, TB
4. Scleritis
- Deep, severe, boring pain - worst of all red eye causes
- Tender on palpation of globe
- Deep scleral inflammation, may cause scleral thinning
- ~50% have underlying systemic disease (Rheumatoid arthritis most common)
- Treat with systemic NSAIDs or steroids
5. Endophthalmitis
- Severe pain, hypopyon, vitritis
- Usually post-operative or post-traumatic
- Ophthalmic emergency - intravitreal antibiotics
6. Corneal Foreign Body / Abrasion
- Acute onset, foreign body sensation, watering, photophobia
- Fluorescein staining shows epithelial defect
B. PAINLESS (OR MILDLY UNCOMFORTABLE) RED EYE
1. Conjunctivitis - Most Common Cause of Red Eye
| Type | Features | Discharge | Treatment |
|---|---|---|---|
| Bacterial | Gritty, bilateral (often) | Purulent / sticky | Topical broad-spectrum antibiotics |
| Viral (Adenoviral) | Watery, preauricular lymph node, one eye then other | Watery | Self-limiting, supportive |
| Chlamydial | Chronic, follicular | Mucopurulent | Systemic + topical antibiotics |
| Allergic | Itching is main symptom, bilateral, seasonal | Stringy/mucoid | Antihistamine drops, mast cell stabilisers |
| Vernal (Spring Catarrh) | Young males, bilateral, itching, cobblestone papillae under upper lid, worse spring/summer | Stringy white | Sodium cromoglicate, topical steroids |
| Giant Papillary (GPC) | Contact lens wearers, large papillae under upper lid | Mucoid | Change lens/solution, stop lens wear |
| Gonococcal | Neonates, hyperacute, profuse purulent discharge | Copious purulent | Systemic penicillin - urgent |
Key: Vision is NOT commonly affected in simple conjunctivitis. Viral conjunctivitis may occasionally cause keratitis.
2. Subconjunctival Haemorrhage
- Bright red, well-defined patch under conjunctiva
- Vision completely normal, minimal discomfort
- Causes: coughing, sneezing, straining, trauma, hypertension, anticoagulants, bleeding disorder
- Resolves spontaneously in 1-2 weeks
- Reassure patient; treat underlying cause
3. Episcleritis
- Mild-moderate discomfort, sectoral redness
- Superficial inflammation of episcleral tissue
- Often idiopathic
- Usually self-limiting; topical NSAIDs help
4. Dry Eye Syndrome
- Burning, grittiness, intermittent redness
- Worse in dry/air-conditioned environments
- Schirmer's test reduced
5. Blepharitis (Lid margin inflammation)
- Lid margin redness, crusting, scaling
- Associated conjunctival redness
- Lid hygiene + topical antibiotics
QUICK COMPARISON TABLE - Key Differentiators
| Feature | Conjunctivitis | Keratitis | Uveitis (Iritis) | Acute ACG |
|---|---|---|---|---|
| Pain | Gritty/mild | Moderate-severe | Deep aching | Severe |
| Vision | Normal | Reduced | Mildly reduced | Markedly reduced |
| Pupil | Normal | Normal | Small, irregular | Mid-dilated, fixed |
| Cornea | Clear | Hazy/ulcer | Clear (usually) | Hazy/oedematous |
| Discharge | Yes (purulent/watery) | Watering | Watering | Watering |
| IOP | Normal | Normal | Normal/low | Very HIGH |
| Redness pattern | Diffuse | Circumcorneal | Circumcorneal (ciliary flush) | Diffuse + ciliary |
| Preauricular LN | Viral - Yes | No | No | No |
MEMORY AID - Causes by Category
Conjunctival causes (most common, least serious)
- Bacterial / Viral / Allergic / Chlamydial Conjunctivitis
- Subconjunctival haemorrhage
- Episcleritis
Corneal causes
- Keratitis (HSV, bacterial, fungal, Acanthamoeba)
- Corneal abrasion / foreign body
- Corneal ulcer
Uveal causes
- Anterior uveitis (iritis)
Scleral causes
- Scleritis
Glaucoma
- Acute angle-closure glaucoma
Lid causes (secondary conjunctival redness)
- Blepharitis
- Entropion (lashes rubbing cornea)
- Ectropion (exposure keratitis)
- Stye (hordeolum) / Chalazion
Systemic / Others
- Dry eye
- Chemical / radiation injury
- Trauma
- Endophthalmitis (post-op/trauma)
Warning signs requiring immediate referral: Pain + reduced vision + abnormal pupil = serious pathology (uveitis, keratitis, acute ACG). Simple conjunctivitis and subconjunctival haemorrhage are the only self-limiting causes. All others need expert management. - Bailey & Love's Surgery, 28e
Sources:
- Bailey and Love's Short Practice of Surgery, 28e - Differential Diagnosis of the Acute Red Eye
- Wills Eye Manual - Red Eye classification
- Tintinalli's Emergency Medicine - Conjunctivitis and Eye Emergencies
- Kanski's Clinical Ophthalmology 10e
What is coloured halos Causes and tests
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I have all the information needed. Here is the complete answer:
Coloured Halos
WHAT ARE COLOURED HALOS?
Coloured halos (also written as "haloes") are rainbow-coloured rings seen around a point source of light (like a bulb, lamp, or car headlight). The patient sees a spectrum of colours - violet/blue on the inner side to red on the outer side - arranged in a ring around the light.
This happens because some opacity or water droplets within the ocular media act like a prism, diffracting white light and separating it into its component colours (just like a rainbow).
The optics: White light enters the eye → dispersed by the abnormal medium → different wavelengths (colours) are refracted at slightly different angles → forms a coloured ring around the source.
CAUSES OF COLOURED HALOS
1. Glaucoma (Most Important Cause)
Acute Angle-Closure Glaucoma - the classic and most dangerous cause
- Raised IOP causes corneal oedema (fluid accumulates in corneal stroma and epithelium)
- The oedematous cornea acts as a diffraction grating → splits white light into spectrum
- Halos appear episodically, especially at night or when IOP rises
- Associated symptoms: severe eye pain, red eye, blurred vision, nausea/vomiting, headache
- Rainbow-coloured halos around lights are a hallmark symptom
Chronic (Open-Angle) Glaucoma - may also cause halos when IOP rises episodically
2. Cataract
- Opacities in the lens scatter and diffract light
- Halos common at night (nocturnal glare / night halos)
- Typically associated with glare from oncoming headlights while driving
- Halos in cataract tend to be less colourful, more whitish/glare-type
- No pain, gradually progressive
3. Corneal Oedema (Any Cause)
- Any cause of corneal epithelial/stromal oedema produces halos
- e.g., bullous keratopathy, Fuchs endothelial dystrophy, post-surgical corneal oedema
4. Mucus/Discharge on Cornea
- Excessive mucus or discharge coating the cornea temporarily
- Halos disappear on blinking (as discharge clears)
- Seen in conjunctivitis, dry eye
5. After Refractive Surgery (LASIK/PRK)
- Multifocal ablation zones and corneal irregular astigmatism post-surgery
- Common complaint in early post-op period
6. Contact Lens Wear
- Dirty or ill-fitting contact lenses can scatter light and produce halos
7. Physiological
- Seen occasionally in normal eyes, especially in bright light causing pupil constriction around lens periphery (not pathological)
KEY DIFFERENTIATING POINT
| Feature | Glaucoma Halos | Cataract Halos |
|---|---|---|
| Colour | Bright rainbow (violet to red) | Whitish/dull glare |
| Pain | Yes (in acute ACG) | No |
| Vision | Markedly reduced | Gradually reduced |
| Time | Episodic (worse at night, with dim light) | Constant, worse at night |
| Disappear on blinking | No | No |
| Red eye | Yes (acute ACG) | No |
Important: If halos appear WITH pain, redness, and blurred vision - Acute Angle-Closure Glaucoma until proved otherwise. This is an emergency.
TESTS FOR COLOURED HALOS
1. Halo Perimetry / Halo Test (Fincham's Test)
- The most specific test for distinguishing glaucomatous halos from other causes
- Method: The patient is asked to look at a bright point source of light in a dark room. A stenopaeic slit (narrow slit) is placed before the eye and rotated:
- In glaucoma: the halo disappears at one position of the slit (because the corneal oedema is responsible and slit eliminates it at one angle) - halo breaks up with stenopaeic slit
- In cataract: the halo does NOT disappear regardless of slit position (lens opacities disperse light in all directions)
Fincham's Slit Test (also called Diffraction Test):
- Slit in front of eye rotated 360°
- Glaucoma: halo is abolished at some position → suggests corneal oedema cause
- Cataract: halo persists in all positions of the slit
2. Tonometry (IOP Measurement)
- Goldmann applanation tonometry - gold standard
- Raised IOP (>21 mmHg, often >40 mmHg in acute ACG) confirms glaucoma
- Done urgently when halos + pain present
3. Slit-Lamp Examination
- Examines cornea for oedema, Descemet's folds, bullae
- Examines anterior chamber depth (shallow = angle-closure risk)
- Examines lens for opacities (cataract)
- Cells and flare (uveitis), keratic precipitates
4. Gonioscopy
- Examines the iridocorneal angle
- Open vs closed angle - differentiates open-angle from angle-closure glaucoma
5. Visual Field Testing (Perimetry)
- Humphrey / Goldmann perimetry
- Detects characteristic field defects in glaucoma (arcuate scotoma, nasal step, tunnel vision)
6. Ophthalmoscopy / Fundus Examination
- Optic disc cupping (cup-disc ratio >0.6 suggests glaucoma)
- Retinal changes
7. Pachymetry
- Measures corneal thickness
- Corneal oedema = increased corneal thickness
MEMORY SUMMARY
| Cause | Mechanism | Key Feature |
|---|---|---|
| Acute Angle-Closure Glaucoma | Corneal oedema from raised IOP | Pain + rainbow halos + red eye - EMERGENCY |
| Cataract | Lens opacities diffracting light | Painless, night glare, progressive |
| Corneal oedema (other) | Stromal water diffraction | Depends on cause |
| Mucus on cornea | Surface irregularity | Clears on blinking |
| Post-refractive surgery | Multifocal ablation zones | Post-op history |
Most important test: Fincham's slit test - differentiates glaucoma (halo abolished by slit) from cataract (halo persists)
Sources:
- Goldman-Cecil Medicine - Halos Around Lights
- Wills Eye Manual - Acute Angle-Closure Glaucoma symptoms
- Textbook of Family Medicine - Angle-Closure Glaucoma
- Histology: Text & Atlas (Junqueira) - Glaucoma clinical correlation
- Kanski's Clinical Ophthalmology 10e
Now give me the cataract case sheet and significance of every point of history and examination and how to do examination
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Here is the complete cataract case sheet with significance of every point and how to perform each examination:
CATARACT - COMPLETE CASE SHEET
SECTION 1: HISTORY
A. PRESENTING COMPLAINTS
| Complaint | Duration |
|---|---|
| Diminution of vision | ___ months/years |
| Glare / difficulty in bright light | |
| Halos around lights | |
| Frequent change of glasses | |
| Difficulty reading / near work | |
| Double vision (uniocular diplopia) |
B. HISTORY OF PRESENTING COMPLAINTS
1. Diminution of Vision
- Onset - sudden or gradual?
- Significance: Cataract is always gradual and progressive. Sudden onset suggests other pathology (retinal detachment, vitreous haemorrhage, vascular occlusion)
- Progression - slow, moderate, fast?
- Significance: Nuclear cataract progresses slowly over years. Posterior subcapsular (PSC) progresses faster. Diabetic or steroid cataract can progress rapidly
- One eye or both?
- Significance: Age-related cataract is usually bilateral but asymmetric. Unilateral cataract in young patient suggests trauma, uveitis, or metabolic cause
- Distance vs. near vision affected?
- Significance: Nuclear sclerosis causes myopic shift → near vision may actually improve ("second sight of the aged") while distance vision deteriorates. PSC predominantly affects near vision (reading) because pupil constricts for near, exposing the opacity
2. Glare / Photophobia
- Significance: PSC cataract causes severe glare in bright light (the opacity is central, right behind the pupil). Nuclear cataract causes less glare. Cortical cataract causes glare when spokes approach the visual axis
3. Coloured Halos Around Lights
- Significance: Due to prismatic dispersion of light through opacified lens. Also seen in acute ACG (corneal oedema) - must be differentiated. In cataract: painless, chronic, no red eye
4. Uniocular Diplopia / Polyopia (seeing double/multiple images with ONE eye)
- Significance: Specific to early cataract - irregular refractive index zones within the lens create multiple images. When double vision persists on closing the other eye = lens problem
- Note: Binocular diplopia (resolves on closing one eye) = extraocular muscle/neurological cause
5. Frequent Change of Glasses ("Myopic Shift")
- Significance: Nuclear cataract increases refractive index of nucleus → lens becomes more convex → increasing myopia → patient needs stronger minus glasses or can suddenly read without spectacles ("second sight"). This is an early sign of nuclear cataract
6. Difficulty in Night Driving / Dim Light
- Significance: In dim light, pupil dilates → peripheral cortical spokes/opacities come into the visual axis → blurring
C. PAST HISTORY
| History | Significance |
|---|---|
| Diabetes mellitus | True diabetic cataract (snowflake) in young Type 1. Accelerated age-related cataract in Type 2. Also: poor surgical healing, risk of infection, may have co-existing diabetic retinopathy |
| Hypertension | Vascular risk for retinal disease; anaesthetic risk if surgery planned |
| Steroid use (topical/systemic/inhaled) | Steroids cause posterior subcapsular cataract - even inhaled steroids. Duration and dose matter |
| Trauma to the eye | Traumatic cataract - rosette-shaped, may have other ocular damage (subluxation of lens, zonule rupture, hyphema) |
| Uveitis / Iritis | Complicated cataract (posterior subcapsular) from inflammation or steroid treatment |
| Glaucoma | Associated condition; may affect surgery planning; visual prognosis guarded |
| Previous eye surgery | Aphakic/pseudophakic status, previous retinal surgery |
| Systemic diseases | Hypothyroidism, myotonic dystrophy, atopic dermatitis, Marfan syndrome, homocystinuria - all cause early cataract |
| Radiation exposure | Posterior subcapsular cataract (classic after radiotherapy to head/neck) |
D. FAMILY HISTORY
- Significance: Hereditary/congenital cataract in relatives. Familial tendency in age-related cataract also exists
E. DRUG HISTORY
- Steroids (topical/systemic/inhaled) → PSC cataract
- Chlorpromazine → anterior subcapsular stellate deposits
- Amiodarone → anterior subcapsular deposits
- Miotics (long-term pilocarpine/echothiophate) → anterior subcapsular cataract
- Allopurinol → nuclear cataract
F. PERSONAL HISTORY
- Occupation: Significance: Glass blowers, furnace workers → heat-induced (infrared) cataract (posterior subcapsular)
- Smoking: associated with nuclear and posterior subcapsular cataract
- Prolonged UV exposure (outdoor workers)
SECTION 2: GENERAL PHYSICAL EXAMINATION
| Examination | What to Look For | Significance |
|---|---|---|
| Built, nutrition | General systemic health | Surgical fitness |
| Pulse, BP | Hypertension, cardiac status | Anaesthetic risk |
| Blood sugar | Diabetes control | Surgical risk, healing, retinopathy risk |
| Thyroid | Hypothyroidism | Cause of cataract |
| Skin | Atopic dermatitis | Atopic cataract (anterior subcapsular, "shield cataract") |
| Face/body | Marfan, homocystinuria habitus | Subluxated lens |
| Facial nerve | CN VII palsy | Inability to close eye post-op (exposure keratitis) |
SECTION 3: OPHTHALMIC EXAMINATION
(Examine both eyes - always compare)
A. VISUAL ACUITY (VA) - Most Important
How to do it:
- Test each eye separately (cover the other eye with an occluder)
- Use Snellen's chart at 6 metres in good illumination
- Ask patient to read smallest line they can
- Record as 6/6, 6/9, 6/12... down to 6/60
- If cannot read top letter (6/60): test at 3 metres → record as 3/60
- If cannot read at 3m: count fingers → "CF" at ___ metres
- If cannot count fingers: hand movements → "HM"
- If no HM: light perception → "PL" (test with torch)
- If no light perception: "NPL"
- Then test with pinhole: if VA improves with pinhole → refractive error component; if no improvement → suggests media opacity or macular disease
Significance:
- Establishes baseline VA and surgical indication
- Near VA (N notation, Jaeger chart): PSC and nuclear cataracts affect near/distance differently
- Pinhole test: In cataract, pinhole usually improves VA (reduces scatter from peripheral lens)
- Glare testing: Check VA in bright illumination - in PSC and cortical cataract, VA drops dramatically in bright light (glare disability)
B. TORCH EXAMINATION (External Eye)
| Step | What to See | Method | Significance |
|---|---|---|---|
| Lids | Ptosis, entropion, ectropion, blepharitis | Inspect with torch | Blepharitis → infection risk post-op; ectropion → exposure; ptosis may mask vision improvement post-op |
| Lacrimal sac | Regurgitation on pressure (ROPLAS) | Press over medial canthus | Active dacryocystitis = contraindication to surgery (infection risk → endophthalmitis) |
| Conjunctiva | Redness, follicles, discharge | Inspect | Active conjunctivitis = contraindicate surgery |
| Cornea | Clarity, scars, size, sensation | Torch; touch cotton wisp for sensation | Corneal disease affects prognosis; scarring affects visual outcome |
| Anterior chamber depth | Shallow/normal/deep | Oblique torch from side | Shallow AC → risk of ACG; important for IOL power |
| Iris | Rubeosis (new vessels), iritis signs, coloboma | Inspect | Rubeosis → vascular disease (diabetic/CRVO); iritis → complicated cataract |
| Pupil | Shape, size, reactions | Direct + consensual light reflex | RAPD (afferent pupillary defect) → optic nerve or retinal disease; may limit visual prognosis post-op |
C. OBLIQUE ILLUMINATION TEST (Torch Test for Cataract)
How to do it:
- Seat patient in a slightly darkened room
- Hold torch at 45° to the optical axis from the lateral side
- Shine light into the eye from the side
- Look at the lens through the pupil
What you see:
- Immature cataract: The iris casts a crescent-shaped shadow on the lens (iris shadow) because the opacity has not reached the anterior surface - called "iris shadow present" / positive iris shadow sign
- Mature cataract: Lens is completely opaque, opacity reaches the front - no iris shadow (negative iris shadow)
- Hypermature cataract: Wrinkled capsule, milky/pearly white appearance
Significance:
- Quick bedside test to roughly stage cataract maturity
- Positive iris shadow = immature (not yet mature)
- Negative iris shadow = mature cataract
D. DISTANT DIRECT OPHTHALMOSCOPY - RED REFLEX TEST
How to do it:
- Set ophthalmoscope to +10 dioptre (convex lens, for initial view)
- Keep at arm's length (~30 cm) from patient
- Look through the ophthalmoscope in a dimly lit room (pupil slightly dilated)
- Direct light into the patient's pupil
- Observe the red reflex (orange-red glow from fundus)
What you see:
- Normal: Bright orange-red reflex (like red-eye in photographs)
- Cataract: Black/dark opacities against the red reflex
- Nuclear cataract: central dark shadow
- Cortical: spoke-like dark shadows at periphery
- PSC: central dark shadow
- Mature cataract: Absent red reflex (no fundal glow visible)
Significance:
- Identifies presence and approximate location of lens opacity
- Absent red reflex = mature/dense cataract OR fundal pathology
- Grading: Can roughly estimate density
E. SLIT LAMP BIOMICROSCOPY - Most Detailed
How to do it:
- Patient sits at the slit lamp, chin on chin-rest, forehead against bar
- Align the eye level
- Start with broad beam, medium magnification
- Examine in sequence: lids → conjunctiva → cornea → anterior chamber → iris → lens
For Lens Examination:
- Use a narrow beam at 45° to the eye
- Scan from anterior capsule to posterior capsule
- The slit beam shows the layers as bright sections: anterior capsule → anterior cortex → nucleus → posterior cortex → posterior capsule
What to look for in lens:
| Location | Finding | Type of Cataract |
|---|---|---|
| Nucleus (centre, bright section) | Brown/yellow/amber discolouration | Nuclear sclerosis (graded 1-4+) |
| Cortex (peripheral zones) | Spoke-like / wedge-shaped opacities radiating from equator | Cortical cataract |
| Posterior subcapsular (just in front of posterior capsule) | Granular/bread-crumb opacities, best seen with retroillumination | PSC cataract |
| Anterior capsule | Stellate/rosette pattern | Traumatic or steroid-induced |
| Whole lens | Complete white opacity | Mature cataract |
Retroillumination technique (for PSC):
- Use the fundal red reflex as a backlight
- PSC appears as dark granular opacity against the red background - most sensitive method
LOCS III Grading (Lens Opacification Classification System):
- Nuclear Colour (NC): 1-6
- Nuclear Opalescence (NO): 1-6
- Cortical (C): 1-5
- Posterior Subcapsular (P): 1-5
F. PUPIL REACTIONS
| Test | Method | Significance |
|---|---|---|
| Direct light reflex | Shine torch in eye, observe same eye constricting | Tests optic nerve + CN III |
| Consensual reflex | Shine in one eye, observe other eye | Confirms reflex arc |
| RAPD (Swinging flashlight test) | Swing torch quickly between eyes, observe dilation when light reaches that eye | RAPD = optic nerve or extensive retinal disease in that eye → poor visual prognosis post-surgery even if cataract removed |
G. EXTRAOCULAR MOVEMENTS (EOM)
- How: Ask patient to follow your finger in H-pattern
- Significance: Pre-existing strabismus (squint) → amblyopia in that eye → limited visual recovery post-cataract surgery
H. INTRAOCULAR PRESSURE (IOP)
How to do it (Goldmann Applanation Tonometry):
- Instil local anaesthetic + fluorescein drops
- Apply blue cobalt light at slit lamp
- Place applanation head on cornea
- Adjust dial until two green semi-circles meet
- Read IOP from the dial (multiply by 10 → mmHg)
Normal: 10-21 mmHg
Significance:
- Raised IOP → glaucoma (may co-exist with cataract)
- Phacomorphic glaucoma - intumescent (swollen) lens pushing iris forward → raised IOP
- Phacolytic glaucoma - protein leaking from hypermature cataract blocking trabecular meshwork → raised IOP
- Low IOP → uveitis, retinal detachment (check for other pathology)
I. FUNDUS EXAMINATION
How to do it:
- Dilate pupil (Tropicamide 1% + Phenylephrine 2.5%, wait 20-30 min)
- Use direct ophthalmoscope (+2D for normal emmetrope) or slit lamp with +90D/+78D lens
- Examine: disc, vessels, macula, periphery
Significance:
- Must be done before deciding on surgery
- Optic disc cupping → glaucoma (may limit visual prognosis)
- Macular degeneration, diabetic maculopathy, epiretinal membrane → visual prognosis is limited even after successful cataract surgery
- If fundus not visible due to dense cataract → B-scan ultrasonography to rule out retinal detachment, vitreous haemorrhage, intraocular tumour
SECTION 4: SPECIAL INVESTIGATIONS (Pre-Surgical Workup)
| Investigation | How Done | Significance |
|---|---|---|
| Keratometry (K-readings) | Measures corneal curvature | Required for IOL power calculation |
| Axial Length (A-scan biometry) | Ultrasound probe on cornea; measures length of eyeball | Required for IOL power calculation |
| IOL Power Calculation | SRK-II / SRK-T formula using K-readings + axial length | Determines which IOL lens power to implant |
| Specular Microscopy | Counts corneal endothelial cells | <1000 cells/mm² → high risk of corneal decompensation post-surgery |
| B-scan Ultrasound | When fundus not visible | Rules out retinal detachment, vitreous pathology, intraocular tumour |
| Visual Evoked Potential (VEP) | Electrical response to light | Assesses optic nerve function when fundus not visible |
| Potential Acuity Meter (PAM) | Laser/pinhole through cataract to project chart on retina | Predicts post-operative visual acuity |
| Entoptic Phenomenon | Patient sees own retinal vessels with moving light | Tests macular function through dense cataract |
| Colour Vision | Ishihara plates | Optic nerve disease? |
| Visual Fields | Confrontation / perimetry | Glaucomatous field defects |
SECTION 5: TYPES OF AGE-RELATED CATARACT - Quick Reference
| Type | Location | Symptoms | Slit Lamp | Red Reflex |
|---|---|---|---|---|
| Nuclear sclerosis | Central nucleus | Distance blur, myopic shift, "second sight" | Brown/yellow nucleus | Dark centre |
| Cortical | Cortex, spokes | Glare, worse in bright light | Spoke-like opacities from periphery | Dark spokes |
| Posterior Subcapsular (PSC) | Just anterior to posterior capsule | Near vision blur, severe glare, affects young more | Granular opacity, best on retroillumination | Central dark patch |
| Mature | Entire lens | Severe vision loss (perception of light) | Uniformly white lens, no iris shadow | Absent |
| Hypermature | Cortex liquefied | PL/NPL, wrinkled capsule | Morgagnian (nucleus sinks), milky lens | Absent |
SECTION 6: DIAGNOSIS STATEMENT
Standard format:
"Mr/Ms _____, aged _____ years, presenting with gradual, painless, progressive diminution of vision in the right/left/both eyes for ___ months, is a case of immature/mature senile cataract of the nuclear/cortical/PSC type in the right/left eye, with no significant co-morbidities, fit for phacoemulsification with IOL implantation under topical/peribulbar/general anaesthesia."
Sources:
- Wills Eye Manual - Cataract workup, types, examination
- Goldman-Cecil Medicine - Cataract clinical features
- Pfenninger & Fowler's Procedures for Primary Care - Slit lamp lens examination technique
- Kanski's Clinical Ophthalmology 10e - Cataract classification
This is a shared conversation. Sign in to Orris to start your own chat.