Examination for ulcer patient
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full structured answer.
Examination of an Ulcer Patient
Based on S. Das - A Manual on Clinical Surgery, 13th Edition
Definition
An ulcer is a break in the continuity of the covering epithelium (skin or mucous membrane), either following molecular death of the surface epithelium or its traumatic removal.
I. HISTORY
1. Mode of Onset
- Did it follow trauma or arise spontaneously?
- Traumatic ulcers heal if the agent is removed; chronicity implies a persisting cause (e.g., dental ulcer of the tongue, ulcer over a joint)
- Spontaneous ulcers may follow a swelling (matted tuberculous lymph nodes, gummata, or a rapidly growing malignant tumour)
- Ulcers may arise in a leg with varicose veins or vascular insufficiency
- A malignant ulcer (Marjolin's) may develop on the scar of a burn
2. Duration
- Acute ulcer: present for a short duration
- Chronic ulcer: persists for a long period
- Note the incubation period: Hunterian chancre (syphilis) = 3-4 weeks; chancroid (soft sore) = 3-4 days
3. Pain
- Painful: acutely inflamed ulcers
- Painless: syphilitic ulcers, trophic/neurogenic ulcers (tabes dorsalis, transverse myelitis, peripheral neuritis)
- Slightly painful: tuberculous ulcers
- Initially painless (later painful if deep invasion): malignant ulcers (epithelioma, basal cell carcinoma)
- Venous ulcer: relatively painless
- Arterial ulcer: pain is the main complaint, worsened by elevation
4. Discharge
- Nature: serum, pus, or blood?
- Serosanguineous discharge suggests tuberculosis or carcinoma
- Scant discharge with pale granulation: tuberculous ulcer
5. Associated Disease
- Nervous diseases (tabes dorsalis, syringomyelia, transverse myelitis, peripheral neuritis) → trophic/perforating ulcer
- Generalised tuberculosis, nephritis, or diabetes → ulcer formation
- Syphilis: primary stage (chancre), tertiary stage (gummatous ulcer)
II. PHYSICAL EXAMINATION
General Survey
- Do not focus only on the ulcer - give due attention to the general examination
- Ulcer may be a sequel of malnutrition, generalised atherosclerosis, syphilis, or tuberculosis
III. LOCAL EXAMINATION
A. INSPECTION
| Feature | What to Observe |
|---|---|
| 1. Size and Shape | Tuberculous ulcers: oval; coalescence gives irregular crescentic border. Gummatous ulcer: circular/oval. Rodent ulcer (BCC): oval. Squamous cell carcinoma: irregular |
| 2. Number | Single or multiple |
| 3. Site | Specific sites indicate type - medial lower third of leg (venous), anterior/outer leg/dorsum foot (arterial), heel/ball of foot (trophic), tibia/sternum (gummatous) |
| 4. Edge | See table below |
| 5. Floor (base) | Granulation tissue (healthy healing); slough (infected/trophic); exposed bone/tendon (arterial/deep) |
| 6. Discharge | Amount, colour, nature |
| 7. State of surrounding skin | Eczema/pigmentation around venous ulcer; erythema in acute inflammation |
Types of Ulcer Edge (Key Feature for Diagnosis)
| Edge Type | Significance |
|---|---|
| Sloping/shelving edge | Healing ulcer |
| Undermined edge | Tuberculous ulcer (thin, reddish-blue, undermined) |
| Punched-out edge | Arterial (ischaemic) ulcer, trophic ulcer, syphilitic (gummatous) ulcer |
| Everted/rolled edge | Squamous cell carcinoma (malignant ulcer) |
| Raised/pearly/rolled edge | Rodent ulcer (basal cell carcinoma) |
| Indurated/hard edge | Carcinomatous infiltration |
B. PALPATION
- Tenderness - Acutely inflamed ulcers are tender; malignant ulcers usually not tender
- Edge - Feel the edge: indurated edge = malignant; soft/undermined = TB; punched-out = arterial/trophic
- Floor/Base - Probe for depth; presence of slough, granulation tissue, bone, or tendon exposure
- Induration at base - Slight induration in TB; marked/hard induration in malignancy
- Discharge - Milk the ulcer gently; note nature and amount
- Relations with deeper structures - Move the ulcer over deeper structures; fixity to underlying bone/fascia = gummatous or malignant; mobility = benign
- Surrounding skin - Increased temperature + tenderness = acute inflammation; fixity of surrounding skin to deeper structures = malignant; test for loss of sensation (nerve involvement); feel for thickened peripheral nerves (leprosy, neurofibromatosis)
C. EXAMINATION OF LYMPH NODES (Often Forgotten!)
| Condition | Lymph Node Character |
|---|---|
| Acutely inflamed ulcer | Enlarged, tender, acute lymphadenitis; may suppurate |
| Tuberculous ulcer | Enlarged, matted, slightly tender |
| Hunterian chancre (syphilis) | Discrete, firm, shotty - pathognomonic |
| Gummatous ulcer | Lymph nodes not usually involved |
| Rodent ulcer (BCC) | Not affected (early obliteration of lymphatics) |
| Malignant ulcer | Stony hard, may be fixed - indicates metastasis |
Note: Simple lymph node enlargement in malignancy does NOT always mean metastasis - may be due to secondary infection. Stony hard consistency confirms metastatic involvement.
D. EXAMINATION FOR VASCULAR INSUFFICIENCY
- Search for varicose veins in the upper leg/thigh when ulcer is on the lower leg
- If no varicose veins, examine peripheral arteries proximal to the ulcer (atherosclerosis, Buerger's disease, Raynaud's disease)
- Check: dorsalis pedis pulse (often feeble/absent in arterial ulcer)
- Look for ischaemic changes: pallor, dry skin, loss of hair, nail fissuring
- Elevation test: In arterial ulcer, elevation above heart level - no healing + pain worsened
E. EXAMINATION FOR NERVE LESION
- Trophic ulcers result from repeated trauma to insensitive areas
- Test sensation around the ulcer (light touch, pin-prick, temperature)
- Check for motor deficits
- Palpate peripheral nerves for thickening (leprosy, neurofibromatosis)
IV. DIFFERENTIAL FEATURES SUMMARY: Common Ulcer Types
| Feature | Venous | Arterial | Trophic | Tuberculous | Malignant (SCC) | Rodent (BCC) |
|---|---|---|---|---|---|---|
| Site | Medial lower leg (above malleolus) | Anterior leg, toes, heel (below malleolus) | Heel, ball of foot, pressure areas | Lymph node areas | Any | Face (nose, eyelids) |
| Pain | Painless | Very painful | Painless | Slight | Painless initially | Painless |
| Edge | Sloping | Punched-out | Punched-out/callous | Undermined | Everted/indurated | Rolled/pearly |
| Base | Granulation tissue | Minimal granulation; exposed tendons/bone | Slough, callous | Pale granulation, pale/unhealthy | Friable/necrotic | Superficial |
| Discharge | Moderate seropurulent | Scant | Scant/purulent | Scanty serosanguineous | Seropurulent/bloody | Minimal |
| Lymph nodes | Normal | Normal | Normal | Matted, tender | Stony hard | Unaffected |
| Surrounding skin | Eczema, pigmentation, lipodermatosclerosis | Ischaemic changes | Callosity, loss of sensation | Relatively normal | Indurated, fixed | Pearly border |
- S. Das, A Manual on Clinical Surgery, 13th Edition
Trendenberg test
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Excellent - comprehensive content and images obtained. Here is the full structured answer:
Trendelenburg Test
The Trendelenburg test has two entirely different clinical applications - one in vascular surgery (varicose veins) and one in orthopaedics (hip abductor weakness).
1. TRENDELENBURG TEST - Varicose Veins (Brodie-Trendelenburg Test)
Purpose
To identify the main site of venous incompetence in the leg - specifically whether varicose veins are caused by:
- Superficial venous incompetence (saphenofemoral junction failure), or
- Deep venous insufficiency with incompetent perforating veins
Procedure
Step 1 - Drain the veins:
- Patient lies supine
- Elevate the leg above body level to drain the varicose veins completely
Step 2 - Apply tourniquet/compression:
- Apply a tourniquet (or digital compression) to the proximal thigh over the suspected incompetent feeding vein (saphenofemoral junction)
Step 3 - Ask the patient to stand:
- Patient stands erect with tourniquet in place
- Observe whether the veins remain empty or fill rapidly
Step 4 - Release the tourniquet:
- Release the compression and observe again
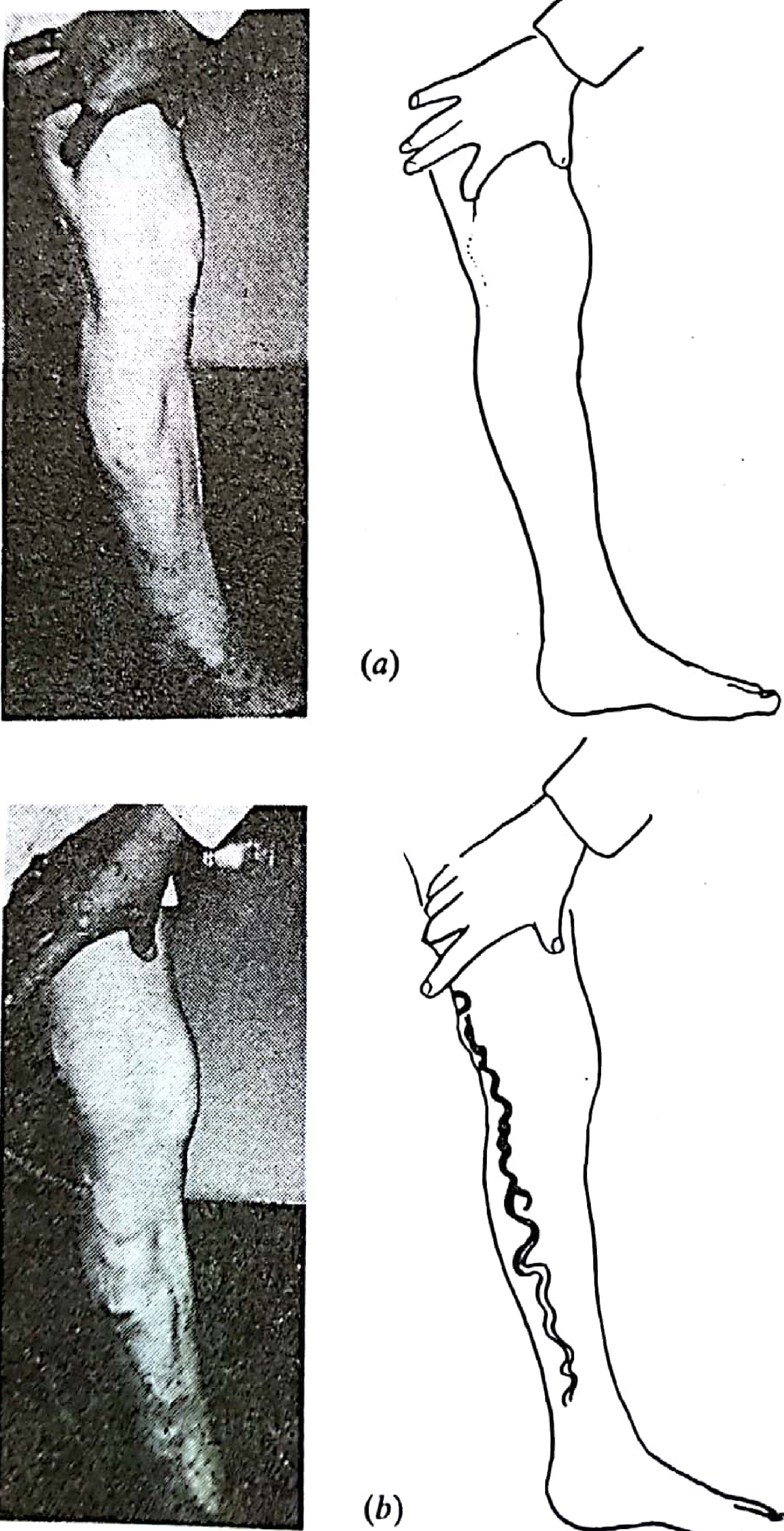
Fig. 25.14 - Trendelenburg's test. (a) No early refilling with compression held. (b) Release of compression allows incompetent downward filling. (Pye's Surgical Handicraft, 22nd Ed.)
Interpretation
| Finding | Interpretation |
|---|---|
| Veins remain empty while tourniquet is in place → fill rapidly on tourniquet release | Positive test - Saphenofemoral incompetence; the reflux is from above (superficial system). Primary varicose veins |
| Veins fill rapidly even before tourniquet is released (within 30 s of standing) | Negative filling control test - Varicose veins are caused by deep venous insufficiency and incompetent perforating veins |
| Veins remain empty even after tourniquet release | Indicates incompetence is below the tourniquet level - reposition and repeat at a lower level |
Key rule: If the varices remain empty under tourniquet compression but fill promptly on release, the tourniquet site marks the level of incompetence. The compression site is marked before surgical ligation. - Pye's Surgical Handicraft, 22nd Ed.
Perthes Test (Companion test)
To assess deep venous obstruction:
- Tourniquet placed on midthigh after patient stands (veins filled)
- Patient walks for 5 minutes
- Patent deep system + competent perforators → superficial veins below tourniquet collapse
- Deep venous obstruction → superficial veins distend further with walking
- Harrison's Internal Medicine, 22nd Ed.
2. TRENDELENBURG SIGN - Hip Abductor Weakness (Orthopaedic)
Purpose
To test the strength and integrity of the hip abductor muscles (gluteus medius and gluteus minimus), and diagnose weakness or paralysis of these muscles.
Procedure
- Examiner stands behind the patient
- Ask the patient to stand on one leg (the suspected affected side)
- Observe the level of the pelvis/iliac crests
Interpretation
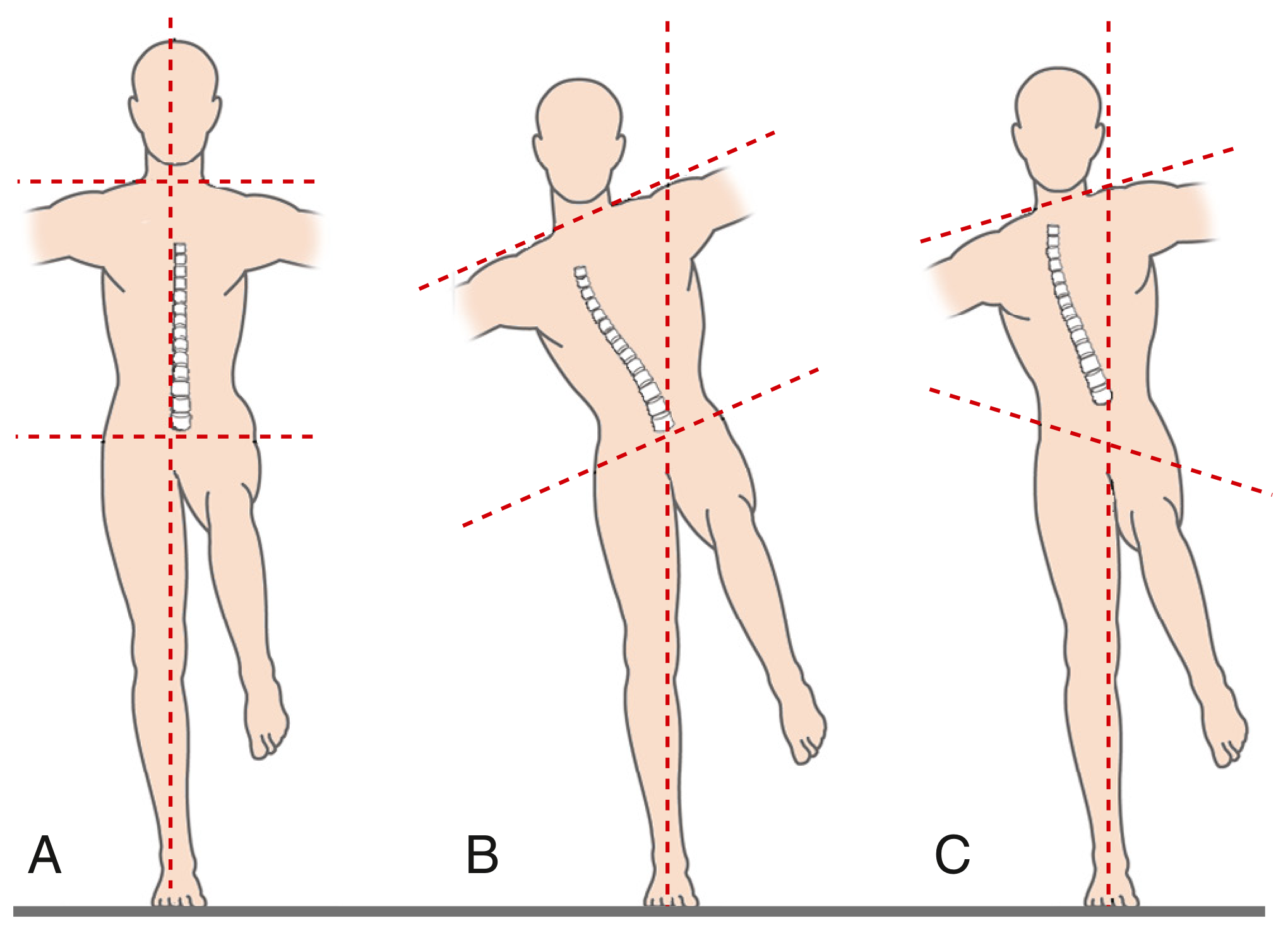
A: Normal single-legged stance - pelvis level. B: Positive Trendelenburg lurch (trunk leans to affected side) with negative sign. C: Positive lurch with pelvic obliquity. (Firestein & Kelley's Textbook of Rheumatology)
| Finding | Interpretation |
|---|---|
| Pelvis remains level | Normal - abductors are strong |
| Pelvis drops on the UNSUPPORTED (opposite/swing) side | Positive Trendelenburg sign - abductor weakness on the standing (affected) side |
| Trunk lurch toward the affected side | Trendelenburg gait/lurch - compensatory mechanism to shift centre of gravity over the weak side |
Mechanism
- Normally, when standing on one leg, the ipsilateral gluteus medius and minimus contract to hold the pelvis level
- If these muscles are weak, the pelvis drops toward the unsupported side
- The patient compensates by leaning the trunk over the affected hip (Trendelenburg lurch)
- If bilateral: produces a waddling gait (duck gait)
Causes of Positive Trendelenburg Sign
| Category | Examples |
|---|---|
| Nerve injury | Superior gluteal nerve injury (most common), radiculopathy |
| Fractures/trauma | Neck of femur fracture, pelvic fractures |
| Congenital | Congenital dislocation of hip (CDH), coxa vara, dysplasia |
| Neuromuscular | Poliomyelitis, myelomeningocele, spinal cord lesions |
| Post-surgical | Disruption of gluteus medius/minimus insertion after hip surgery |
| Other | Slipped capital femoral epiphysis (SCFE), abductor tendon tears |
Positive signs are typically found with damage to the superior gluteal nerve. Bilateral positive signs (as in CDH) produce waddling gait. - Gray's Anatomy for Students
Quick Comparison Summary
| Feature | Varicose Vein Test | Hip Test |
|---|---|---|
| Also called | Brodie-Trendelenburg test | Trendelenburg sign |
| Position | Supine → standing | Standing on one leg |
| Tests | Saphenofemoral valve competence | Hip abductor (gluteus medius) strength |
| Positive result | Varices fill on tourniquet release | Pelvis drops to unsupported side |
| Specialty | Vascular surgery | Orthopaedics / Neurology |
Sources: Pye's Surgical Handicraft 22nd Ed. | Harrison's Internal Medicine 22nd Ed. | Firestein & Kelley's Rheumatology | Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.