Ecg
Asking for Preferences
Reading File
Finding Sources
Searching the Web
how to read ECG systematically step by step 2024
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Excellent - I now have all the key diagrams and content. Let me compile a complete, well-structured guide.
ECG (Electrocardiogram) - A Complete Beginner's Guide
Source: Harrison's Principles of Internal Medicine, 22nd Edition (2025)
What Is an ECG?
An electrocardiogram records the electrical activity of the heart from electrodes placed on the skin. Each lead is like a different camera angle looking at the same events - atrial and ventricular depolarization and repolarization - from different spatial orientations.
The 12 Leads
A standard ECG has 12 leads:
- 6 limb leads (I, II, III, aVR, aVL, aVF) - record potentials in the frontal plane
- 6 precordial (chest) leads (V1-V6) - record potentials in the horizontal plane
Precordial Electrode Placement
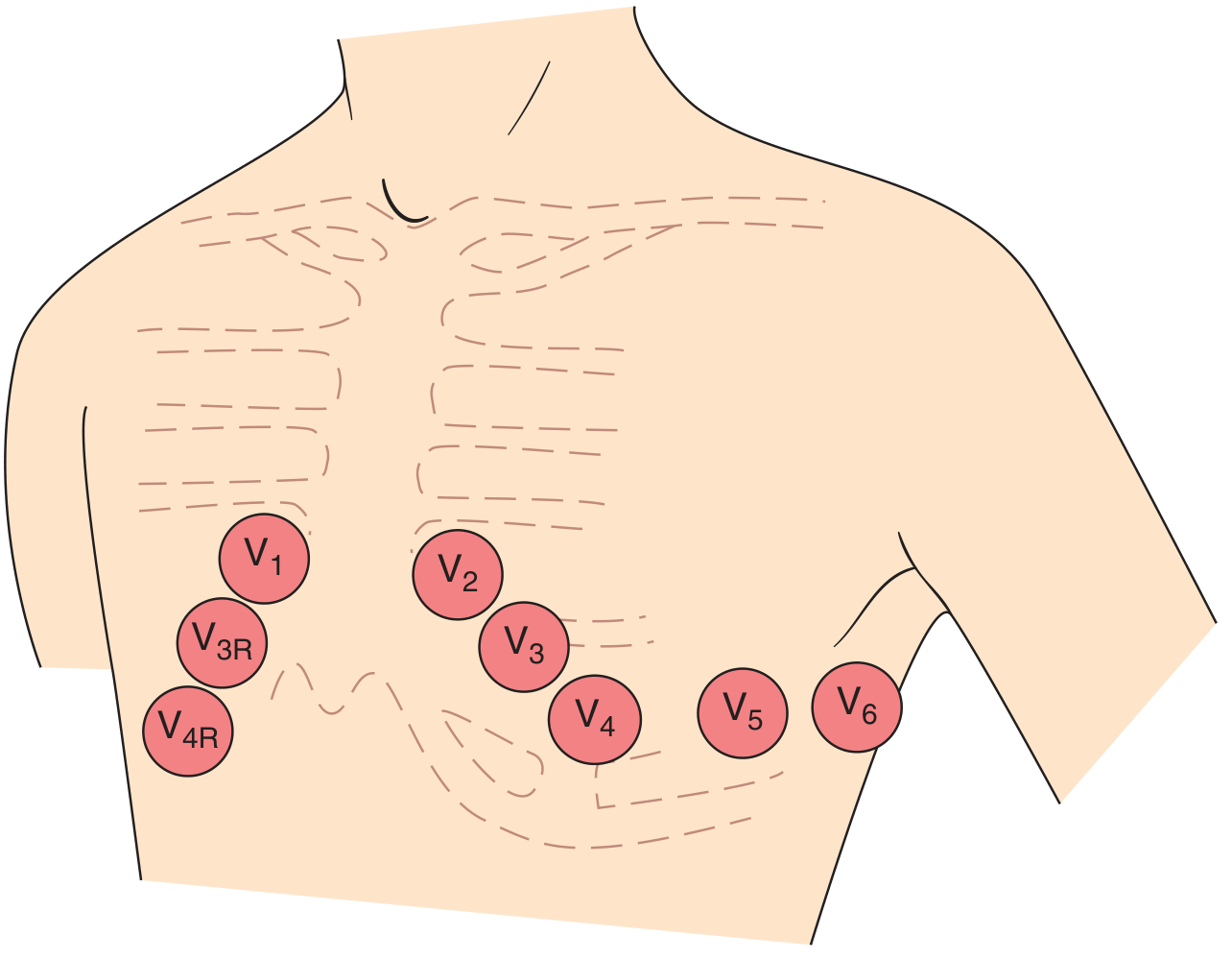
| Lead | Position |
|---|---|
| V1 | 4th intercostal space, right sternal border |
| V2 | 4th intercostal space, left sternal border |
| V3 | Between V2 and V4 |
| V4 | 5th intercostal space, midclavicular line |
| V5 | Anterior axillary line (same level as V4) |
| V6 | Midaxillary line (same level as V4) |
The Normal ECG Waveforms
Each cardiac cycle on the ECG consists of:
| Wave/Interval | Represents | Normal Duration |
|---|---|---|
| P wave | Atrial depolarization (SA node fires, atria contract) | <120 ms (<3 small squares) |
| PR interval | Time from atrial to ventricular depolarization (AV node delay) | 120-200 ms (3-5 small squares) |
| QRS complex | Ventricular depolarization (ventricles contract) | <120 ms (<3 small squares) |
| ST segment | Early ventricular repolarization (isoelectric) | Should be at baseline |
| T wave | Ventricular repolarization | Upright in most leads |
| QT interval | Total ventricular electrical activity (QRS + ST + T) | <440 ms (men), <460 ms (women) |
| U wave | Thought to reflect Purkinje fiber repolarization | Small, follows T wave |
ECG Paper Speed and Grid
- Each small square = 0.04 seconds (horizontal) and 0.1 mV (vertical)
- Each large square = 0.20 seconds (5 small squares)
The P Wave - Atrial Depolarization
The normal atrial depolarization vector is oriented downward and to the left (from the sinus node toward the AV node). This means:
- P wave is positive in lead II and negative in lead aVR - this confirms sinus rhythm
- In V1, the P wave may be biphasic: positive component (right atrium) then small negative component (left atrium)
An ectopic atrial pacemaker in the lower atrium or AV junction produces retrograde P waves (negative in II, positive in aVR).
The QRS Complex - Ventricular Depolarization
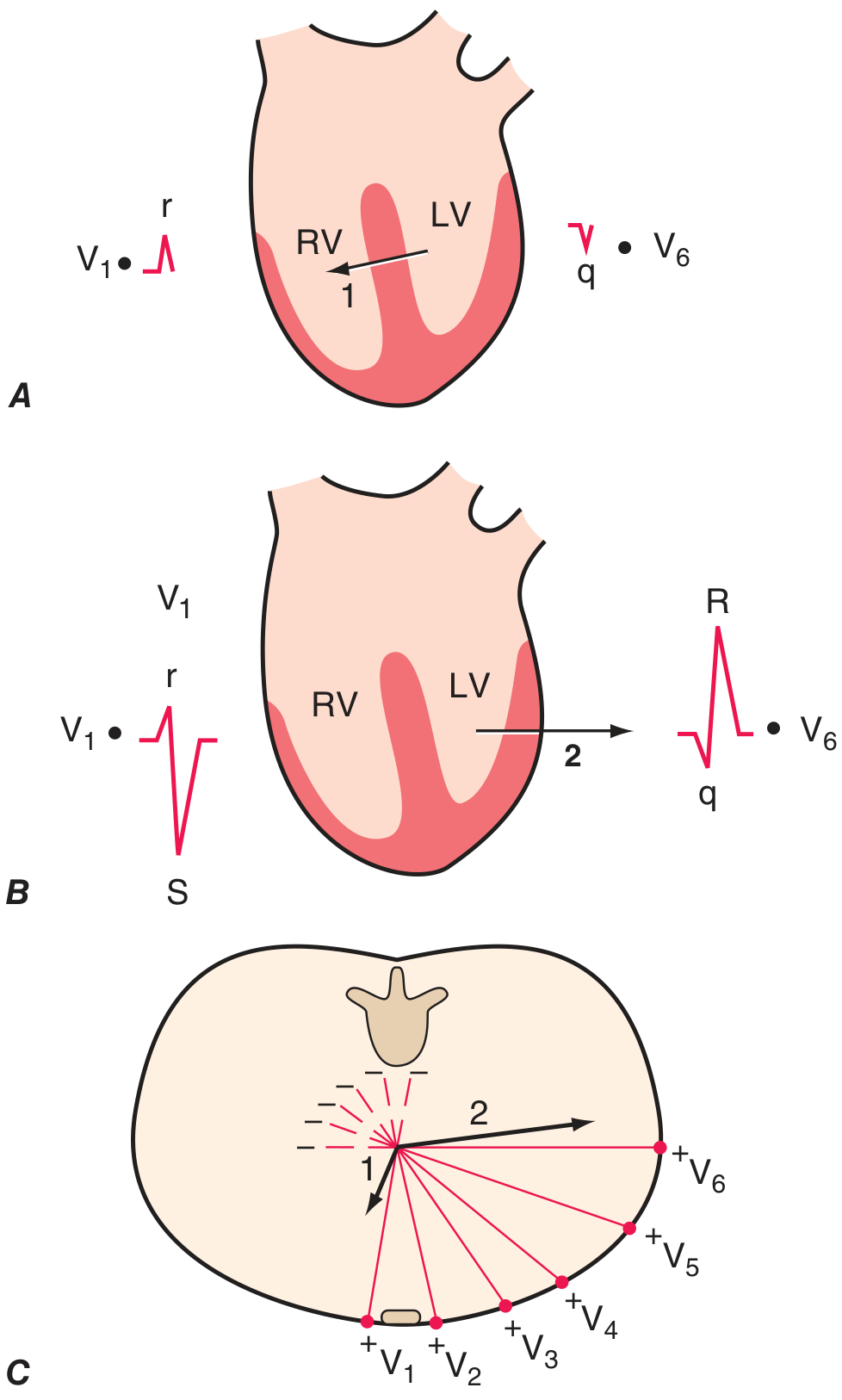
Ventricular depolarization has two main phases:
- Phase 1 - Septal depolarization: Left to right, produces a small r wave in V1 and small septal q wave in V6
- Phase 2 - Ventricular depolarization: The dominant left ventricle pulls the vector leftward and posteriorly, producing a large S wave in V1 and tall R wave in V6
This explains normal R-wave progression across the chest leads - R waves get taller from V1 to V5, and S waves decrease. The transition zone (where R=S) is normally at V3-V4.
QRS Axis
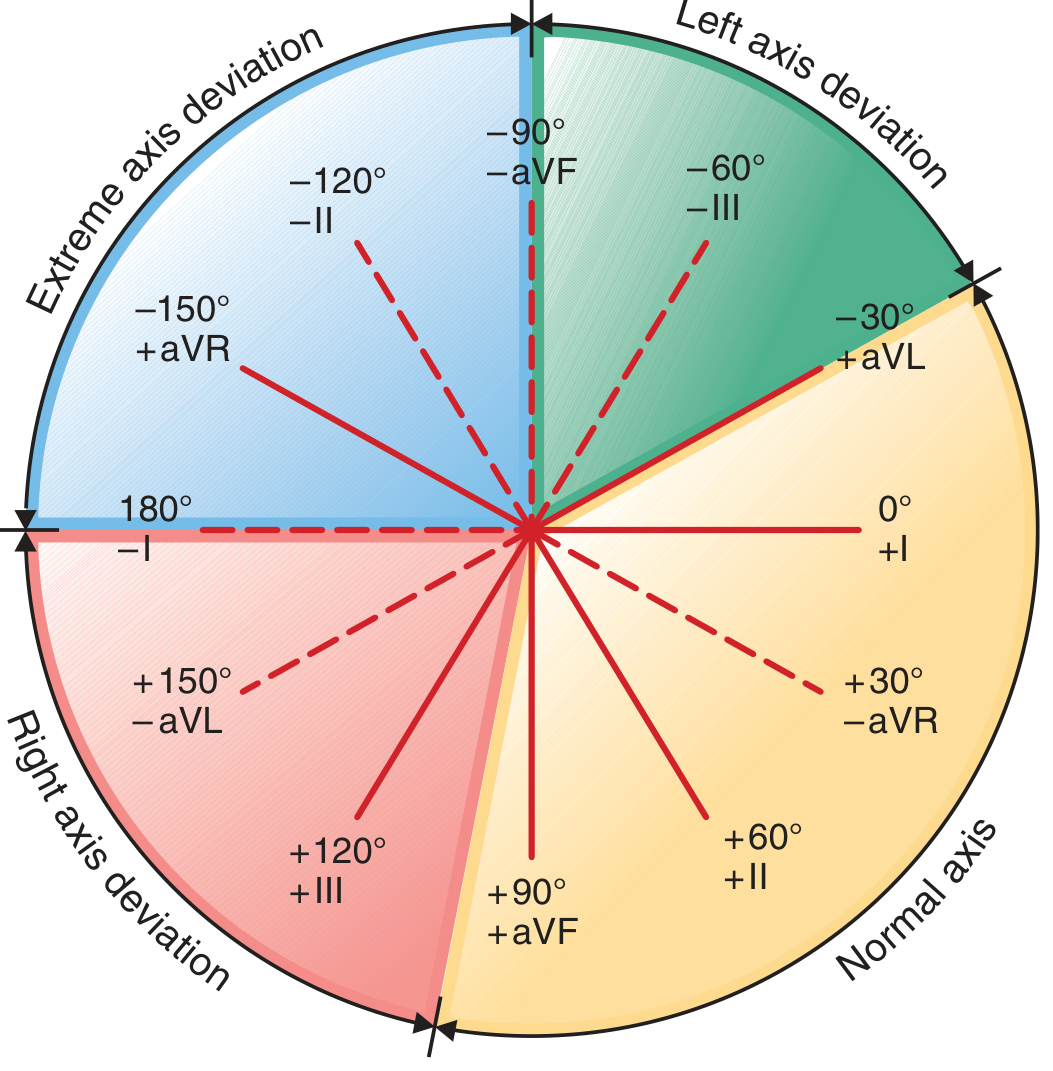
The mean QRS axis describes the overall direction of ventricular depolarization in the frontal plane:
| Axis | Range | Common Causes |
|---|---|---|
| Normal | -30° to +90°/+100° | Normal variant |
| Left axis deviation (LAD) | More negative than -30° | Left ventricular hypertrophy, left anterior fascicular block |
| Right axis deviation (RAD) | More positive than +90°/+100° | Right ventricular hypertrophy, left posterior fascicular block, lateral MI |
| Extreme | -90° to ±180° | Severe disease |
Quick trick: If lead I is positive and aVF is positive → normal axis. If I is positive and aVF is negative → LAD.
Systematic 14-Step ECG Interpretation
Harrison's recommends analyzing every ECG in this order:
- Standardization/calibration - check paper speed and gain (1 mV = 10 mm is standard), artifacts, correct lead placement
- Rhythm - regular or irregular? Sinus vs. ectopic?
- Heart rate - regular rhythm: divide 300 by the number of large squares between R waves; irregular: count QRS complexes in 10 seconds × 6
- PR interval - normal 120-200 ms; prolonged = AV block; shortened = pre-excitation
- QRS interval - normal <120 ms; wide = bundle branch block or ventricular origin
- QT/QTc interval - prolonged QT is a risk factor for torsades de pointes
- Mean QRS axis - use hexaxial diagram above
- P waves - morphology, axis, one P per QRS?
- QRS voltages - high = hypertrophy; low = pericardial effusion, obesity, COPD
- Precordial R-wave progression - loss = anterior MI or LBBB
- Abnormal Q waves - pathologic Q waves (>40 ms wide or >25% of QRS height) = old infarction
- ST segments - elevation = STEMI or pericarditis; depression = ischemia, NSTEMI
- T waves - inversion = ischemia, ventricular hypertrophy, BBB; peaked = hyperkalemia
- U waves - prominent U waves = hypokalemia, bradycardia, certain drugs
Always compare with previous ECGs - this is invaluable.
Calculating Heart Rate (Quick Methods)
Regular rhythm:
- Memorize: 300, 150, 100, 75, 60, 50 for 1, 2, 3, 4, 5, 6 large squares between R waves
- Formula: 300 ÷ (number of large squares between consecutive R peaks)
Irregular rhythm (e.g., atrial fibrillation):
- Count all QRS complexes in a 10-second rhythm strip and multiply by 6
Key Pathological Patterns (Quick Reference)
| ECG Finding | Think of |
|---|---|
| ST elevation in contiguous leads | STEMI (in the territory of the affected vessel) |
| ST depression + T inversion | NSTEMI / unstable angina |
| Wide QRS with RBBB pattern (rSR' in V1) | Right bundle branch block |
| Wide QRS with LBBB pattern (broad R in V5/V6) | Left bundle branch block |
| Absent P waves, irregularly irregular QRS | Atrial fibrillation |
| Sawtooth baseline, regular QRS | Atrial flutter (~300 bpm atrial rate) |
| Short PR + delta wave | Wolff-Parkinson-White (WPW) pre-excitation |
| Prolonged QT | Drug toxicity, electrolyte disturbance, congenital LQTS |
| Peaked T waves | Hyperkalemia |
| Pathologic Q waves | Old myocardial infarction |
ECG Limitations
Computerized ECG analysis has major limitations - it should never be accepted without careful clinician review. ECG interpretation requires correlation with the patient's age, sex, and clinical status. Many errors are errors of omission, which is why a systematic approach is essential.
- Harrison's Principles of Internal Medicine, 22E (2025), Chapter 247 - ECG Leads, Genesis of the Normal ECG, Clinical Interpretation of the ECG
Want me to go deeper on any specific part - arrhythmias, bundle branch blocks, axis, STEMI patterns, or anything else?
This is a shared conversation. Sign in to Orris to start your own chat.