Effect of increasing glucose on all the ions like na ,k,calcium etc
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, well-sourced information from multiple authoritative textbooks. Here is the full answer:
Effect of Increasing Glucose (Hyperglycemia) on Electrolytes
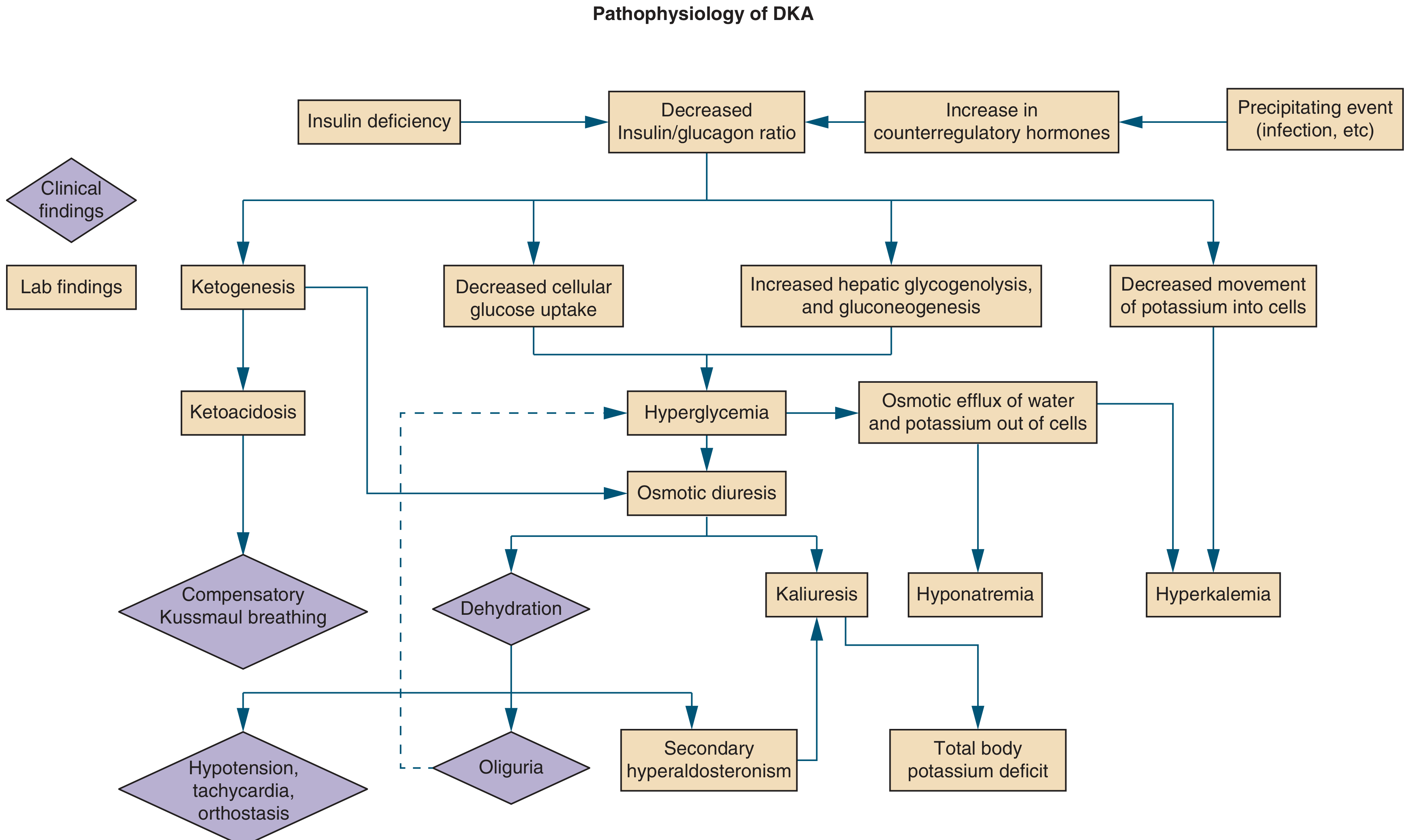
Hyperglycemia affects every major electrolyte through two primary mechanisms: osmotic shifts (glucose is an effective osmol that draws water out of cells) and osmotic diuresis (glycosuria pulls electrolytes into the urine). The classic context is DKA or HHS, but these effects apply any time blood glucose rises significantly.
1. Sodium (Na+)
Serum level: Appears LOW (pseudohyponatremia / dilutional hyponatremia)
- Glucose is an effective osmol restricted mostly to the extracellular space (ECF) - it does not freely enter muscle cells without insulin.
- High glucose raises ECF osmolality, pulling water out of cells into the ECF, which dilutes serum Na+.
- For every 100 mg/dL rise in glucose above 100 mg/dL, serum Na+ falls by approximately 2.4 mEq/L (older teaching used 1.6, but 2.4 is the more accurate correction factor, especially at glucose >400 mg/dL).
- Correction formula: Corrected Na+ = Measured Na+ + 2.4 × [(Glucose - 100)/100]
- Simultaneously, osmotic diuresis (glycosuria) causes renal losses of NaCl, worsening true sodium depletion.
- ADH is also stimulated by the high osmolality, causing water retention which further dilutes sodium.
- With treatment (insulin + fluids), glucose falls, water shifts back intracellularly, and serum Na+ rises - it can overshoot into hypernatremia if fluids are not replaced adequately.
- Henry's Clinical Diagnosis and Management by Laboratory Methods, Effect of Hyperglycemia on Serum Na+
- Tintinalli's Emergency Medicine, Sodium and Other Electrolytes (DKA chapter)
- Symptom to Diagnosis, 4th Ed.
2. Potassium (K+)
Serum level: ELEVATED (despite total body deficit)
This is perhaps the most clinically dangerous electrolyte change in hyperglycemia:
| Mechanism | Effect on serum K+ |
|---|---|
| Insulin deficiency - less K+ driven into cells | Raises serum K+ |
| Hypertonicity (osmotic efflux) - water and K+ exit cells together | Raises serum K+ |
| Metabolic acidosis (H+/K+ exchange across cell membrane) | Raises serum K+ |
| Osmotic diuresis (kaliuresis) | Depletes total body K+ |
| Secondary hyperaldosteronism (from volume depletion) | Increases renal K+ loss |
- At presentation: serum K+ is normal or high in most DKA patients (4-6% present with hypokalemia).
- Total body K+ is significantly depleted despite normal/high serum levels.
- With insulin therapy: K+ shifts back into cells rapidly - serum K+ drops ~1.5 mEq/L and parallels the drop in glucose.
- This is why K+ must be monitored closely and repleted during insulin therapy.
- Tintinalli's Emergency Medicine, Potassium section
- Symptom to Diagnosis, 4th Ed., DKA chapter
3. Phosphate (PO4³-)
Serum level: Initially ELEVATED or normal → drops with treatment
- Osmotic diuresis causes significant renal phosphate wasting, depleting total body phosphate.
- Insulin deficiency and hyperosmolarity shift phosphate from cells to ECF, so serum levels at presentation may be normal or elevated.
- With insulin treatment, phosphate is driven back into cells, and serum phosphate can fall dramatically (hypophosphatemia).
- Severe hypophosphatemia can impair respiratory muscle function, cardiac function, and oxygen delivery (reduced 2,3-DPG in red blood cells).
- Tintinalli's Emergency Medicine: "Osmotic diuresis also causes urinary losses and total-body depletion of phosphorous, calcium, and magnesium. Hemoconcentration frequently leads to initially elevated levels of these electrolytes in serum. As therapy progresses, lower serum levels of each will be evident."
4. Magnesium (Mg²+)
Serum level: Initially normal/elevated → falls with treatment
- Same pattern as phosphate: osmotic diuresis causes renal wasting of magnesium.
- At presentation, hemoconcentration (from dehydration) can mask the deficit, making serum Mg²+ appear normal or high.
- With fluid therapy and insulin, hypomagnesemia becomes apparent.
- Hypomagnesemia exacerbates hypokalemia (makes it refractory to treatment) and raises the risk of cardiac arrhythmias.
- Acidosis and hyperosmolarity shift Mg²+ out of cells as well.
- Tintinalli's Emergency Medicine, Sodium and Other Electrolytes
- Rosen's Emergency Medicine (related table)
5. Calcium (Ca²+)
Serum level: Variably affected - usually normal at presentation, may fall with treatment
- Like phosphate and magnesium, osmotic diuresis causes some renal calcium loss.
- Hemoconcentration at presentation can initially mask this.
- Metabolic acidosis increases ionized calcium (H+ competes with Ca²+ for albumin binding), so ionized Ca²+ may actually be higher initially.
- As acidosis corrects with treatment, ionized Ca²+ can drop.
- Clinically significant hypocalcemia in DKA/HHS is less common than hypokalemia/hypophosphatemia but should be monitored.
6. Chloride (Cl-) and Bicarbonate (HCO3-)
- Chloride: Lost through osmotic diuresis alongside sodium. In hyperchloremic non-anion gap acidosis (after saline resuscitation), Cl- rises.
- Bicarbonate: Falls due to the metabolic acidosis from ketones (DKA) or lactic acid. HCO3- ≤ 18 mEq/L is a diagnostic criterion for DKA.
Summary Table
| Ion | Serum Level at Presentation | Total Body | Key Mechanism |
|---|---|---|---|
| Na+ | LOW (dilutional) | Depleted | Osmotic dilution + osmotic diuresis |
| K+ | NORMAL/HIGH | Depleted | Osmotic efflux + acidosis shift; masked deficit |
| PO4³- | Normal/High → drops | Depleted | Osmotic diuresis; shifts with insulin |
| Mg²+ | Normal/High → drops | Depleted | Osmotic diuresis; hemoconcentration masks |
| Ca²+ | Normal | Mildly depleted | Osmotic diuresis; acidosis effect on ionized Ca |
| HCO3- | LOW | Depleted | Metabolic acidosis from ketones |
| Cl- | Variable | Depleted | Osmotic diuresis; rises with saline therapy |
Key clinical takeaways:
- The serum K+ is the most dangerous - it is high (or normal) at presentation but total body K+ is depleted, and insulin therapy will crash the serum level. Always check ECG and replace K+ before/alongside insulin if serum K+ <3.5 mEq/L.
- Correct serum Na+ for glucose before interpreting hyponatremia (add 2.4 per each 100 mg/dL glucose above 100).
- Phosphate and magnesium need to be monitored and replaced as treatment progresses.
This is a shared conversation. Sign in to Orris to start your own chat.