Please explain this presentation in detail and deapth Prepare me for usmle questions Don't skip any topic I have test tmr Please explain everything in detail Add extra information that you fell like i should know as a medical student studying for usmle
Reading File
Reading File
Running Command
cd /tmp/workspace/attachments/506366d5-9425-4c4a-864b-19da2c3951ec/ && python3 -c " from pptx import Presentation prs = Presentation('3-Receptors.pptx') for i, slide in enumerate(prs.slides, 1): print(f'\n=== SLIDE {i} ===') for shape in slide.shapes: if shape.has_text_frame: text = shape.text_frame.text.strip() if text: print(text) "
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed. Let me compile the full, comprehensive USMLE-focused study guide.
🧬 Receptors - Complete USMLE Study Guide
This is a full breakdown of every topic in the presentation, with extra USMLE-tested details added. Study this carefully before your exam tomorrow.
PART 1: RECEPTOR BASICS - Foundations
What Is a Receptor?
A receptor is a specific protein that binds a signaling molecule (ligand) to initiate a cellular response. Receptors are either:
- Bound to the plasma membrane (for hydrophilic/polar ligands that cannot cross the membrane)
- Located intracellularly - in the cytoplasm or nucleus (for hydrophobic/lipid-soluble ligands that can diffuse across the membrane)
Ligand-Receptor Binding
- Binding follows equilibrium kinetics - as ligand concentration increases, more receptors bind; as it decreases, the ligand dissociates
- Unlike enzyme-substrate binding, ligand binding does not chemically modify the ligand
- Receptors have very high affinity for their specific ligands
- ~5% of human genome codes for plasma membrane receptors
USMLE HIGH-YIELD: Upregulation vs. Downregulation
| Concept | Cause | Result |
|---|---|---|
| Upregulation | Chronic exposure to an antagonist | More receptors inserted into membrane → increased sensitivity to agonists |
| Downregulation | Chronic exposure to an agonist | Receptors internalized/removed → decreased response (tolerance) |
Clinical examples (USMLE loves these):
- Morphine tolerance = downregulation of opioid receptors (need higher doses over time)
- Beta-blocker withdrawal = beta-blockers (antagonists) cause upregulation of beta receptors → if stopped suddenly, excess catecholamines can trigger rebound tachycardia/hypertension
- Bronchodilator tachyphylaxis = overuse of albuterol (beta-2 agonist) downregulates receptors → less response
Tachyphylaxis = rapid desensitization often caused by phosphorylation of the receptor, rendering it unresponsive. Also called desensitization.
Refractoriness = period after stimulation when ion channel receptors cannot be re-activated (especially important for Na+ channels in cardiac physiology).
Spare Receptors (Reserve Receptors)
- Because signal amplification is so powerful, only a fraction of all receptors need to be occupied to get a maximum response
- Insulin: ~99% of insulin receptors are "spare" - huge functional reserve
- Beta-1 adrenergic (heart): only ~5-10% spare - almost all must be occupied for max contractility; this is why heart failure patients have little reserve
- Lippincott Illustrated Reviews: Pharmacology, p. 92
Co-receptors
Some receptors require a co-receptor: the ligand binds a surface binding receptor first, which then binds to a signal receptor that initiates the cellular reaction. Classic USMLE example: HIV uses CD4 as primary receptor + CCR5 or CXCR4 as co-receptors to enter T cells.
PART 2: TWO BROAD CATEGORIES OF RECEPTORS
1. Intracellular Receptors
Key features:
- Located in the cytoplasm or nucleus
- Ligands must be lipid-soluble/hydrophobic to diffuse through the plasma membrane
- Examples of ligands: steroid hormones, thyroid hormone, vitamin D, retinoic acid
- Mechanism: hormone diffuses in → binds receptor → hormone-receptor complex acts as a transcription factor → binds specific DNA sequences → activates or represses gene transcription → new protein synthesis (effects take hours to days)
Mnemonic for steroid/intracellular receptor ligands - "STAVE":
- Sex steroids (estrogen, progesterone, testosterone)
- Thyroid hormone
- Aldosterone & Adrenal corticosteroids (cortisol)
- Vitamin D
- Ecdysone (insect, not tested)
- Also: Retinoic acid (vitamin A derivative)
USMLE Pearl: Thyroid hormone receptor sits in the nucleus already bound to DNA (in an inactive state) even without ligand. When T3 binds, it relieves repression. This is different from steroid receptors, which reside in the cytoplasm and translocate to nucleus after ligand binding (though details vary by hormone - this is sometimes simplified in Step 1 material).
Transcription Factors:
- Proteins that bind specific DNA sequences and regulate the rate of mRNA synthesis
- The hormone-receptor complex in this system acts as a gene-specific (site-specific) transcription factor
- Effects are delayed (hours-days) because new proteins must be synthesized
2. Plasma Membrane Receptors
- Required for polar, hydrophilic, large molecules that cannot cross the membrane
- Examples: peptide hormones (insulin, glucagon, GH), catecholamines (epinephrine, NE), cytokines
- Have three domains: extracellular ligand-binding domain, transmembrane domain (alpha-helices), intracellular signal transduction domain
- Basic Medical Biochemistry, p. 337
PART 3: FOUR MAJOR CLASSES OF PLASMA MEMBRANE RECEPTORS
The presentation organizes these into 3-4 classes. The USMLE tests all of them.
CLASS 1: Ion Channel Receptors (Ligand-Gated Ion Channels / Ionotropic Receptors)
Structure:
- Transmembrane domain containing the ion pore
- Extracellular ligand-binding domain
- When ligand binds → conformational change → channel opens → ions flow
Signal transduction = the conformational change itself (fastest of all receptor types - milliseconds)
Key USMLE examples:
| Receptor | Ion | Agonist (Neurotransmitter) | Effect |
|---|---|---|---|
| Nicotinic ACh receptor (nAChR) | Na+/K+ (depolarizing) | Acetylcholine, Nicotine | Muscle contraction, autonomic ganglia depolarization |
| GABA-A receptor | Cl- (hyperpolarizing) | GABA | Inhibitory - neuronal hyperpolarization |
| NMDA receptor | Ca2+, Na+, K+ | Glutamate + Glycine (co-agonist) | Excitatory; requires glycine AND voltage (Mg2+ block removed by depolarization) |
| AMPA receptor | Na+/K+ | Glutamate | Excitatory |
| Glycine receptor | Cl- | Glycine | Inhibitory (in spinal cord) |
| 5-HT3 receptor | Na+/K+ | Serotonin | Excitatory |
USMLE drug pearls:
- Benzodiazepines & Barbiturates act on GABA-A receptor (but at different sites!)
- Benzodiazepines: increase frequency of Cl- channel opening
- Barbiturates: increase duration of Cl- channel opening
- Succinylcholine: depolarizing NMB - acts at nAChR, causes persistent depolarization
- Ketamine: NMDA antagonist (dissociative anesthetic)
- Stahl's Essential Psychopharmacology notes two major classes of ion channels: ligand-gated and voltage-gated
CLASS 2: Catalytic Receptors - Receptors That ARE Kinases or BIND Kinases
These are the enzyme-linked receptors. The presentation covers 3 subtypes:
2A. Receptor Tyrosine Kinases (RTKs)
Structure: Single transmembrane alpha-helix, extracellular ligand domain, intracellular tyrosine kinase domain
Mechanism (step by step - USMLE loves this):
- Ligand binds → receptor undergoes dimerization (two receptor monomers come together)
- Autophosphorylation occurs: each monomer phosphorylates the other on tyrosine residues
- Phosphotyrosines serve as docking sites for adaptor proteins like Grb2 (via its SH2 domain)
- Grb2 recruits SOS (son of sevenless) through its SH3 domain
- SOS is a GEF (guanine nucleotide exchange factor) - it activates Ras by exchanging GDP → GTP on Ras
- Ras-GTP (active) binds and activates Raf (= MAPKKK)
- Raf starts a phosphorylation cascade: Raf → MEK (MAPKK) → ERK (MAPK)
- ERK translocates to nucleus → alters transcription factors → gene expression for cell survival and proliferation
USMLE RTK Examples:
| Ligand/Hormone | Receptor |
|---|---|
| Insulin | Insulin receptor (RTK) |
| IGF-1 | IGF-1 receptor |
| EGF | EGFR/HER1 |
| PDGF | PDGF receptor |
| FGF | FGF receptor |
| VEGF | VEGF receptor |
| HER2/neu | Overexpressed in breast cancer (target of trastuzumab) |
Oncology USMLE pearl - Ras mutations:
- Ras is a proto-oncogene
- Point mutations in RAS (especially codons 12, 13, 61) prevent GTPase activity → Ras stays "stuck ON" in GTP-bound form → constitutive activation of MAP kinase pathway → uncontrolled cell proliferation
- RAS mutations found in: KRAS in pancreatic cancer (~90%), colon cancer, lung adenocarcinoma
- NF1 mutations: NF1 encodes neurofibromin, a GAP (GTPase-activating protein) that normally turns Ras OFF. Loss of NF1 → Ras stays active → neurofibromatosis type 1
The SH2/SH3 domain concept:
- SH2 domain = binds phosphotyrosine residues
- SH3 domain = binds proline-rich sequences
- This explains signal specificity: different phosphotyrosines (with different surrounding amino acid sequences) recruit different downstream proteins
2B. JAK-STAT Receptors
Structure: Single transmembrane receptor with no intrinsic kinase activity. Instead, the intracellular domain is non-covalently associated with JAK (Janus Kinase).
Mechanism:
- Cytokine/hormone binds → receptor dimerization
- Adjacent JAKs phosphorylate each other (trans-phosphorylation)
- JAKs phosphorylate receptor tyrosines → creates docking sites
- STAT proteins (Signal Transducers and Activators of Transcription) bind to phosphorylated receptor via their SH2 domains
- JAK phosphorylates STATs on tyrosine residues
- Phospho-STATs dimerize, translocate to nucleus, activate gene transcription
USMLE JAK-STAT Ligands:
| Cytokine/Hormone | JAK | STAT |
|---|---|---|
| Growth Hormone (GH) | JAK2 | STAT5 |
| Prolactin | JAK2 | STAT5 |
| Erythropoietin (EPO) | JAK2 | STAT5 |
| Thrombopoietin | JAK2 | STAT5 |
| IFN-alpha/beta | JAK1, TYK2 | STAT1, STAT2 |
| IFN-gamma | JAK1, JAK2 | STAT1 |
| IL-6 | JAK1, JAK2 | STAT3 |
| IL-2, IL-4, IL-7 | JAK1, JAK3 | STAT5 |
USMLE drug pearl - JAK inhibitors:
- Tofacitinib, baricitinib, upadacitinib = JAK inhibitors used in rheumatoid arthritis, IBD, JAK2 polycythemia vera
- Ruxolitinib = JAK1/2 inhibitor used in polycythemia vera and myelofibrosis (both driven by JAK2 V617F mutation)
JAK2 V617F mutation = point mutation in JAK2 → constitutively active → seen in ~95% of polycythemia vera cases, also myelofibrosis and essential thrombocythemia
SOCS proteins (Suppressors of Cytokine Signaling) act as negative feedback to terminate JAK-STAT signaling.
2C. Serine-Threonine Kinase Receptors (TGF-beta Receptor Family)
Structure: Receptor dimer of Type I and Type II subunits, both with serine/threonine kinase domains
Mechanism:
- TGF-beta (transforming growth factor beta) binds Type II receptor
- Type II receptor recruits and phosphorylates Type I receptor
- Activated Type I receptor phosphorylates R-Smad (receptor-regulated Smad, e.g., Smad2, Smad3)
- Phospho-R-Smad binds Co-Smad (Smad4)
- Smad dimer translocates to nucleus → regulates gene expression
- Can either activate or inhibit transcription depending on the target gene and cell context
USMLE TGF-beta pearls:
- TGF-beta acts as a tumor suppressor in early cancer (inhibits cell proliferation) but can be pro-tumorigenic in late cancer (promotes invasion, EMT, immune evasion)
- TGF-beta also promotes fibrosis (important in idiopathic pulmonary fibrosis, liver cirrhosis)
- BMP (Bone Morphogenetic Proteins) also use Serine-Threonine kinase receptors (Smad1/5/8 pathway)
- Activin uses the same pathway (Smad2/3)
2D. Receptor Guanylyl Cyclase (Mentioned in slide 13)
Mechanism: Ligand binds extracellular domain → intracellular guanylyl cyclase domain activated → catalyzes GTP → cGMP → activates PKG (protein kinase G)
USMLE Examples:
- ANP/BNP (atrial/brain natriuretic peptide) receptors are guanylyl cyclases → increase cGMP → vasodilation, natriuresis
- NO (nitric oxide) acts on soluble guanylyl cyclase (not a receptor per se, but same downstream pathway) → cGMP → vasodilation → basis of nitrates (nitroglycerin) in angina
- Sildenafil (Viagra) inhibits PDE-5 (which normally breaks down cGMP) → prolongs cGMP → vasodilation in pulmonary hypertension and erectile dysfunction
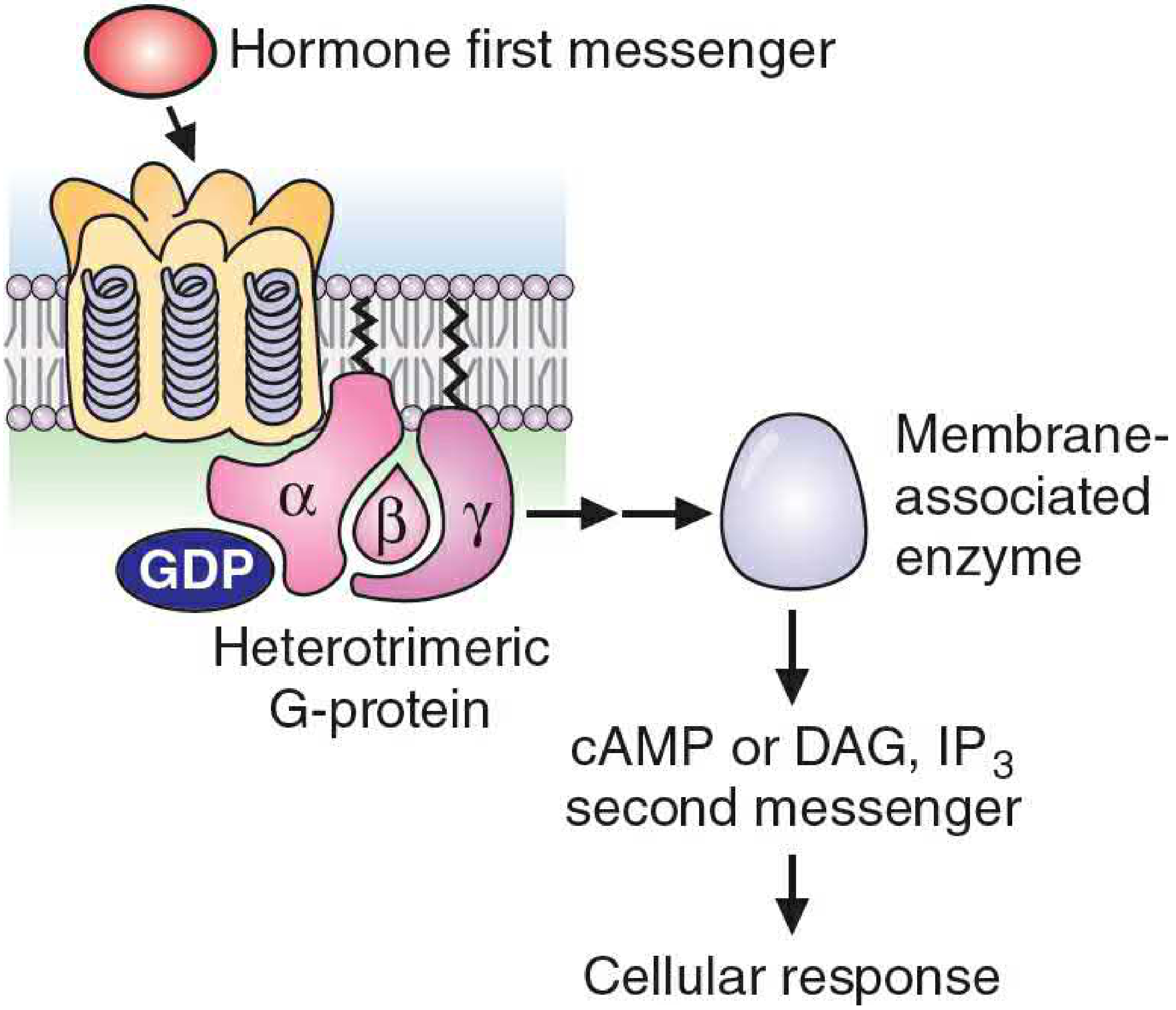
CLASS 3: Heptahelical Receptors (G-Protein-Coupled Receptors / GPCRs)
The most clinically important class - ~40% of all drugs target GPCRs!
Structure:
- 7 transmembrane alpha-helices (hence "hepta-helical")
- Extracellular N-terminus and ligand-binding loops
- Intracellular loops couple to heterotrimeric G-proteins
- Most abundant plasma membrane receptor type (~2% of human genome)
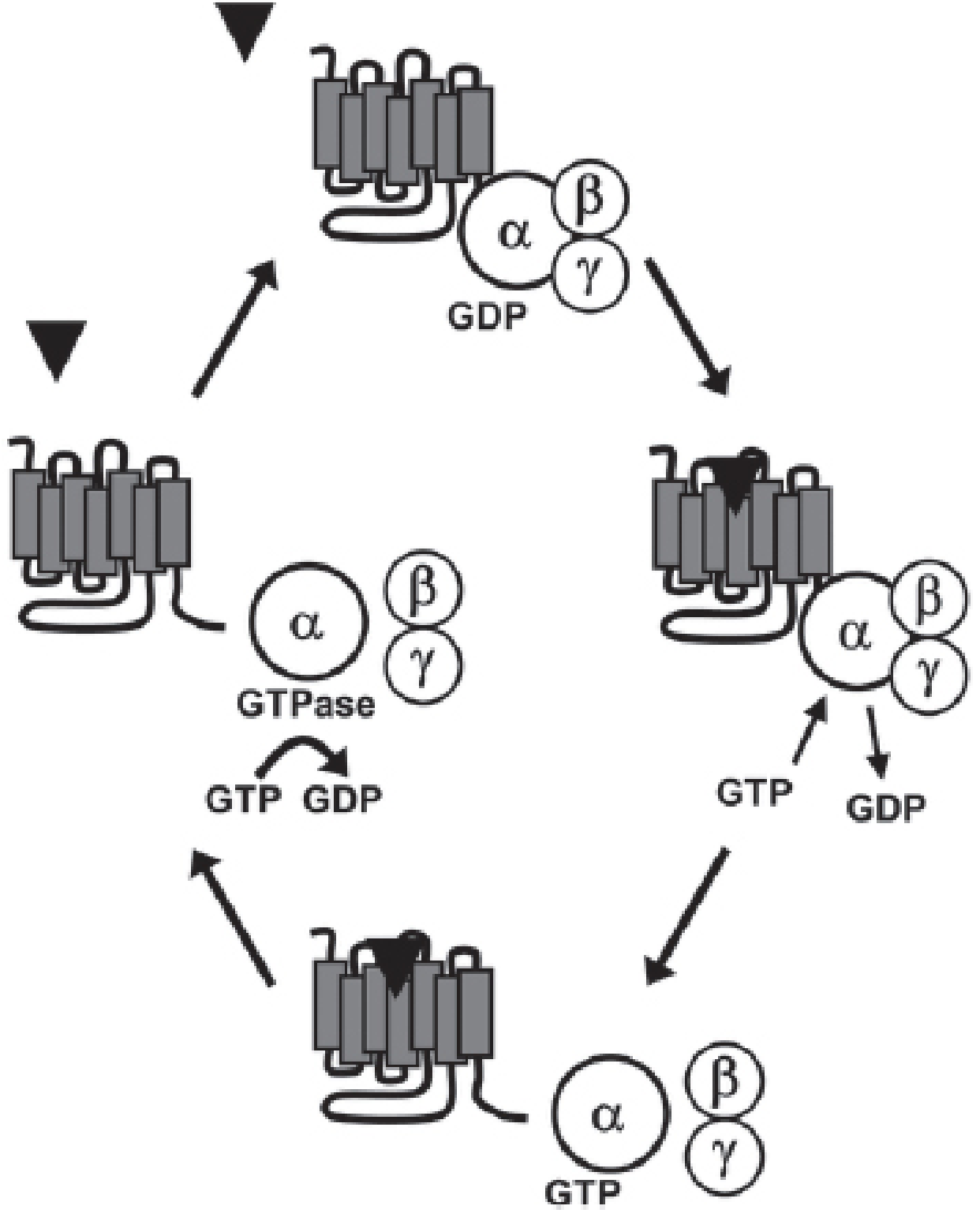
The G-Protein Cycle (MEMORIZE THIS):
- Basal state: Inactive heterotrimer = alpha (α) + beta (β) + gamma (γ) subunits, alpha bound to GDP
- Agonist binds GPCR → receptor changes conformation → promotes GDP dissociation from alpha subunit
- GTP binds to alpha subunit (more abundant than GDP in cytoplasm) → conformational change
- Alpha-GTP dissociates from beta-gamma → both alpha and beta-gamma become active effectors
- Active subunits activate/inhibit downstream effectors (adenylyl cyclase, phospholipase C, ion channels)
- Alpha subunit has intrinsic GTPase activity → hydrolyzes GTP → GDP → alpha re-associates with beta-gamma and with receptor → back to inactive state
The signal terminates when GTP is hydrolyzed to GDP. This is the "off switch."
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 562
- Basic Medical Biochemistry, p. 338
The Four Major G-Protein Classes - MASTER TABLE:
| G-protein | Effect on Effector | Second Messenger | Final Effect |
|---|---|---|---|
| Gs (stimulatory) | Activates adenylyl cyclase | ↑ cAMP → PKA activation | Phosphorylates proteins (diverse effects) |
| Gi (inhibitory) | Inhibits adenylyl cyclase | ↓ cAMP | Opposes Gs effects |
| Gq | Activates phospholipase C-beta (PLC-β) | ↑ IP3 + DAG | IP3→Ca2+ release; DAG→PKC activation |
| G12/13 | Activates Rho GTPase | (no classic second messenger) | Cytoskeletal changes, cell motility |
Second Messenger Details:
cAMP pathway (via Gs):
- Gs → adenylyl cyclase → cAMP → activates PKA (Protein Kinase A)
- PKA phosphorylates serine/threonine residues on target proteins
- Examples: glycogen breakdown, lipolysis, cardiac contractility (beta-1), bronchodilation (beta-2)
- Terminated by phosphodiesterase (PDE) which converts cAMP → 5'-AMP
- Methylxanthines (theophylline, caffeine) inhibit PDE → increase cAMP → bronchodilation
IP3/DAG pathway (via Gq):
- Gq → PLC-β → cleaves PIP2 (phosphatidylinositol 4,5-bisphosphate) into:
- IP3 (inositol trisphosphate): goes to ER → opens Ca2+ channels → ↑ intracellular Ca2+
- DAG (diacylglycerol): stays in membrane → activates PKC (Protein Kinase C)
- Ca2+ + calmodulin → activates calmodulin-dependent kinases (CaMK)
- Muscle contraction (smooth muscle alpha-1 receptors use this), platelet activation, glandular secretion
USMLE Receptor-to-G-protein Table - HIGH YIELD:
| Receptor | G-protein | Second Messenger | Clinical Relevance |
|---|---|---|---|
| Beta-1 adrenergic | Gs | ↑ cAMP | Heart: ↑ HR, ↑ contractility; beta-1 blockers in heart failure/HTN/angina |
| Beta-2 adrenergic | Gs | ↑ cAMP | Bronchodilation (albuterol), uterine relaxation, vasodilation |
| D1 dopamine | Gs | ↑ cAMP | Renal vasodilation (fenoldopam); reward pathway |
| H2 histamine | Gs | ↑ cAMP | Gastric acid secretion; H2 blockers (ranitidine, famotidine) |
| V2 vasopressin (ADH) | Gs | ↑ cAMP | Water reabsorption in collecting duct (inserts aquaporin-2); nephrogenic DI when V2 receptor mutated |
| PTH | Gs | ↑ cAMP | ↑ Ca2+ reabsorption (kidney), ↑ bone resorption |
| TSH | Gs | ↑ cAMP | Thyroid hormone synthesis |
| FSH, LH | Gs | ↑ cAMP | Gonadal hormone synthesis |
| Glucagon | Gs | ↑ cAMP | Glycogenolysis, gluconeogenesis |
| Alpha-1 adrenergic | Gq | ↑ IP3/DAG | Vasoconstriction, pupil dilation, bladder sphincter contraction; alpha-1 blockers for BPH/HTN |
| M1, M3 muscarinic | Gq | ↑ IP3/DAG | M3: Glandular secretion, smooth muscle contraction, pupil constriction, bladder contraction; M1: gastric acid |
| H1 histamine | Gq | ↑ IP3/DAG | Bronchoconstriction, itch/allergic response; H1 blockers (diphenhydramine, loratadine) |
| Alpha-2 adrenergic | Gi | ↓ cAMP | Pre-synaptic inhibition of NE release; CNS: clonidine lowers BP |
| M2 muscarinic | Gi | ↓ cAMP | ↓ HR (SA node), AV node slowing |
| D2 dopamine | Gi | ↓ cAMP | Dopamine pathway; target of antipsychotics |
| Mu opioid receptor | Gi | ↓ cAMP | Analgesia, sedation, respiratory depression, constipation |
| Adenosine A1 | Gi | ↓ cAMP | Slows AV conduction; adenosine for SVT |
| Somatostatin receptor | Gi | ↓ cAMP | Inhibits GH, TSH, insulin secretion; octreotide for carcinoid/acromegaly |
USMLE mnemonic - "Gs GQ Gi":
- "QS" = Qq stimulates, Gi inhibits adenylyl cyclase ... no wait.
- Better: "QQQQQ" = Gq uses "IP3 please" (I=IP3, P=phospholipase C, 3=PKC/Ca2+)
- Gs = "Stimulates" cAMP, Gi = "Inhibits" cAMP
Bacterial Toxins that Exploit G-Protein Signaling:
| Toxin | Mechanism | Effect |
|---|---|---|
| Cholera toxin | ADP-ribosylates Gs alpha → cannot hydrolyze GTP → Gs permanently active → ↑↑↑ cAMP in intestinal cells | Massive Cl-/water secretion → "rice-water diarrhea" |
| Pertussis toxin | ADP-ribosylates Gi alpha → cannot exchange GDP for GTP → Gi permanently inactive → ↑ cAMP | Loss of feedback inhibition; pertussis toxin also blocks chemokine receptor signaling → lymphocyte homing failure → lymphocytosis |
PART 4: THE RAS-MAP KINASE PATHWAY (Presented in Depth on Slides 27-28)
This was given significant attention in the presentation. Here it is structured for USMLE:
Full cascade:
Growth factor (EGF, PDGF, FGF, etc.)
↓
RTK dimerization + autophosphorylation on Tyr residues
↓
GRB2 (adaptor protein) binds phosphoTyr via SH2 domain
↓
SOS (GEF) recruited via GRB2's SH3 domain
↓
SOS activates RAS: GDP → GTP exchange on Ras
↓
Ras-GTP binds RAF (MAPKKK = MAP kinase kinase kinase)
↓
RAF phosphorylates MEK (MAPKK)
↓
MEK phosphorylates ERK (MAPK)
↓
ERK enters nucleus → phosphorylates transcription factors
↓
Gene expression → cell survival, proliferation, differentiation
KEY USMLE points:
- RAS is a proto-oncogene - when mutated to an oncogene, it loses GTPase activity and is permanently ON
- The α-subunit GTPase activity (and for Ras, intrinsic GTPase activity) is the OFF switch - any mutation inactivating GTPase = constitutive activation = cancer
- BRAF V600E mutation (common in melanoma) similarly keeps the kinase cascade permanently active → target of vemurafenib (BRAF inhibitor)
- GAPs (GTPase-Activating Proteins) speed up GTP hydrolysis (help turn signaling OFF)
- GEFs (Guanine nucleotide Exchange Factors) promote GDP-for-GTP exchange (help turn signaling ON)
- NF1 gene encodes neurofibromin = a GAP for Ras; loss of NF1 = neurofibromatosis type 1 = café-au-lait spots, Lisch nodules, neurofibromas
PART 5: TGF-BETA / SMAD PATHWAY (Slide 35)
The presentation shows this figure explicitly. TGF-β signals through:
- TGF-β dimer binds Type II serine/threonine kinase receptor
- Type II receptor recruits and phosphorylates Type I receptor (serine kinase domain)
- Type I receptor phosphorylates R-Smads (Smad2, Smad3)
- R-Smad + Co-Smad (Smad4) dimerize
- Complex translocates to nucleus
- Activates or represses target gene transcription
USMLE pearls:
- TGF-β = tumor suppressor early in cancer; promotes metastasis late
- Smad4 (DPC4) is deleted in ~50% of pancreatic cancers
- TGF-β promotes epithelial-to-mesenchymal transition (EMT) in cancer
- TGF-β promotes fibrosis - lung, liver, kidney
PART 6: SUMMARY COMPARISON TABLE (PERFECT FOR USMLE REVIEW)
| Receptor Type | Location | Signal Speed | Mechanism | Key Examples |
|---|---|---|---|---|
| Intracellular (Nuclear) | Cytoplasm/Nucleus | Hours-Days (gene expression) | Hormone-receptor = transcription factor | Steroids, thyroid hormone, Vit D, retinoic acid |
| Ion Channel (Ionotropic) | Plasma membrane | Milliseconds | Conformational change → ion flow | nAChR, GABA-A, NMDA, AMPA, glycine, 5-HT3 |
| RTK | Plasma membrane | Minutes (protein modification) | Dimerization → autophosphorylation → Ras-MAP kinase | Insulin, EGF, PDGF, IGF-1, FGF, VEGF |
| JAK-STAT | Plasma membrane | Minutes-Hours | Cytokine → JAK phosphorylates STAT → gene expression | GH, prolactin, EPO, cytokines (IL-2, IFN-gamma) |
| Ser/Thr Kinase | Plasma membrane | Minutes-Hours | Type II phosphorylates Type I → Smad pathway | TGF-beta, BMP, activin |
| Guanylyl Cyclase | Plasma membrane | Minutes | Ligand binding → cGMP synthesis → PKG | ANP, BNP |
| GPCR (Heptahelical) | Plasma membrane | Seconds-Minutes (via 2nd messengers) | GDP-GTP exchange on Gα → effectors (AC/PLC) → cAMP or IP3/DAG | Adrenergic, muscarinic, dopamine, opioid, serotonin (non-5HT3) |
PART 7: BONUS HIGH-YIELD USMLE CONCEPTS NOT TO MISS
Phosphoinositide Signaling Details
- PI3K (phosphoinositide 3-kinase): activated by RTKs and GPCRs → phosphorylates PIP2 → PIP3 → recruits Akt (PKB) → promotes cell survival (anti-apoptosis), protein synthesis (via mTOR), glycogen synthesis
- PTEN = phosphatase that dephosphorylates PIP3 → acts as a tumor suppressor; PTEN mutations in endometrial cancer, prostate cancer, glioblastoma
- Akt → mTOR pathway: growth, proliferation, survival; targets: everolimus, sirolimus (mTOR inhibitors) used in renal cell carcinoma, transplant rejection
cAMP and Protein Kinase A - Complete Story
- cAMP binds regulatory subunits of PKA → releases catalytic subunits (active)
- PKA phosphorylates CREB (cAMP Response Element Binding protein) in nucleus → activates CRE-containing genes
- PKA also phosphorylates: phosphorylase kinase (activates glycogen breakdown), hormone-sensitive lipase (activates lipolysis), L-type Ca2+ channels in heart
- Cholera toxin → constitutive Gs activation → massive cAMP → PKA → phosphorylation of CFTR → massive Cl- secretion into intestinal lumen
Nitric Oxide (NO) - Special Case
- Not a conventional receptor but extremely USMLE-tested
- L-arginine + NOS (nitric oxide synthase) → NO
- NO diffuses into smooth muscle cells → activates soluble guanylyl cyclase → ↑ cGMP → PKG → myosin light chain phosphatase activation → smooth muscle relaxation/vasodilation
- eNOS (endothelial): vasodilation, inhibits platelet aggregation
- nNOS (neuronal): neurotransmission/synaptic plasticity
- iNOS (inducible): macrophage killing of bacteria/tumor cells (septic shock mechanism)
- Nitroglycerin → acts as NO donor → venodilation (primarily) → ↓ preload → treats angina
Receptor Phosphorylation and Desensitization
The GRK (G-protein Receptor Kinase) family phosphorylates GPCRs after agonist binding → beta-arrestin binds → uncouples receptor from G-protein → receptor internalized → desensitization. This is the molecular basis of tachyphylaxis/tolerance.
Autocrine vs. Paracrine vs. Endocrine Signaling
- Endocrine: hormone travels long distance through blood
- Paracrine: acts on nearby cells
- Autocrine: acts on the same cell that secreted it (common in growth factors, important in cancer)
- Juxtacrine: requires direct cell-cell contact (Notch-Delta signaling)
USMLE-STYLE PRACTICE QUESTIONS
Q1. A patient is prescribed a long-acting beta-2 agonist for asthma. After 3 months, they report that the medication is less effective. What is the most likely cellular mechanism?
A: Downregulation (internalization) of beta-2 adrenergic receptors due to chronic agonist exposure → decreased receptor density → reduced bronchodilator response.
Q2. A mutation in the RAS gene results in a single amino acid substitution that impairs GTPase activity. What is the likely consequence?
A: Ras remains permanently bound to GTP (active state) → constitutive activation of MAP kinase pathway → uncontrolled cell proliferation → cancer (oncogenic gain-of-function mutation).
Q3. Cholera toxin causes profuse watery diarrhea. Which of the following best describes its mechanism?
A: ADP-ribosylation of Gs-alpha subunit → prevents GTP hydrolysis → Gs permanently active → constitutive adenylyl cyclase activation → ↑↑↑ cAMP → PKA-mediated phosphorylation of CFTR → massive Cl- and water secretion.
Q4. A child is found to have café-au-lait spots, axillary freckling, and multiple neurofibromas. Genetic testing reveals a loss-of-function mutation in the NF1 gene. The protein product of NF1 normally functions as which of the following?
A: A GTPase-activating protein (GAP) for Ras. Neurofibromin accelerates GTP hydrolysis, inactivating Ras. Loss of neurofibromin → Ras stays active → increased cell proliferation.
Q5. A 35-year-old woman has elevated prolactin and GH levels. A drug is needed that blocks the receptors for these hormones. Which type of receptor would be targeted?
A: JAK-STAT receptor (specifically, GH and prolactin act through JAK2-STAT5 signaling). Pegvisomant (GH receptor antagonist) blocks GH's JAK-STAT action.
Q6. Albuterol stimulates beta-2 receptors. Trace the complete intracellular pathway to bronchodilation.
A: Albuterol binds beta-2 (GPCR) → activates Gs → GTP-Gs-alpha activates adenylyl cyclase → ↑cAMP → activates PKA → PKA phosphorylates myosin light chain kinase (MLCK, inhibiting it) AND opens K+ channels → smooth muscle relaxation → bronchodilation.
Q7. A researcher finds that a hormone binds a membrane receptor and activates phospholipase C. What are the two downstream second messengers and their immediate effects?
A: PLC cleaves PIP2 into: (1) IP3 → binds ER receptor → releases Ca2+ from ER → activates calmodulin-dependent kinases; (2) DAG → remains in plasma membrane → activates PKC (protein kinase C) → phosphorylates various proteins.
QUICK-REFERENCE MNEMONICS
Gs ligands (↑cAMP): "BADFs and TSH-PTH-V2" = Beta-1, Beta-2, Adenosine A2, D1, FSH/LH, TSH, PTH, V2-ADH, Glucagon, H2
Gq ligands (↑IP3/DAG): "QQQ = Alpha-1, M1/M3, H1, V1-vasopressin, Oxytocin, GnRH, TRH"
Gi ligands (↓cAMP): "I inhibit = Alpha-2, M2, D2, Mu/Delta/Kappa opioid, Adenosine A1, Somatostatin"
RTKs remember with "PEFF-GI" = PDGF, EGF, FGF, FGF, Insulin, IGF (all RTKs)
JAK-STAT = "GhostProlEPO" = GH, Prolactin, EPO, Thrombopoietin, cytokines (most ILs, IFNs)
Good luck tomorrow! The most tested areas are: GPCR classification and second messengers, RAS pathway and oncogenes, JAK2 mutations, downregulation/upregulation, bacterial toxin mechanisms (cholera, pertussis), and intracellular steroid receptor targets.
This is a shared conversation. Sign in to Orris to start your own chat.