
eeec8752-c67f-4585-b854-a9fb04d3ca58.png
Decipher how shud I look and interpret thismlead serially
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Now I have everything I need. Let me provide a complete, detailed analysis.
ECG Analysis - Full 12-Lead Interpretation
Settings confirmed
- Speed: 25 mm/sec | Gain: 1 cm/mV (standard)
Step-by-Step Lead-by-Lead Breakdown
RHYTHM (Lead II rhythm strip - bottom row)
- Regular rhythm, narrow QRS
- Rate: approximately 75-80 bpm
- P waves present and upright in II - normal sinus rhythm
SYSTEMATIC LEAD ANALYSIS
Limb Leads
| Lead | P wave | Q wave | ST segment | T wave |
|---|---|---|---|---|
| I | Upright | Absent/small | Isoelectric | Upright, small |
| II | Upright, tall | Deep Q wave present | Appears isoelectric or minimally elevated | T wave upright |
| III | Upright | Deep, wide Q wave | Mildly elevated or at baseline | T wave upright or biphasic |
| aVR | Inverted | - | ST depression (reciprocal) | Inverted T |
| aVL | Upright | Small Q or absent | ST depression (reciprocal) | T wave inverted/flattened |
| aVF | Upright | Deep Q wave | ST mildly elevated/isoelectric | T wave upright |
Key finding in limb leads: Deep, wide Q waves in II, III, and aVF with reciprocal ST changes in aVL. This is the hallmark pattern.
Precordial Leads
| Lead | Q wave | R wave | ST segment | T wave |
|---|---|---|---|---|
| V1 | QS pattern | Poor R | Isoelectric | Biphasic/flat |
| V2 | QS pattern | Small R | Mildly elevated | Deep T inversion |
| V3 | Small Q | Transitional | Elevated | Deep T inversion |
| V4 | Absent | Tall R | Isoelectric to slightly elevated | Upright |
| V5 | Absent | Tall R | Isoelectric | Upright |
| V6 | Absent | Tall R | Isoelectric | Upright |
Key finding in precordial leads:
- Deep T-wave inversions in V2-V3 (anterior leads)
- Possible residual ST elevation in V2-V3 zone
- R-wave progression preserved by V4-V6
- No dominant R in V1 to suggest true posterior MI
THE MAIN DIAGNOSIS
Evolving/Evolved Inferior STEMI with possible anterior extension
This ECG pattern is classic for Inferior ST-Elevation MI (STEMI) - in an evolving or post-acute phase. Here's the temporal staging:
How to Read This SERIALLY (ECG Evolution Over Time)
This is the most important part of your question. Inferior STEMI evolves through 4 phases:
Phase 1 - Hyperacute (0 to ~2 hours)
- Tall, "hyperacute" T waves in II, III, aVF (may be taller than normal)
- ST segments just beginning to elevate
- No Q waves yet
- Reciprocal ST depression begins in aVL and I
Phase 2 - Acute STEMI (2-12 hours)
- ST elevation in II, III, aVF - tombstone or convex morphology
- ST depression in aVL (reciprocal) - this is diagnostically very helpful
- Q waves beginning to appear in II, III, aVF
- T waves may still be upright
Phase 3 - Evolving (12-72 hours) - This ECG is likely here
- ST elevation is resolving back toward baseline
- Deep Q waves now established in II, III, aVF - these are pathological (>1 small square wide and >1/4 of R height)
- T wave inversion appearing in II, III, aVF - this represents ongoing reperfusion/healing
- Precordial T inversions in V2-V3 suggest extension or reciprocal changes
Phase 4 - Chronic/Old MI (days to months)
- ST fully returns to baseline
- Q waves persist (permanent scar)
- T waves may normalize or remain inverted
- R-wave amplitude may be permanently reduced
Comparing Your ECG to the Textbook Pattern
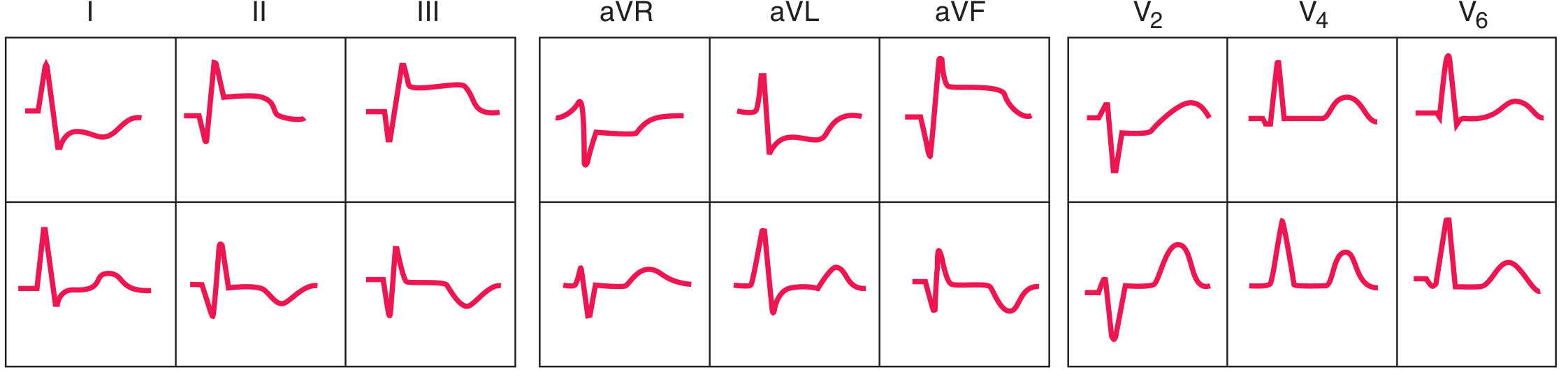
The textbook diagram above (from Harrison's, 22nd Edition, Fig. 247-13) shows exactly this: acute inferior STEMI (top row) vs evolved inferior STEMI (bottom row) - with Q waves deepening and T inversion appearing as the ECG evolves over time. Your ECG closely matches the evolving/evolved phase in the bottom row.
Summary of Abnormal Findings in Your ECG
- Pathological Q waves in II, III, aVF - indicating inferior wall necrosis
- Residual/resolving ST changes in inferior leads - suggests sub-acute phase
- Reciprocal changes in aVL (ST depression, T inversion) - confirms infero-lateral territory
- T-wave inversions in V2-V3 - may represent anterior extension or reciprocal anterior changes; also could indicate RV involvement or proximal RCA occlusion
- Normal R-wave progression V4-V6 - lateral wall spared
Territory and Likely Culprit Vessel
| Finding | Implication |
|---|---|
| Inferior Q waves (II, III, aVF) | RCA (right coronary artery) in ~80% of cases |
| ST changes also in V1-V3 | Consider proximal RCA (with RV involvement) or co-existing posterior MI |
| Reciprocal aVL changes | Confirms inferior MI, not pericarditis |
- Source: Harrison's Principles of Internal Medicine, 22E, Chapter 247 (ECG section on Myocardial Ischemia and Infarction)
How to Approach Serial ECGs in Practice
When reviewing serial ECGs in this patient, look for:
- ST elevation trending down over time (good sign - reperfusion occurring)
- Q waves deepening or persisting - indicates permanent scar
- T-wave inversion evolving - normal part of healing
- New ST re-elevation - danger sign (re-occlusion or aneurysm formation)
- Arrhythmias developing - look for VPBs, VT, heart block (common with inferior MI)
- PR interval - inferior MI can damage the AV node (supplied by RCA), so watch for 1st, 2nd, or 3rd degree AV block serially
Clinical note: This ECG does not represent an acute STEMI requiring immediate cath lab activation - the ST elevation has resolved and Q waves with T inversions are present. It represents a sub-acute or evolving inferior MI, most likely 24-72 hours old. Always correlate with troponin trend and clinical history.
This is a shared conversation. Sign in to Orris to start your own chat.