When to say clcd is decompensated
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
I now have everything needed for a comprehensive answer. Here it is:
When is Chronic Liver Disease (CLCD) Called Decompensated?
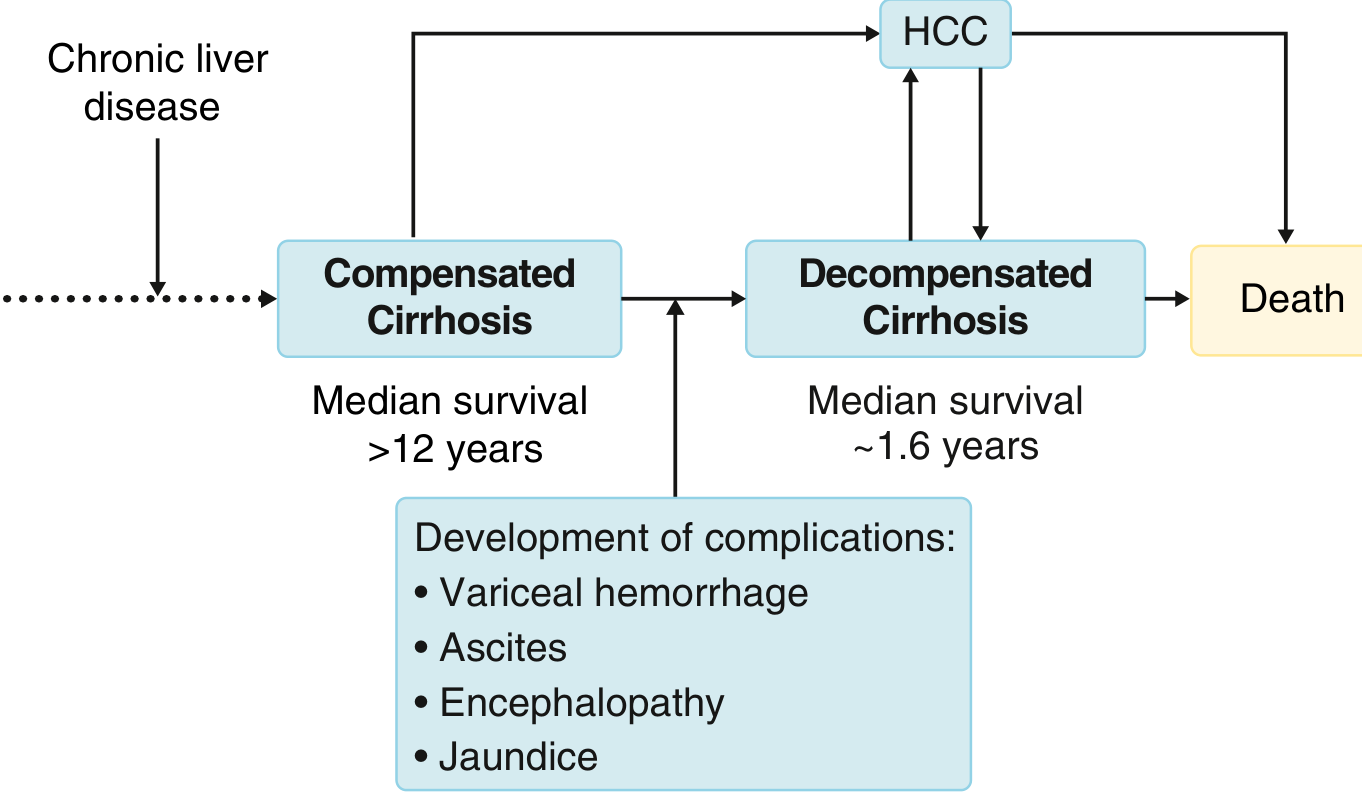
Chronic liver disease progresses through two main phases - compensated and decompensated cirrhosis. The transition is defined by the first appearance of any major clinical complication reflecting either portal hypertension or liver synthetic failure.
The Four Cardinal Signs of Decompensation
CLCD (cirrhosis) is called decompensated when any one or more of the following develop:
| Feature | Key Points |
|---|---|
| Ascites | Most common sign - present in 80% of decompensated cases; fluid accumulation from portal hypertension + hypoalbuminemia |
| Variceal Hemorrhage | Hematemesis/melena from gastroesophageal varices; medium/large varices bleed at ~15%/year |
| Hepatic Encephalopathy | Brain dysfunction from liver insufficiency + portosystemic shunting; ammonia is the key toxin |
| Jaundice | Inability to excrete bilirubin; reflects liver insufficiency |
Note: The presence of varices without bleeding does NOT constitute decompensation - it is still considered compensated stage 2.
The 4-Stage Clinical Classification (Sleisenger & Fordtran)
| Stage | Features | Phase |
|---|---|---|
| Stage 1 | No ascites, no varices | Compensated |
| Stage 2 | Varices present, no bleeding, no ascites | Compensated |
| Stage 3 | Ascites (with or without varices) | Decompensated |
| Stage 4 | Variceal bleeding (with or without ascites) | Decompensated |
Stages 3 and 4 = decompensated cirrhosis.
Why Does Decompensation Occur?
As disease progresses, two mechanisms drive decompensation:
- Portal hypertension worsens - portal pressure rises above threshold, leading to varices, ascites, and portosystemic shunting (encephalopathy)
- Liver synthetic function fails - reduced albumin, coagulation factors, and impaired bilirubin excretion
The transition from compensated to decompensated occurs at a rate of ~5-7% per year, with a median time to first decompensation of ~6 years from the compensated stage.
Prognosis Implications
| Phase | Median Survival |
|---|---|
| Compensated cirrhosis | >12 years |
| Decompensated cirrhosis | ~1.6-2 years |
Decompensated patients have a 10-fold increased mortality risk compared to the general population (vs. 5-fold for compensated).
Additional Complications That Worsen Prognosis Further
Once decompensated, additional complications signal further deterioration:
- Refractory ascites - ascites unresponsive to diuretics
- Hepatorenal syndrome (HRS) - functional renal failure
- Spontaneous bacterial peritonitis (SBP) - infected ascitic fluid
- Hepatopulmonary syndrome - arterial hypoxemia from pulmonary vasodilation
- Portopulmonary hypertension - pulmonary vascular disease
- Hepatocellular carcinoma (HCC) - can develop at any stage and precipitate decompensation
Infection is now recognized as a distinct stage in the natural history, associated with poor survival even after clearance.
Acute-on-Chronic Liver Failure (ACLF) - Beyond Decompensation
ACLF is a separate, more severe entity where a precipitating event (e.g., infection, alcoholic hepatitis, viral reactivation) leads to multi-organ failure on top of chronic liver disease. It carries a significantly higher short-term mortality than simple decompensation.
Sources: Goldman-Cecil Medicine, 26th ed., Ch. 139 | Sleisenger & Fordtran's GI and Liver Disease, Ch. 74
Thanks
You're welcome! Feel free to ask anytime. 😊
This is a shared conversation. Sign in to Orris to start your own chat.