Massive blood transfusion
Reading File
Finding Sources
Searching PubMed
"massive transfusion" AND "damage control resuscitation"
Finding Sources
Reading File
Searching PubMed
"massive transfusion" AND hemorrhage
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
I now have comprehensive content. Let me compile the full answer.
Massive Blood Transfusion (MBT)
Definition
Massive transfusion (MT) is most commonly defined as transfusion of ≥10 units of packed red blood cells (PRBCs) within 24 hours. Alternate definitions include:
- Replacement of 50% of total blood volume within 3 hours, or
- Blood loss exceeding 150 mL/minute
Up to 10% of military and 3-5% of civilian trauma patients require massive transfusion. - Tintinalli's Emergency Medicine
Triggers and Prediction Scores
The Assessment of Blood Consumption (ABC) Score uses four values available on arrival:
| Variable | Present = 1 point |
|---|---|
| Penetrating mechanism of injury | Yes |
| Positive FAST examination | Yes |
| SBP <90 mmHg | Yes |
| Heart rate >120 bpm | Yes |
Score ≥2: Sensitivity 76-90%, Specificity 67-87% for predicting MT. - Tintinalli's Emergency Medicine, p. 108
The Lethal Triad
Massive hemorrhage initiates a deadly cycle of:
- Hypothermia - from environmental heat loss, anesthesia, exposed peritoneal surfaces, cold resuscitation fluids
- Acidosis - from tissue hypoxia and large-volume crystalloid (hyperchloremic acidosis)
- Coagulopathy - hypothermia + acidosis reduce coagulation factor activity and platelet function; crystalloid dilutes clotting factors
Together known as the "lethal triad," these three factors markedly increase mortality. Modern resuscitation - called Damage Control Resuscitation (DCR) - is specifically designed to prevent and reverse this triad. - Mulholland and Greenfield's Surgery, p. 1558
Acute Traumatic Coagulopathy (ATC)
Up to 25% of trauma patients arrive already coagulopathic - before resuscitation begins. Proposed mechanisms include:
- Diffuse endothelial damage
- Activation of the protein C pathway
- Massive catecholamine release
ATC is then worsened by hypothermia, acidosis, and dilution. - Mulholland and Greenfield's Surgery, p. 1557
Detecting coagulopathy: Conventional PT/aPTT/INR are unreliable - they are performed at physiologic pH and temperature, failing to capture the effects of hypothermia and acidosis. Viscoelastic hemostatic assays (TEG - thromboelastography; ROTEM - rotational thromboelastometry) give a dynamic, real-time picture of the entire coagulation-fibrinolysis process and are preferred for guiding MTP.
Damage Control Resuscitation (DCR) - Principles
| Component | Details |
|---|---|
| Permissive hypotension | Target SBP ~90 mmHg (MAP ~60 mmHg) before definitive hemostasis; avoids "popping the clot" |
| Minimize crystalloids | Large-volume crystalloid raises BP but worsens coagulopathy and dilutes clotting factors |
| High-ratio blood products | PRBCs : FFP : Platelets in a 1:1:1 (or 1:2 ratio) |
| Hypertonic saline | Pulls water back into the vascular compartment |
| Early coagulopathy correction | Factor VIIa, prothrombin complex concentrate (PCC), tranexamic acid (TXA) |
Caution: Permissive hypotension is for otherwise-healthy young patients with penetrating trauma. It is NOT recommended in traumatic brain injury (TBI), blunt trauma, or elderly patients with cardiac/carotid disease. - Mulholland and Greenfield's Surgery, p. 1559
Massive Transfusion Protocol (MTP)
The MTP is a predefined blood bank activation system. All verified trauma centers are required by the American College of Surgeons to have an MTP in place. - Sabiston Textbook of Surgery, p. 588
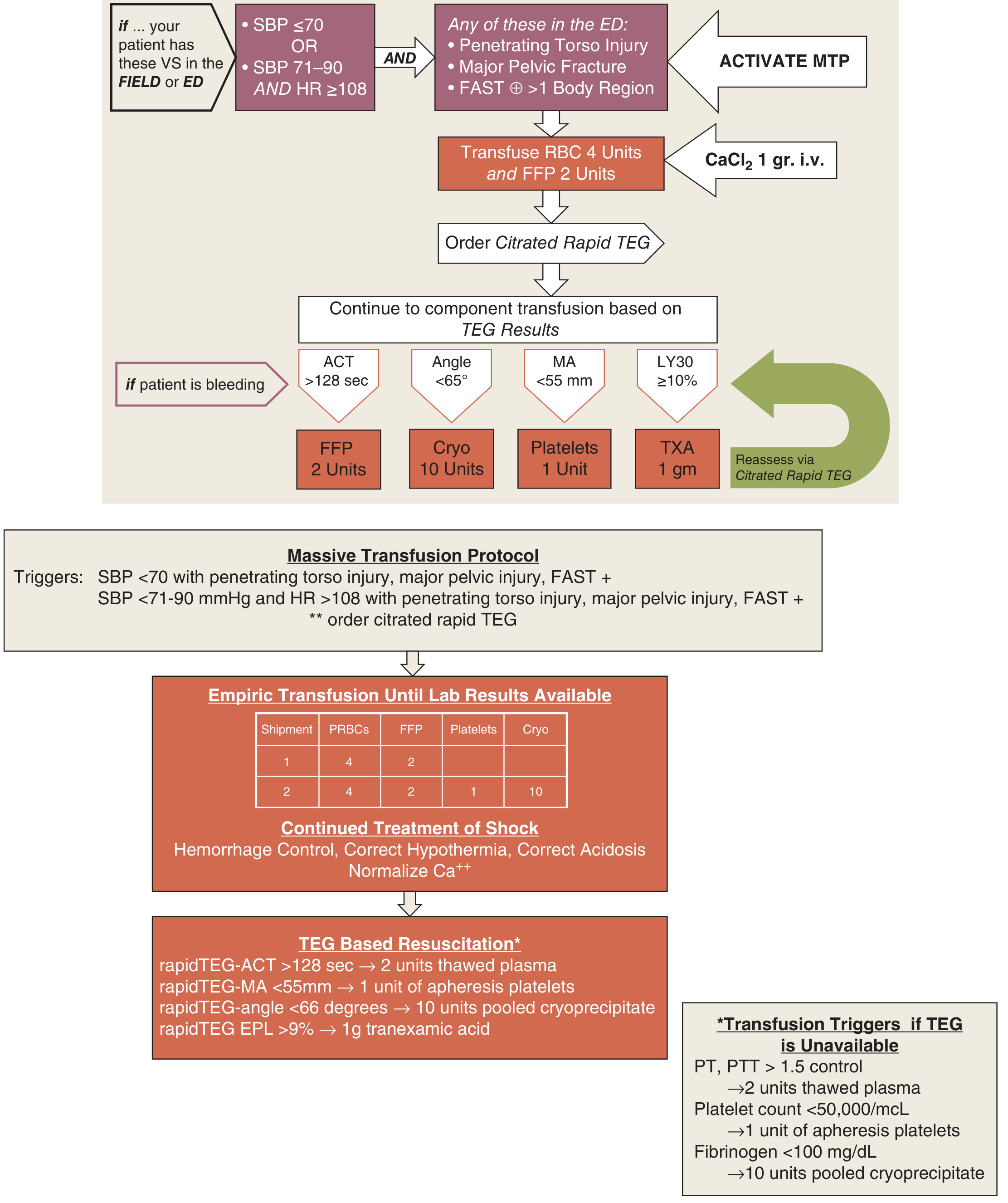
Empiric Initial Approach (before lab results):
- Shipment 1: 4 units PRBCs + 2 units FFP
- Shipment 2: 4 units PRBCs + 2 units FFP + 1 unit platelets + 10 units cryoprecipitate
- Alternatively: low-titer O whole blood (LTOWB) if available
Optimal Transfusion Ratio:
- 1:1:1 ratio (Plasma : Platelets : RBCs) - reduces early exsanguination and improves hemostasis
- 1:1:2 ratio - remains the most commonly recommended; no significant difference in 30-day mortality compared to 1:1:1
- High plasma-to-PRBC ratios offer survival benefit independent of coagulopathy - possibly by endothelial repair and reducing vascular permeability - Tintinalli's Emergency Medicine, p. 108; Goldman-Cecil Medicine, p. 1850
TEG-Guided Transfusion (when available):
| TEG Finding | Interpretation | Action |
|---|---|---|
| ACT >128 sec | Clotting factor deficiency | 2 units FFP |
| Angle <65° | Low fibrinogen | 10 units cryoprecipitate |
| MA <55 mm | Poor platelet function | 1 unit apheresis platelets |
| LY30 ≥10% (EPL >9%) | Fibrinolysis | TXA 1 g |
If TEG unavailable:
- PT/PTT >1.5x control → 2 units thawed plasma
- Platelets <50,000/μL → 1 unit apheresis platelets
- Fibrinogen <100 mg/dL → 10 units pooled cryoprecipitate
Adjuncts
Tranexamic Acid (TXA)
- Antifibrinolytic - blocks the fibrinolytic phase of trauma-induced coagulopathy
- Should be given as early as possible after injury
- Military (MATTERS study) and civilian studies show reduced overall mortality
- Recommended for all trauma patients suspected of significant bleeding - Bailey & Love, p. 8093
Calcium
- PRBCs and FFP both contain citrate, which chelates calcium → life-threatening hypocalcemia
- Calcium chloride is preferred over calcium gluconate (the latter requires hepatic metabolism)
- Maintain ionized calcium ≥0.9 mmol/L
- Signs of hypocalcemia: circumoral paresthesias, muscle weakness, cardiac dysfunction - Tintinalli's EM, p. 109; Harrison's, p. 1261
Whole Blood
- Fresh whole blood has demonstrated superior outcomes in combat settings
- Low-titer O whole blood (LTOWB) is increasingly used in civilian trauma centers as first-line therapy when available - Sabiston, p. 588; supported by a 2024 EAST meta-analysis (PMID 38531812)
Complications of Massive Transfusion
| Complication | Mechanism | Management |
|---|---|---|
| Hypothermia | Cold products, heat loss | Warm all fluids; Bair Hugger; warm ventilator gases; keep ambient temp high |
| Hypocalcemia | Citrate chelation | IV CaCl₂; monitor ionized Ca |
| Hyperkalemia | Potassium leaks from stored RBCs | ECG monitoring; K⁺ management |
| Dilutional coagulopathy | Loss + dilution of clotting factors | High-ratio blood products; cryoprecipitate |
| Metabolic acidosis | Tissue hypoxia + citrate load | Restore perfusion; avoid excess crystalloid |
| Transfusion-Related Acute Lung Injury (TRALI) | Donor antibodies activating neutrophils | Supportive care |
| Transfusion-Associated Circulatory Overload (TACO) | Volume overload | Diuretics; reduce rate |
| Hypothermia-induced coagulopathy | Enzyme dysfunction <34°C | Aggressive rewarming |
Special Considerations
- Blood type: O-negative PRBCs are reserved for females of childbearing age when blood type is unknown; O-positive can be used in males and post-menopausal women
- Crossmatching: Draw blood samples early, before the patient has received ~1 blood volume of product - donor blood interferes with subsequent crossmatching - Tintinalli's EM, p. 108
- Obstetric hemorrhage: MTP protocols are applicable in postpartum hemorrhage; TXA also reduces maternal mortality - Creasy & Resnik's Maternal-Fetal Medicine
- VTE prophylaxis: Once hemorrhage is controlled, initiate LMWH; consider removable IVC filters for prolonged contraindications - Schwartz's Principles of Surgery, p. 236
Recent Evidence (2024-2025)
- A 2024 systematic review (PMID 38616968) addressed defining "ultra-massive transfusion" (beyond the standard 10-unit threshold), noting inconsistent definitions in the literature.
- A 2024 EAST Practice Management Guideline (PMID 38531812) conditionally recommends whole blood resuscitation over component therapy for injured patients requiring transfusion, based on survival benefit data.
- A 2025 Cochrane Review (PMID 39911088) examined transfusion strategies specifically for postpartum hemorrhage management.
Sources: Tintinalli's Emergency Medicine; Sabiston Textbook of Surgery; Schwartz's Principles of Surgery; Mulholland and Greenfield's Surgery; Goldman-Cecil Medicine; Bailey & Love's Short Practice of Surgery; Miller's Anesthesia; Barash Clinical Anesthesia; Henry's Clinical Diagnosis
This is a shared conversation. Sign in to Orris to start your own chat.