Discuss the uses of indocyanine green dye in present day surgery.
Reading File
Searching the Web
indocyanine green ICG fluorescence guided surgery uses 2024 2025
Searching PubMed
indocyanine green fluorescence guided surgery
Finding Sources
Reading Web Page
indocyanine green ICG surgery uses recommendations
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
I now have a thorough foundation from the textbooks and current literature. Let me compose the comprehensive answer.
Indocyanine Green (ICG) in Present-Day Surgery
Background and Pharmacology
Indocyanine green is a water-soluble tricarbocyanine dye that was first used in the late 1950s to evaluate liver function, and subsequently found use in cardiology and ophthalmology. It is the only FDA-approved near-infrared (NIR) fluorophore for intraoperative use. Once injected intravenously, it binds strongly to plasma proteins (predominantly albumin), is not metabolized, and is completely eliminated unchanged in bile. Its half-life is short - 3 to 5 minutes - which permits repeated intraoperative evaluations during a single procedure.
ICG absorbs NIR light at approximately 800 nm and emits fluorescence at ~830 nm. A dedicated camera system filters out wavelengths below 820 nm, capturing only the ICG-emitted signal, which is then superimposed on the white-light image. This gives surgeons real-time anatomical or physiological information that is invisible to the naked eye. Its severe reaction rate is extremely low (~0.05%), making it safe for routine intraoperative use.
- Fischer's Mastery of Surgery, 8th ed. (pp. 881-882)
Principle Operating Domains
1. Biliary Anatomy Visualization - Laparoscopic Cholecystectomy
One of the best-established uses of ICG is near-infrared fluorescence cholangiography (NIFC) during laparoscopic cholecystectomy. ICG (2.5 mL of a 25 mg/10 mL solution) is injected intravenously at least 45 minutes before the procedure, allowing time for hepatic excretion into bile. The cystic duct, common hepatic duct, and common bile duct (CBD) then fluoresce brilliantly under NIR light, revealing their anatomy and junctions before any dissection.
A landmark multicenter RCT by Dip et al. randomized 639 patients to white light alone vs. white + NIR light, showing superior extrahepatic bile duct visualization in the NIFC group. Critically, both cases of bile duct injury (BDI) in the trial occurred in the white-light-only group, as did four of five conversions to open surgery. A meta-analysis of eight prospective studies (1,603 NIFC vs. 5,070 non-NIFC cases) found the BDI rate roughly 75% lower with NIFC and the conversion rate ~95% lower. Two separate RCTs confirmed that ICG-based fluorescent cholangiography is as effective as intraoperative X-ray cholangiography for identifying bile duct variations.
- Fischer's Mastery of Surgery, 8th ed. (pp. 889-890); Sabiston Textbook of Surgery (p. 185)
2. Colorectal Surgery - Anastomotic Perfusion Assessment
Ischemia is a primary cause of anastomotic leaks in colorectal surgery. ICG fluorescence angiography provides a real-time map of bowel wall perfusion before and after the anastomosis is formed. The surgeon injects ICG IV (2.5 mL of 25 mg/10 mL), toggles to NIR mode, and within seconds the arterial supply of the bowel segment lights up, identifying areas of poor perfusion where the resection margin can be moved proximally.
The 2025 SAGES guidelines (the most current and comprehensive evidence synthesis available) gave a strong recommendation with moderate certainty for the use of FIGS with ICG in patients undergoing left-sided colorectal anastomosis, based on strong evidence that it reduces anastomotic leak rates. The European Registry EURO-FIGS, analyzing 1,240 patients across 30 hospitals in 8 countries, found that ICG imaging changed the intended resection level in 27% of cases, and 99% of surgeons reported higher confidence in their anastomosis when guided by ICG.
- Fischer's Mastery of Surgery, 8th ed. (p. 884); SAGES 2025 guidelines (PMID 41249539); PMID 41422225
3. Hepatic Surgery - Tumor Detection and Margin Assessment
The liver's intrinsic metabolism of ICG underpins several hepatic applications:
- Preoperative liver function testing: The ICG 15-minute retention rate (ICG-R15) is a standard tool to assess hepatic reserve and functional capacity before major hepatectomy, replacing the older constant-infusion clearance technique because of better tolerance.
- Intraoperative tumor identification: ICG (0.25-0.5 mg/kg) is administered 24 hours or more before surgery. Normal hepatocytes clear ICG into bile, while tumor cells - particularly metastases from colorectal and pancreatic cancer - are unable to accumulate ICG. This creates a sharp "dark spot" contrast against fluorescing liver parenchyma that guides resection margins.
- Differential tumor fluorescence: Hepatocellular carcinoma fluoresces less intensely than surrounding parenchyma, while fibrolamellar carcinoma and cholangiocarcinoma display brighter fluorescence than the hepatic background - enabling pathological differentiation.
- A 2024 systematic review and meta-analysis (PMID 38867212) confirmed that ICG-guided laparoscopic hepatectomy achieves significantly better surgical margin status in liver malignancies.
- Fischer's Mastery of Surgery, 8th ed. (pp. 886-887)
4. Sentinel Lymph Node (SLN) Mapping
ICG is now widely used for intraoperative SLN identification across multiple cancer types, exploiting the fact that ICG injected peritumorally drains through lymphatics to the regional sentinel nodes, which then fluoresce under NIR light (780 nm excitation).
- Breast cancer: ICG identifies sentinel nodes with 95-100% accuracy under infrared light at 780 nm - superior to older methods. It can be used alone or in combination with blue dye (>90% identification), and serves as an alternative when radioisotope (Tc-99m) is unavailable.
- Gastric cancer: ICG is injected submucosally around the primary lesion endoscopically. Within minutes, lymphatic drainage basins and SLNs light up under NIR, guiding lymphadenectomy. This is particularly valuable in laparoscopic/robotic settings where traditional blue dye or radiotracers are impractical.
- Colorectal cancer: A 2024 meta-analysis (PMID 39542857) found ICG fluorescence imaging significantly increases lymph node yield and improves long-term oncologic outcomes in colorectal cancer surgery.
- Gynecologic oncology: SLN mapping with ICG is now standard in endometrial and cervical cancer, with near-universal adoption in robotic-assisted surgery.
- Bailey and Love's Short Practice of Surgery, 28th ed. (pp. 957-958); Fischer's Mastery of Surgery, 8th ed. (p. 827)
5. Esophageal and Foregut Surgery
After esophagectomy, anastomotic leak rates can reach 30%, with ischemia as the dominant cause. ICG perfusion assessment of the gastric pull-up conduit is now routinely performed. After IV injection (2.5 mL of 25 mg/10 mL), the arterial supply of the conduit and esophageal stump can be visualized within 30 seconds under NIR. Studies have suggested that if NIR perfusion is visualized within 60 seconds of injecting ICG, the graft blood supply is likely adequate for anastomosis. "Fluorescence-based enhanced reality" software can quantify time-to-peak fluorescence, adding objective measurement to the assessment.
- Fischer's Mastery of Surgery, 8th ed. (pp. 890-891)
6. Bariatric Surgery
In sleeve gastrectomy, leaks near the esophagogastric (EG) junction are the most feared complication, driven by tenuous blood supply from the left phrenic and left gastric arteries. ICG perfusion assessment during sleeve gastrectomy and gastric bypass identifies areas of inadequate arterial supply before the staple line is completed, potentially allowing the surgeon to adapt the technique. Though current evidence from small series remains limited, the safety and simplicity of the approach make it an attractive adjunct.
- Fischer's Mastery of Surgery, 8th ed. (pp. 892-893)
7. Endocrine Surgery - Parathyroid Identification
Inadvertent devascularization or removal of parathyroid glands during thyroidectomy is a major cause of postoperative hypoparathyroidism. ICG angiography is now used to confirm the viability and perfusion of parathyroid glands in real time. After IV ICG injection, the parathyroid glands (which receive their blood supply from small end-arteries) display robust fluorescence when perfused, and diminished or absent fluorescence when devascularized. This guides the decision to auto-transplant a gland into the sternocleidomastoid muscle. Parathyroid autofluorescence (without exogenous dye) is also exploited but is limited to a few mm depth; ICG offers greater penetration and more dramatic signal.
- Sabiston Textbook of Surgery (pp. 1528-1529)
8. Thoracic Surgery
ICG is used in video-assisted (VATS) and robotic thoracoscopic surgery for:
- Pulmonary nodule localization: Before resection of small or ground-glass pulmonary nodules that are difficult to palpate, ICG is injected endobronchially or percutaneously to mark the target segment, which then fluoresces under NIR and guides the resection plane.
- Intersegmental plane identification: For anatomic segmentectomy, ICG administered intravenously lights up the perfused segment while the target segment to be resected remains dark (or vice versa), precisely delineating the intersegmental boundary.
- Fischer's Mastery of Surgery, 8th ed.; Bailey and Love's, 28th ed. (p. 3007)
9. Urology - Robotic Partial Nephrectomy
ICG is increasingly used in robotic-assisted partial nephrectomy (RAPN) for:
- Selective arterial clamping guidance: After IV ICG injection, the specific renal artery branch supplying the tumor can be identified before selective clamping, preserving perfusion to the remaining kidney. A 2024 meta-analysis (PMID 38000056) confirmed improved perioperative outcomes with ICG-guided selective arterial clamping compared to standard RAPN.
- Tumor margin delineation: Renal cortex and tumor tissue can be differentially fluoresced based on their perfusion characteristics.
- Adrenal surgery: ICG helps with intraperitoneal tumor localization during robotic adrenal procedures.
10. Plastic and Reconstructive Surgery - Flap Perfusion
ICG angiography is a standard tool for intraoperative assessment of:
- Free flap viability: Real-time assessment of arterial inflow and venous outflow in free tissue transfers, allowing early identification of a failing anastomosis before clinical signs develop.
- Perforator mapping: Locating perforator vessels preoperatively or intraoperatively for perforator flap design.
- Pericranial flap viability: Used in head and neck reconstructive surgery and skull base surgery to confirm vascular pedicle integrity.
- Cummings Otolaryngology Head and Neck Surgery (PMID references, p. 3159)
11. Ophthalmology - ICG Angiography
While technically a diagnostic rather than purely surgical use, ICG angiography (ICGA) is performed in the operating room or ophthalmic suite to:
- Evaluate choroidal circulation
- Diagnose polypoidal choroidal vasculopathy, central serous chorioretinopathy, and other macular diseases
- Guide photodynamic therapy targeting
- Kanski's Clinical Ophthalmology, 10th ed. (p. 568-575); The Wills Eye Manual
12. Acute Care and Emergency Surgery
A 2023 systematic review (PMID 37743419) assessed ICG in the acute care setting, highlighting its role in:
- Evaluating bowel ischemia and viability in emergency laparotomy
- Assessing perfusion of stomas and bowel segments
- Identifying the extent of ischemia in vascular emergencies
Technical Considerations
| Parameter | Detail |
|---|---|
| Excitation wavelength | ~800 nm (NIR) |
| Emission wavelength | ~830 nm |
| Half-life | 3-5 minutes |
| Elimination | Unchanged in bile (hepatic) |
| Severe reaction rate | ~0.05% |
| Typical IV dose | 2.5 mL of 25 mg/10 mL (for perfusion/cholangiography) |
| Hepatic tumor detection dose | 0.25-0.5 mg/kg, administered 24h pre-op |
| Re-dosing | Permitted - short half-life allows multiple intraoperative evaluations |
Modern laparoscopic towers and robotic platforms (including the da Vinci system with Firefly technology) are equipped with built-in NIR capabilities. Newer overlay systems allow white-light and NIR images to be superimposed in real time, maintaining anatomical context without toggling.
Current Evidence Level Summary (SAGES 2025)
| Application | Evidence/Recommendation Strength |
|---|---|
| Left-sided colorectal anastomosis | Strong recommendation, moderate certainty |
| Laparoscopic cholecystectomy (cholangiography) | Strong evidence, BDI reduction ~75% |
| Hepatic tumor identification | Good evidence from systematic reviews |
| SLN mapping (breast, gynecologic) | Well-established; >95% detection |
| Anastomotic leak prevention (esophageal, bariatric) | Promising; limited RCT evidence |
| Parathyroid identification | Growing evidence; no randomized trial yet |
Key References
- Fischer's Mastery of Surgery, 8th ed. - Chapter 27: Fluorescence-Guided Surgery
- Sabiston Textbook of Surgery - Chapter 11 (Tools section); Chapter on Thyroid Surgery
- Bailey and Love's Short Practice of Surgery, 28th ed. - Chapter 58 (Breast surgery)
- SAGES 2025 Guidelines - PMID 41249539 (strong recommendation for left-sided colorectal anastomosis)
- PMID 38867212 - Meta-analysis: ICG hepatectomy and surgical margin status
- PMID 39542857 - Meta-analysis: ICG lymph node detection in colorectal cancer
- PMID 38000056 - Meta-analysis: ICG-guided selective arterial clamping in partial nephrectomy
- PMID 41422225 - GRADE systematic review: ICG perfusion vs. standard to prevent anastomotic leak
Clinical feature and management of hyperkalemia
Reading File
Searching PubMed
hyperkalemia management treatment guidelines
Searching the Web
hyperkalemia clinical features management guidelines 2024 2025
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading Article
Loading Image
Loading Image
I have all the information needed. Now let me compile the comprehensive answer.
Hyperkalemia: Clinical Features and Management
Definition and Classification
Hyperkalemia is defined as a serum potassium (K⁺) concentration above 5.0-5.5 mEq/L. It is the most dangerous acute electrolyte abnormality, potentially causing life-threatening arrhythmias and death. The kidney normally maintains serum K⁺ between 3.5 and 5.0 mEq/L through tight regulation via the renin-angiotensin-aldosterone (RAA) axis.
| Grade | Serum K⁺ |
|---|---|
| Mild | 5.5 - 6.0 mEq/L |
| Moderate | 6.1 - 6.9 mEq/L |
| Severe | >7.0 mEq/L |
A level of 10.0 mEq/L is usually fatal, but decompensation and death can occur at any level above 7-8 mEq/L.
- Rosen's Emergency Medicine (p. 2513); Current Surgical Therapy, 14th ed. (p. 3136)
Pathophysiology
Serum K⁺ homeostasis depends on:
- Transcellular distribution: ~98% of total body K⁺ is intracellular, maintained by the Na⁺/K⁺-ATPase pump. Insulin and β₂-adrenergic stimulation drive K⁺ into cells; metabolic acidosis (by H⁺/K⁺ exchange) drives it out.
- Renal excretion: The primary route of K⁺ elimination, occurring in the distal nephron under aldosterone regulation.
Hyperkalemia raises the resting membrane potential of cardiac myocytes, causing increased membrane excitability, sluggish depolarization, and decreased duration of repolarization. At very high levels, K⁺ raises the depolarization threshold, producing overall depressed cardiac function.
Causes
Pseudohyperkalemia (Spurious)
The most common cause is hemolysis during or after the blood draw, leading to K⁺ release from red blood cells in vitro. Markedly elevated white cell or platelet counts can also cause in-vitro K⁺ leak. Always exclude this first with a repeat sample.
True Hyperkalemia
1. Impaired Renal Excretion (most important)
- Acute or chronic kidney disease
- Volume depletion / dehydration
- Adrenal insufficiency (Addison disease)
- Hyporeninemic hypoaldosteronism (Type 4 RTA - common in diabetic nephropathy)
2. Transcellular Shift (K⁺ moving from ICF → ECF)
- Metabolic acidosis (excluding organic acidoses)
- Insulin deficiency / diabetic ketoacidosis
- Hyperosmolality
- Non-selective β-blockers
- Depolarizing muscle relaxants (succinylcholine) - especially dangerous in burns, crush injury, rhabdomyolysis
- Digitalis toxicity
- Severe exercise, rhabdomyolysis, tumor lysis syndrome, massive hemolysis
3. Drugs (very common)
- ACE inhibitors and angiotensin receptor blockers (ARBs)
- Potassium-sparing diuretics (spironolactone, amiloride, triamterene)
- NSAIDs
- Cyclosporine
- Heparin, ketoconazole (decrease aldosterone production)
- Potassium supplementation / salt substitutes
4. Excessive Intake (rarely the sole cause unless renal excretion is impaired)
- High-K⁺ foods: salt substitutes, dried fruits, nuts, potatoes, tomatoes, spinach, bananas, citrus juices
Surgical note: In the surgical population, ischemia-reperfusion injury (especially after >4-6 hours of ischemia during revascularization) can cause acute severe systemic hyperkalemia. Succinylcholine is absolutely contraindicated in burns and crush injuries.
- Rosen's Emergency Medicine (p. 2513-2514); Washington Manual (pp. 2701-2711); Current Surgical Therapy, 14th ed. (p. 3138)
Clinical Features
Symptoms (often minimal until severe)
Hyperkalemia is notoriously difficult to diagnose on clinical grounds alone. Mild-to-moderate hyperkalemia is often found incidentally on blood tests.
| Severity | Symptoms |
|---|---|
| Mild (5.5-6.0) | Usually asymptomatic; may have vague GI symptoms |
| Moderate (6.1-6.9) | Nausea, vomiting, diarrhea; fatigue |
| Severe (>7.0) | Muscle cramps, generalized weakness, paresthesias, tetany, flaccid paralysis (ascending), dyspnea (if respiratory muscles involved), depressed deep tendon reflexes; hemodynamic instability, arrhythmias |
Key point: Cardiac arrest can be the very first "symptom." Symptoms are neither sensitive nor specific and do not reliably correlate with a particular serum K⁺ level.
ECG Changes (ordered by progressive severity)
The ECG is essential for assessing cardiotoxicity and guiding urgency of treatment:
| K⁺ Level | ECG Finding |
|---|---|
| >5.5-6.5 mEq/L | Peaked (tall, narrow, symmetric) T waves - most prominent in V2-V4 |
| >6.5-7.5 mEq/L | Prolonged PR interval, P wave flattening/disappearance, AV conduction delay |
| >7.0-8.0 mEq/L | QRS widening, bundle branch-like patterns |
| Severe | Sine wave (QRS merges with T wave), Brugada pattern, pseudoinfarction, ST elevation |
| Terminal | Ventricular fibrillation, PEA, asystole |
ECG 1: Severe hyperkalemia with wide QRS merging into T wave, absent P waves (sine wave pattern)
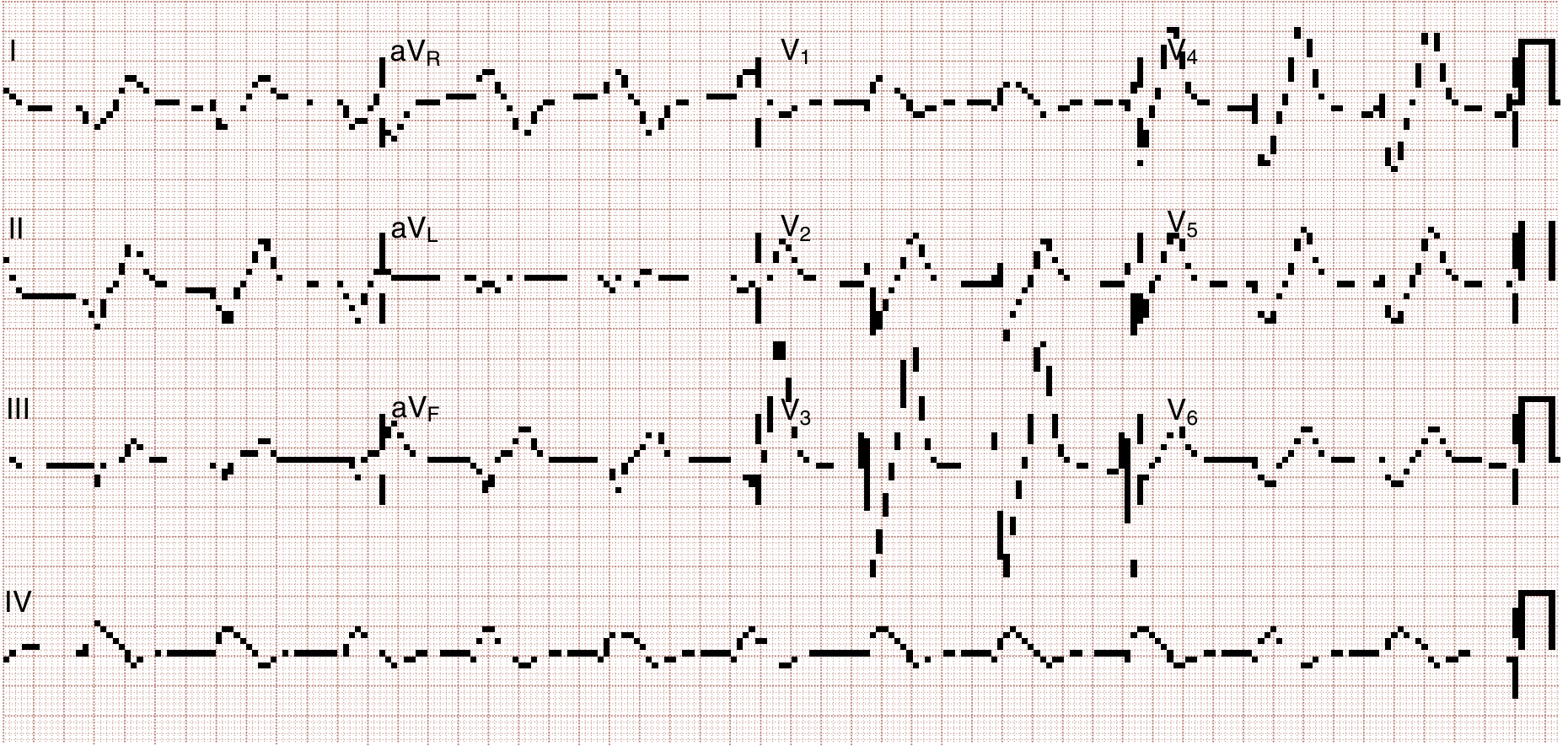
Fig. 114.1 from Rosen's Emergency Medicine - Hyperkalemia with QRS widening merging into T wave, absent P wave
ECG 2: After initial potassium-lowering therapy - tall peaked T waves still visible, P waves returning
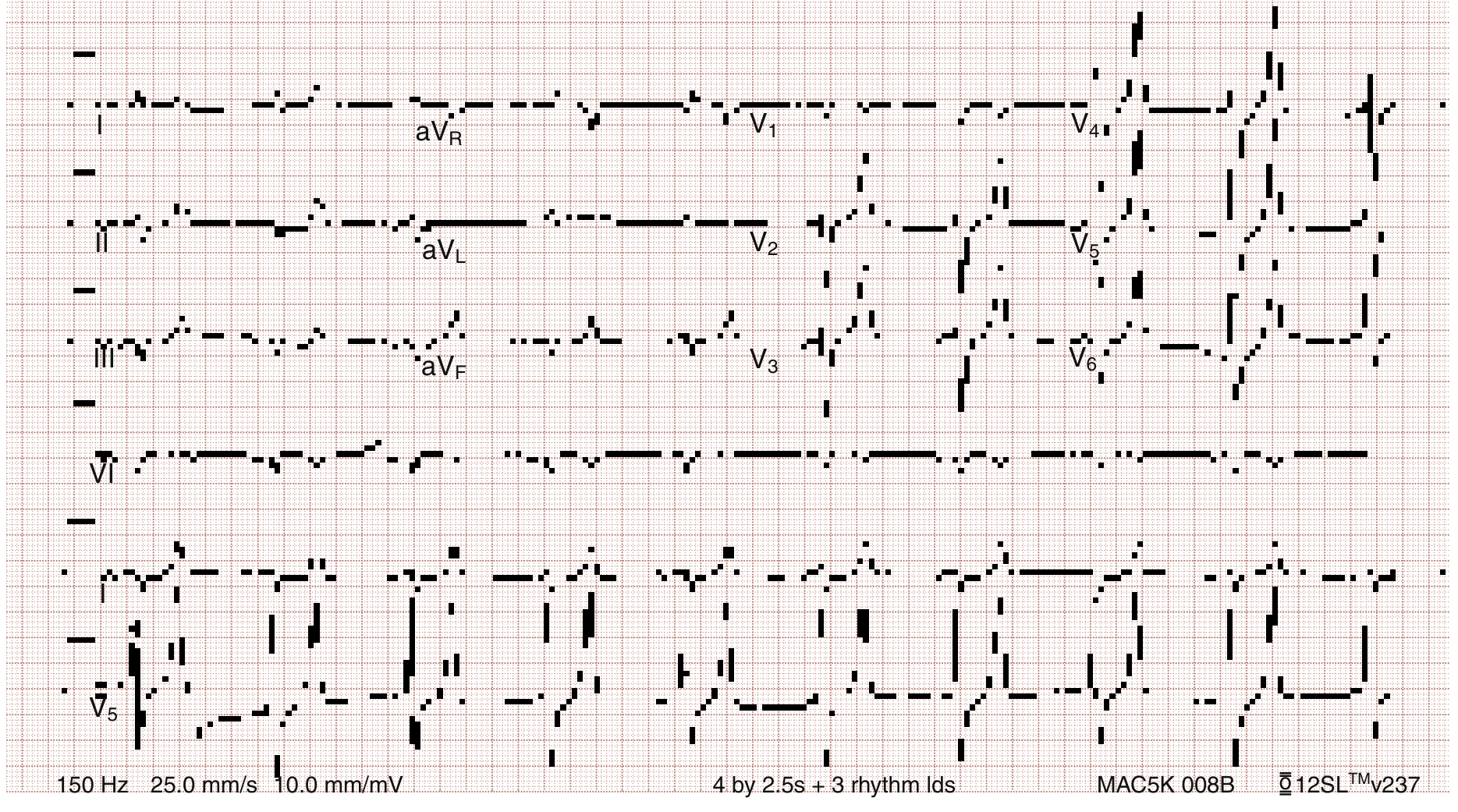
Fig. 114.2 from Rosen's Emergency Medicine - Same patient after potassium-lowering therapy has begun: tall peaked T waves, decreased P wave
Important: ECG changes appear in only about 50% of patients, so the absence of ECG changes does not exclude dangerous hyperkalemia. Hyperkalemia may also present as atropine-resistant bradycardia with or without heart block.
Management
Treatment is organized around three sequential and additive goals:
1. Stabilize the Cardiac Membrane
Calcium (Calcium Gluconate or Calcium Chloride)
| Drug | Dose | Route | Notes |
|---|---|---|---|
| Calcium gluconate 10% | 10-20 mL IV (1-2 g) over 2-3 min | Peripheral or central | Preferred; safer if extravasation occurs |
| Calcium chloride 10% | 5-10 mL IV (0.5-1 g) | Central vein preferred | 3× the calcium content of gluconate; risk of tissue necrosis if extravasates |
- Mechanism: Does NOT lower serum K⁺. Restores the electrical gradient by increasing the depolarization threshold and the calcium gradient across the cardiac membrane, thereby reducing myocyte excitability and narrowing the QRS.
- Onset: 1-3 minutes
- Duration: 30-60 minutes (transient - must be followed by K⁺-shifting agents)
- Repeat if no ECG improvement in 5-10 minutes
- Indication: ECG changes (peaked T waves that are rapidly evolving, absent P waves, wide QRS, sine wave, bradycardia, cardiac arrest attributed to hyperkalemia)
2. Shift Potassium into Cells (Temporizing - does NOT remove K⁺ from body)
a) Insulin + Glucose (most reliable agent)
| Component | Dose | Notes |
|---|---|---|
| Regular insulin | 10 units IV push (5 units if renal dysfunction) | Stimulates Na⁺/K⁺-ATPase pump |
| 50% Dextrose | 50 mL (25 g) IV push | To prevent hypoglycemia - omit in hyperglycemic patients |
- Onset: <15 minutes; peak effect: 30-60 minutes
- K⁺ reduction: ~0.6 mEq/L on average
- Monitor glucose closely for several hours post-therapy
b) Beta-2 Agonists (Nebulized Albuterol/Salbutamol)
- Dose: 10-20 mg nebulized continuously over 30-60 minutes (4× the normal bronchodilator dose)
- Mechanism: Stimulates Na⁺/K⁺-ATPase pump
- Onset: 15 minutes; K⁺ reduction: 0.5-1.0 mEq/L
- Additive to insulin: Combined insulin + albuterol lowers K⁺ by ~1.2 mEq/L on average
- Not reliable in all patients (some are albuterol-resistant)
c) Sodium Bicarbonate
- Dose: 50-100 mEq IV (or 3 ampules in 1 L of D5W as isotonic solution)
- Mechanism: Buffers H⁺ extracellularly; K⁺ shifts into cells in exchange
- Only effective in hyperkalemic patients with confirmed concurrent metabolic acidosis - no benefit in non-acidotic patients
- Use as an adjunct, not primary therapy
d) Normal Saline
- Even a few hundred mL can stimulate Na⁺/K⁺-ATPase
- Increases distal Na⁺ delivery to the kidney, promoting K⁺ excretion
- Use judiciously in anuric patients; consult nephrology
3. Remove Potassium from the Body (Definitive)
a) Hemodialysis (most effective and reliable)
- Removes K⁺ by at least 1 mEq/L in the first hour and another 1 mEq/L during the next 2 hours
- The only experimentally validated method of reliable K⁺ removal
- Indicated: life-threatening hyperkalemia with renal failure; failure of medical management
- Should be initiated early in patients with renal failure and severe hyperkalemia
- In patients with intact renal function, medical management alone is usually sufficient
b) Loop Diuretics (Furosemide)
- Enhance kaliuresis in patients with intact or recovering renal function
- Particularly useful in rhabdomyolysis or tumor lysis syndrome with intact urine output (combined with saline)
- Not effective acutely in anuric patients
c) Potassium Binders (Cation Exchange Resins)
| Drug | Dose | Notes |
|---|---|---|
| Patiromer (Veltassa) | 8.4 g in 100 mL water, once daily | Non-absorbed; newer; onset hours; chronic use |
| Sodium Zirconium Cyclosilicate (SZC) (Lokelma) | 10 g up to 3×/day (acute); 5-10 g/day (chronic) | Faster onset than patiromer; non-polymeric |
| Sodium Polystyrene Sulfonate (Kayexalate) | 15-30 g oral or 50 g rectal | Onset 4+ hours - NOT useful for acute management; GI adverse effects; bowel necrosis risk with sorbitol |
Important caveats on exchange resins in surgical patients (per Current Surgical Therapy):
- Oral Kayexalate is contraindicated in bowel obstruction
- Rectal administration is contraindicated in immunosuppressed patients
- The sorbitol vehicle in Kayexalate carries risk of bowel ischemia
- Patiromer and SZC are effective and safe for chronic/recurrent hyperkalemia, particularly in CKD and heart failure patients on RAASi therapy
A 2025 systematic review and meta-analysis (PMID 40542996) confirmed that patiromer and SZC effectively reduce K⁺ and allow maintenance or up-titration of RAAS inhibitors in CKD and heart failure patients.
Summary Treatment Algorithm
Suspected Hyperkalemia
↓
Establish IV access + continuous cardiac monitoring
Obtain ECG + serum K⁺ + blood gas
↓
ECG changes present? ──YES──→ CALCIUM GLUCONATE IV (Step 1)
│ (10-20 mL of 10% over 2-3 min)
│
Both paths proceed to:
↓
SHIFT K⁺ INTO CELLS (Step 2) - effects additive:
• Insulin 10 units IV + 50% dextrose 50 mL IV
• Nebulized albuterol 10-20 mg
• NaHCO₃ if acidotic
↓
REMOVE K⁺ FROM BODY (Step 3):
• Furosemide (if urine output present)
• Patiromer or SZC (chronic/maintenance)
• Hemodialysis (renal failure or refractory severe hyperkalemia)
↓
Address underlying cause + chronic prevention
(dietary restriction, correct acidosis, review offending drugs,
optimize RAASi with K⁺ binder if tolerated)
Chronic Management and Prevention
- Dietary restriction: Avoid salt substitutes, dried fruits, nuts, bananas, potatoes, tomatoes, spinach, canned fruit/vegetable juices. Boil vegetables rather than steaming.
- Correct metabolic acidosis: Oral sodium bicarbonate or citrate.
- Optimize diuresis: Thiazide or loop diuretics if residual renal function allows.
- Exogenous mineralocorticoid: In hypoaldosteronism states (fludrocortisone).
- Reassess medications: Stop or reduce ACE inhibitors/ARBs, NSAIDs, K-sparing diuretics when clinically safe.
- RAASi management (2025 GUARDIAN-HK European Guidelines, PMID 40685253): Disease-modifying therapies such as RAASi should not simply be stopped when hyperkalemia occurs. Instead, use patiromer or SZC to maintain RAASi at target doses, particularly in heart failure and CKD patients, because the cardiorenal benefits outweigh the risk.
Key Sources
- Rosen's Emergency Medicine (pp. 2113-2205) - Clinical features, ECG classification, management table
- Washington Manual of Medical Therapeutics (pp. 2700-2761) - Causes, diagnosis, treatment doses
- Current Surgical Therapy, 14th ed. (pp. 3136-3143) - Surgical population specifics
- Fischer's Mastery of Surgery, 8th ed. (p. 1405) - Acute treatment summary
- PMID 40685253 - GUARDIAN-HK 2025 European interdisciplinary recommendations on recurrent hyperkalemia (note: erratum published, PMID 41637058)
- PMID 40542996 - Novel potassium binders (patiromer, SZC) systematic review and meta-analysis, 2025
Discuss use of drains in surgical practice.
Finding Sources
Searching PubMed
surgical drains drainage indications evidence
Searching the Web
surgical drains use indications types evidence 2024 2025 review
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive and well-sourced material from three major surgical textbooks plus current literature. Let me now compose the full answer.
Surgical Drains: Classification, Uses, and Evidence-Based Practice
Historical Perspective
The use of surgical drains dates back centuries. In 1887, Lawson Tait famously declared "When in doubt, drain!" - a maxim that governed surgical practice for much of the 20th century. This philosophy has since been critically re-examined. The modern approach has moved decisively away from routine prophylactic drainage toward selective, evidence-based use.
Definition and Purpose
A surgical drain is a tube or device placed in a wound, body cavity, or potential space to allow the egress of fluid (blood, serum, pus, bile, lymph, urine, intestinal contents, air, or pancreatic secretions) to the surface. Their use can be:
- Prophylactic - placed at the end of a clean or elective procedure to prevent anticipated fluid accumulation
- Therapeutic - placed to treat an existing collection (abscess, haematoma, bile leak)
Classification of Surgical Drains
The fundamental classification is based on whether the system is open or closed, and whether it uses active (suction) or passive (gravity/capillary) drainage.
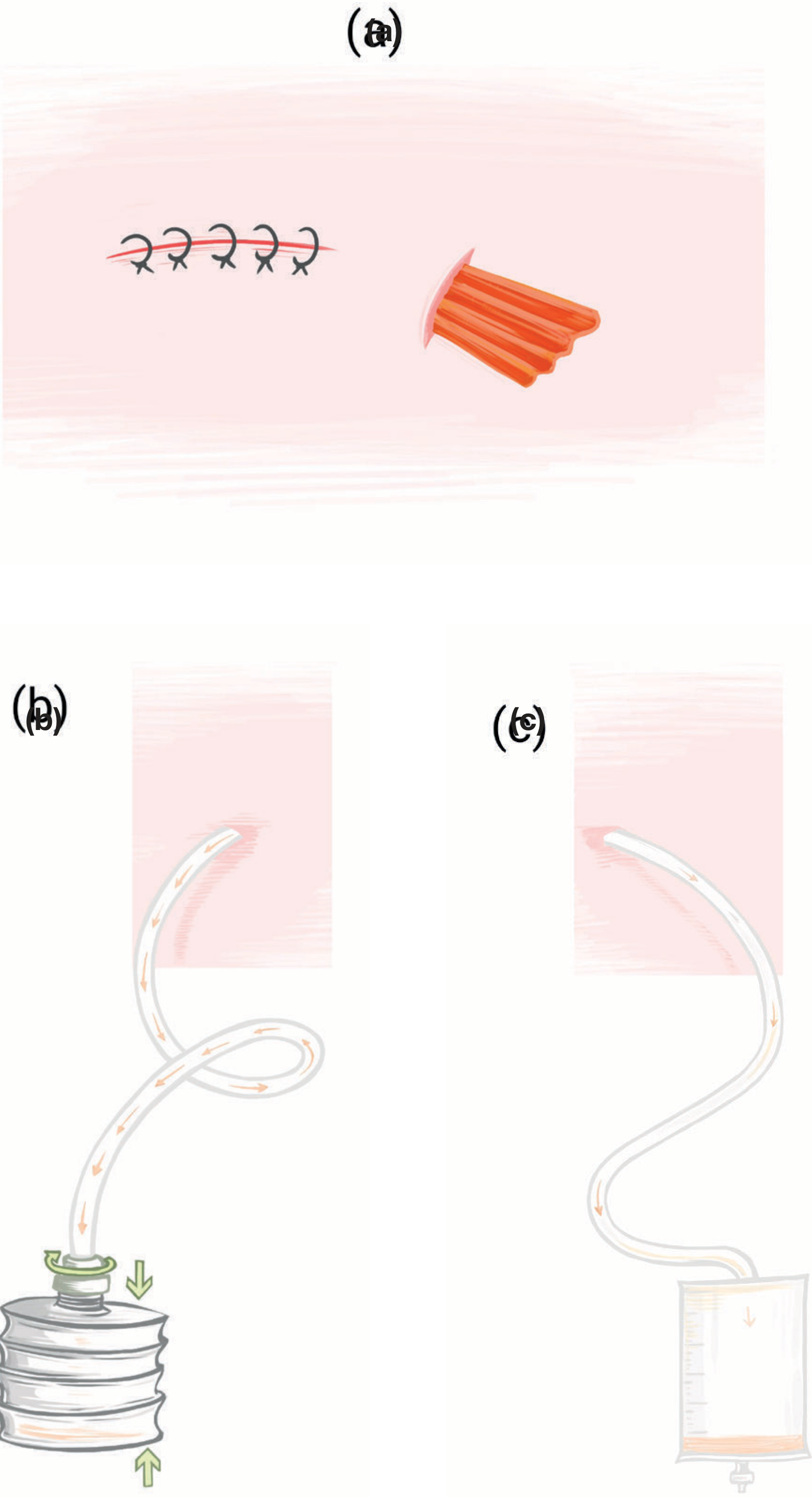
Figure from Bailey and Love's Short Practice of Surgery, 28th ed. - (a) Open corrugated drain, (b) Closed suction drain with vacuum-assisted system, (c) Closed non-suction drain (Robinson-type) for abdominal drainage
1. Open Drains (Passive)
Aid passive drainage of a cavity by forming a channel between the body and the external environment, relying on gravity. They are associated with frequent dressing changes, poor cosmesis, and a risk of ascending bacterial colonisation.
- Corrugated drain: A flat, ribbed latex or rubber sheet that creates channels for passive fluid egress. Used in debrided wounds and abscess cavities.
- Penrose drain: A soft, flexible latex or silicone rubber tube available in ¼ to 1 inch diameters; can be cut to length; sutured to skin to prevent migration. Has no collection reservoir - drains into external dressings. Used in scrotal surgery and for subcutaneous fluid prevention during wound closure. Associated with a higher risk of surgical site infection compared to closed systems and therefore removed earlier.
2. Closed Non-Suction Drains (Passive)
Use capillary action and gravity. Connected to a collection bag or reservoir.
- Robinson's drain: A simple soft tube with multiple side holes used within the abdominal cavity to evacuate fluid without the negative pressure hazard of sucking viscera or omentum into the drain. Connected to a drainage bag.
- Urinary catheters and nasogastric tubes are considered specific examples of passive closed drains.
- Pigtail drain: Contains a curled inner portion (deployed by tightening a suture after placement) with small perforations for fluid removal that keep the drain in position. Used for nephrostomy, suprapubic drainage, percutaneous abscess drainage, and pleural collections. Removal requires loosening of the internal suture or transection of the drain to unfurl the coil.
3. Closed Suction Drains (Active)
Maintain negative pressure, actively suctioning fluid and obliterating dead space. Preferred when accurate quantification of drainage volume is needed or when early detection of small amounts of fluid is important.
-
Jackson-Pratt (JP) drain: A flat or round perforated internal tube connected to a grenade-shaped compressible bulb. The bulb is compressed to create low negative pressure (~70-170 mmHg). Widely used for intra-abdominal urologic, gynaecologic, and general surgical procedures. The perforated collecting portion is larger than the external tubing, which can cause some discomfort on removal.
-
Blake drain: Similar to JP in principle but uses continuous-diameter tubing with longitudinal channels that allow fluid entry via capillary action and negative pressure, rather than side perforations. The uniform diameter may be less uncomfortable during removal. Commonly used in abdominal surgery.
-
Redivac (Hemovac): A high-negative-pressure drain used where larger volumes of fluid are anticipated (e.g., after major orthopaedic or vascular procedures). The reservoir is a flat coil-spring container.
-
Wound drain with suction: Various proprietary designs used in head and neck surgery, axillary dissection, and after ventral hernia repair.
-
T-tube: A specialised T-shaped drain inserted into the common bile duct (CBD) after exploration and stone retrieval, or after repair of a damaged CBD. The horizontal limb sits within the duct; the vertical limb exits externally. It:
- Drains bile while the sphincter of Oddi is in spasm postoperatively
- Acts as a safety valve if stones are retained distally
- Allows T-tube cholangiography to confirm clearance before removal
- Must remain in situ for at least 2-3 weeks to allow a fistulous tract to form, minimising the risk of biliary peritonitis on removal
- Before removal: T-tube cholangiogram confirms free bile flow to duodenum; then clamp for 24 hours; if asymptomatic, remove
- Note: A Cochrane analysis found T-tubes are associated with increased bile leakage, prolonged hospital stay, and cost, with minimal benefit over primary CBD closure
-
Campbell-Walsh Wein Urology (pp. 1337-1360); Bailey and Love's Short Practice of Surgery, 28th ed. (pp. 8694-8903)
Schwartz's Four Indications for a Surgical Drain
Schwartz's Principles of Surgery, 11th ed. (p. 452) identifies four clear indications:
- To collapse surgical dead space in areas of redundant tissue (e.g., neck, axilla)
- To provide focused drainage of an abscess or grossly infected surgical site
- To provide early warning of a surgical leak (bowel contents, secretions, urine, air, or blood) - the so-called "sentinel drain"
- To control an established fistula leak
Arguments For and Against Routine Drainage
Bailey and Love's Short Practice of Surgery, 28th ed. (p. 8731-8748) summarises the ongoing debate:
Arguments FOR drain use
- Removes collections of purulent material, blood, serous fluid, bile, chyle, pancreatic or intestinal secretions
- Acts as a sentinel signal for postoperative haemorrhage or anastomotic leakage
- Provides a track for long-term drainage and fistula control
Arguments AGAINST routine drain use
- Increases intra-abdominal and wound infection by introducing skin bacteria into the peritoneal cavity (retrograde contamination)
- Delays recovery and increases hospital stay
- Increases abdominal pain
- Decreases pulmonary function (by splinting)
- Can create a false sense of security - a blocked drain may give no output while a significant collection forms
- Active suction (70-170 mmHg negative pressure) may itself promote anastomotic dehiscence by creating suction injury at the anastomotic line - raising the question of whether it is the drain or the anastomosis that fails first
- Schwartz's Principles of Surgery specifically states that "data do not support closed suction drainage to 'protect an anastomosis' or to 'control a leak' when placed at the time of surgery"
Evidence-Based Use by Surgical Procedure
Non-Gastrointestinal Surgery
| Procedure | Evidence-Based Recommendation |
|---|---|
| Thyroid surgery | Avoid routine drain placement |
| Breast lumpectomy | Avoid routine drain placement |
| Inguinal hernia repair | Avoid routine drain placement |
| Modified/radical neck dissection | Consider routine drain (dead space obliteration) |
| Parotid surgery | Consider routine drain (prevent sialocele) |
| Axillary dissection ± mastectomy | Consider routine drain (prevent seroma/lymphocele) |
| Inguinal lymphadenectomy | Consider routine drain |
| Ventral hernia repair (obese patients) | Consider routine drain |
| Simple mastectomy | Drain placed; removed when output <30 mL for two consecutive days (typically POD 7-14) |
Gastrointestinal Surgery
| Procedure | Evidence-Based Recommendation |
|---|---|
| Colonic surgery | Avoid routine drain |
| Small bowel resections | Avoid routine drain |
| Hepatic resections | Avoid routine drain |
| Laparoscopic cholecystectomy | Avoid routine drain |
| Oesophageal surgery | Consider routine drain (high anastomotic leak rate) |
| Major pancreatic resection (Whipple's) | Consider routine drain (pancreatic fistula surveillance) |
| Rectal surgery | Selective use |
| Gastric resections | Selective use |
Bailey and Love's Short Practice of Surgery, 28th ed. (Summary boxes 7.10 and 7.11)
Emergency Gastrointestinal Surgery
- Four-quadrant peritoneal contamination: Routine drainage generally beneficial
- Localised peritoneal contamination: More selective approach is appropriate
- The decision must account for clinical state, comorbidities, and availability of round-the-clock interventional radiology for percutaneous drainage if needed
Specific Specialist Uses
Nasogastric Drainage
ERAS (Enhanced Recovery After Surgery) pathways now prohibit prophylactic use of nasogastric tubes in elective abdominal surgery. Selective indications remain:
- Conservative management of paralytic ileus or partial bowel obstruction
- Decompression of stomach before emergency laparotomy
- When postoperative ileus is anticipated after extensive bowel handling
- Feeding route after upper aerodigestive tract procedures
Contraindications: Base of skull fracture, oesophageal stricture/recent oesophageal surgery
Vacuum-Assisted Closure (VAC/NPWT)
Negative Pressure Wound Therapy is a form of active drainage applied to open wounds. A sterile foam or gauze dressing is sealed with film and placed under controlled suction (-125 mmHg typically) for 2-4 days at a time. It:
- Decreases local wound oedema
- Promotes granulation tissue formation
- Dramatically improves complex wound healing
- Effectively manages contaminated wounds, fasciotomy sites, abdominal wound dehiscence, and open fractures
- Exposed dura is not a contraindication
Chest Drains (Intercostal Drains)
Used after thoracic surgery, trauma (haemothorax, pneumothorax), empyema, pleural effusion, and oesophageal surgery. Connected to underwater seal drainage systems. Digital drain systems with electronic flow monitoring are increasingly used and have been shown to shorten drain removal time.
Percutaneous Image-Guided Drains
CT- or ultrasound-guided percutaneous drain placement is the current standard of care for:
- Intra-abdominal and pelvic abscesses
- Loculated infections
- Bilomas, urinomas, lymphoceles
- Drainage of anastomotic leaks This has largely replaced formal surgical re-exploration for accessible fluid collections.
Complications of Surgical Drains
| Complication | Notes |
|---|---|
| Ascending infection/surgical site infection | Retrograde bacterial colonisation through drain track; especially with open drains |
| Drain blockage | Creates false reassurance; drain tip may become plugged with clot, fibrin, or omentum |
| Drain migration | Can migrate inward or outward; always suture to skin |
| Anastomotic disruption | Suction drains placed adjacent to anastomoses may promote leakage |
| Visceral/vascular erosion | Pressure necrosis from long-term drain placement adjacent to bowel or vessels |
| Pain and restricted mobility | Increases post-operative discomfort; may impair respiratory effort |
| Prolonged hospital stay | Patients often not discharged until drain is removed |
| Retained drain | Rare; requires surgical removal |
| Biliary peritonitis after T-tube removal | If removed before adequate tract formation (<2-3 weeks) |
Principles of Drain Removal
- A drain should be removed as soon as its defined objective is achieved - not based on arbitrary volume thresholds alone
- Sentinel (haemostasis) drains: Usually removable at 24 hours if no bleeding
- Infection drains: Remove when infection is subsiding and drainage is minimal
- Post-anastomotic drains: Remove at 3-5 days (they do not prevent anastomotic leak but may allow controlled external drainage if one occurs)
- Closed suction drains: Release the suction before removal to prevent tissue trauma
- T-tubes: Clamp for 24 hours prior to removal after confirming patent cholangiogram; leave in situ minimum 2-3 weeks
- Mastectomy drains: Remove when output <30 mL/day for two consecutive days (typically POD 7-14)
- Longer drain dwell increases infection risk through retrograde bacterial contamination
Summary
The philosophy of surgical drainage has evolved from the blanket "when in doubt, drain" to a targeted, evidence-based approach. Modern consensus is:
- Therapeutic drainage of established collections (abscess, haematoma, bile leak) is strongly supported and increasingly performed percutaneously under image guidance
- Prophylactic drainage of clean anastomoses, standard elective colonic, hepatic, and biliary procedures is not routinely indicated and may cause harm
- Selective drainage is appropriate for high-risk anastomoses (oesophageal, pancreatic), major contaminated procedures, and operations creating large dead spaces (neck dissection, axillary surgery)
- ERAS protocols have eliminated many traditional drainage practices (routine NG tubes, routine pelvic drains) from elective surgery
Key Sources
- Bailey and Love's Short Practice of Surgery, 28th ed. (pp. 8694-8903) - Classification, controversy, procedure-specific guidelines, T-tubes, nasogastric drainage, drain removal
- Schwartz's Principles of Surgery, 11th ed. (p. 452) - Four indications for surgical drains; VAC therapy
- Campbell-Walsh Wein Urology (pp. 1337-1360) - Penrose, Jackson-Pratt, Blake, pigtail drain descriptions
- Mulholland and Greenfield's Surgery, 7th ed. (p. 3107-3110) - Mastectomy drain management
- PMID 41246741 (2025 narrative review) - Drain removal timing, criteria, and evidence-based practices
How will you diagnose and evaluate a patient with non healing ulcer of foot?
Finding Sources
Finding Sources
Searching PubMed
diabetic foot ulcer diagnosis assessment management
Searching the Web
non-healing foot ulcer diagnosis evaluation approach 2024 2025 guidelines
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have thorough, well-sourced content from multiple authoritative textbooks. Let me now compile the comprehensive answer.
Diagnosis and Evaluation of a Non-Healing Foot Ulcer
Epidemiology and Significance
A non-healing foot ulcer is defined as one failing to show measurable healing progression after 4 weeks of standard care. The lifetime risk of developing a diabetic foot ulcer (DFU) is 19-34%, with ulcer recurrence rates of 30-60% per year once an initial ulcer occurs. Globally, 9-26 million people develop DFUs annually. Critically, a new diabetic foot ulcer carries a 44% five-year mortality rate with a mean survival of only 50 months after onset - prognosis comparable to several cancers. Ulcers infected with ischaemia are 90 times more likely to result in amputation compared to clean, non-ischaemic ulcers.
- Campbell's Operative Orthopaedics, 15th ed. 2026 (p. 5054-5061)
Step 1: Establish the Aetiology - The Differential Diagnosis
The first task is determining the predominant cause, as management differs completely:
| Type | Location | Appearance | Pain | Key Feature |
|---|---|---|---|---|
| Neuropathic | Plantar surface, pressure points, callus sites | Punched-out, painless, surrounded by callus | Absent (analgesia) | Peripheral neuropathy, diabetic |
| Ischaemic (arterial) | Toes, metatarsal heads, shins, heel | Pale/necrotic base, irregular edges, no granulation | Severe (rest pain) | Cold foot, absent pulses, PAD |
| Venous | Above medial/lateral malleolus (gaiter area) | Irregular, sloughy, moderate exudate | Mild (aching) | Oedema, varicosities, lipodermatosclerosis |
| Mixed | Variable | Features of both | Variable | Coexisting PAD + neuropathy (common in diabetics) |
| Pressure/decubitus | Heel, bony prominences | Staging I-IV | Variable | Immobility, hospitalised patient |
| Malignant (Marjolin's ulcer) | Any site, longstanding | Raised/everted edges, bleeds easily | Variable | Squamous cell carcinoma arising in a chronic wound |
| Infective | Any site | Sloughy, purulent | Variable | Osteomyelitis, Charcot foot |
Step 2: History Taking
A. Ulcer-Specific History
- Duration - how long has it been present? Any previous episodes?
- Mode of onset - trauma, spontaneous, minor injury unnoticed due to neuropathy
- Pain - painless ulcers suggest neuropathy; severely painful suggest ischaemia
- Prior treatments - antibiotics, dressings, offloading, surgery
- Rate of progression - stable, growing, improving
B. Systemic and Medical History
Diabetes mellitus (most important background condition):
- Duration and type of diabetes
- Current glycaemic control (HbA1c)
- History of neuropathy (paresthesias, numbness, burning) - patients may deny any pain or trauma preceding the ulcer
- History of prior foot ulcers or amputations (strongest single predictor of recurrence)
- Known retinopathy or nephropathy (renal failure dialysis patients are especially high-risk)
- Impaired vision (reduces self-inspection ability)
Vascular history:
- Symptoms of peripheral arterial disease: intermittent claudication, rest pain
- Coronary artery disease, cerebrovascular disease (marker of systemic atherosclerosis)
- Prior vascular interventions (angioplasty, bypass)
Other relevant conditions:
- Venous insufficiency, deep vein thrombosis, varicose veins
- Rheumatoid arthritis, vasculitis, Raynaud's disease
- Malignancy (both as immunosuppressant and direct cause via Marjolin's ulcer)
- Immunosuppression (steroids, chemotherapy, transplant drugs)
- Smoking (major vascular risk factor)
C. Medications
- NSAIDs (impair healing, reduce pain perception)
- Steroids (suppress immune response and healing)
- Anticoagulants
- Immunosuppressants
Step 3: Physical Examination
A. General Assessment
- Vital signs: fever, tachycardia, hypotension (systemic sepsis from severe infection)
- Overall nutritional state, BMI
- Signs of systemic disease (diabetes signs, renal disease)
B. Inspect the Patient's Footwear (before removing shoes)
- Undersized shoes create pressure over bony prominences
- Toe box inadequate for forefoot deformities (claw toes, hammer toes)
- Abnormal wear pattern = structural or dynamic foot deformity
- Prominent seams or foreign bodies inside shoe that patient cannot feel = strong neuropathy sign
C. Local Examination of the Ulcer
Site and size:
- Plantar surface / pressure points → neuropathic
- Over metatarsal heads / toes / shins → ischaemic
- Medial/lateral malleolus (gaiter region) → venous
- Measure dimensions in cm (length × width × depth)
- 96% of ulcers <1 cm² heal without amputation vs. only 72% of those >3 cm² (Ince et al.)
- Ulcers showing ≥50% reduction in 4 weeks have significantly better 12-week healing
Ulcer base:
- Granulating (healthy, red) vs. sloughy (yellow/grey) vs. necrotic/eschar (black)
- Exposed tendon (Wagner grade II), exposed bone (Wagner III)
Edges:
- Punched-out, undermined, with surrounding callus → neuropathic
- Sloping, irregular → healing or venous
- Raised, everted, firm, bleeds easily → suspect malignancy (Marjolin's ulcer)
Surrounding skin:
- Shiny, taut skin without hair growth → peripheral arterial disease
- Dry, scaly skin → autonomic neuropathy (anhidrosis)
- Erythema, swelling, calor → infection/cellulitis (measure extent from ulcer edge)
- Lipodermatosclerosis, haemosiderin staining, varicosities → venous disease
- Corns or calluses → precursors to ulcer formation from abnormal pressure
Wound assessment with probe-to-bone test:
- Insert a sterile, blunt metallic probe into the ulcer
- A hard, gritty sensation on contact = positive probe-to-bone → strong indicator of osteomyelitis
- Sensitivity 60%, Specificity 91%, LR+ 6.4
- Positive predictive value ~90% in hospitalised diabetics with chronic deep foot ulcers
Clinical photographs at each visit to document progression
D. Foot Deformity Assessment
- Claw toes, hammer toes → motor neuropathy (intrinsic muscle wasting)
- Fat pad migration distally (normal fat pad displaced from metatarsal heads)
- Rocker-bottom deformity → Charcot neuroarthropathy (midfoot collapse)
- Hallux valgus, prominent metatarsal heads
- Hindfoot alignment with weight bearing (varus/valgus)
- Atrophy of extensor digitorum brevis → motor neuropathy
E. Vascular Examination
- Inspection: colour (pallor, cyanosis, rubor), hair loss, shiny skin, nail dystrophy, gangrene
- Elevation test: elevation pallor; dependent rubor (Buerger's test)
- Temperature: warm foot = infection or neuropathy; cold foot = ischaemia
- Pulses: femoral, popliteal, dorsalis pedis, posterior tibial - absence indicates PAD
- Capillary refill time (>3 seconds = impaired perfusion)
F. Neurological Examination (Neuropathic Foot)
Semmes-Weinstein 10g monofilament test (most clinically important):
- Inability to feel a 5.07 monofilament (10g pressure) is one of the most predictive risk factors for foot morbidity
- Standard testing: 10 sites on the plantar foot
- Quick alternative: 4.5g monofilament beneath both first metatarsal heads gives equivalent results
- "You cannot examine the feet of your diabetic patients too often, and you cannot examine them with their shoes on!"
Other neurological tests:
- Vibration sense: 128 Hz tuning fork at first MTP joint and medial malleolus
- Proprioception testing
- Deep tendon reflexes (absent ankle reflex = peripheral neuropathy)
- Two-point discrimination
Gastrocnemius contracture test (Silfverskiöld test):
- Reduced ankle dorsiflexion with knee in extension (but not in flexion) = gastrocnemius contracture
- Equal reduction in both positions = Achilles tendon contracture
- Both increase forefoot pressure loading, predisposing to ulceration
Step 4: Ulcer Classification
Wagner-Meggitt Classification (most widely used)
| Grade | Description |
|---|---|
| 0 | Skin at risk - no ulceration present |
| I | Superficial ulcer, skin and subcutaneous tissue only |
| II | Deep ulcer - exposed tendon or joint capsule |
| III | Deep ulcer with abscess or osteomyelitis |
| IV | Partial gangrene (forefoot) |
| V | Extensive gangrene requiring major amputation |
Wagner Grade I - superficial ulcer:

Fig 91.4 - Campbell's Operative Orthopaedics 2026: Superficial (Wagner grade I) ulcer
Wagner Grade II - deep ulcer with exposed tendon and joint capsule:

Fig 91.5 - Campbell's Operative Orthopaedics 2026: Deep (Wagner grade II) ulcer with exposed tendon and joint capsule
Brodsky Depth-Ischaemia Classification (adds vascular assessment)
| Depth | Description |
|---|---|
| 0 | At-risk foot, no ulceration |
| 1 | Superficial ulceration, no infection |
| 2 | Deep ulceration, tendons or joint exposed |
| 3 | Extensive ulceration or abscess |
| Ischaemia | Description |
|---|---|
| A | Not ischaemic |
| B | Ischaemia without gangrene |
| C | Partial forefoot gangrene |
| D | Complete gangrene |
This creates a grid (e.g. Grade 2B = deep ulcer with ischaemia). Grades IV and V in the Wagner system correspond to ischaemic ulcers in the Brodsky system.
IDSA/IWGDF Infection Severity Classification
| Grade | Features |
|---|---|
| Mild | ≥2 local signs (swelling, erythema ≤2 cm, warmth, tenderness, purulence); skin/subcutaneous only; no systemic signs |
| Moderate | Erythema >2 cm from ulcer, OR deep structure involved (abscess, osteomyelitis, septic arthritis, fasciitis); no SIRS |
| Severe | Local infection + ≥2 SIRS criteria: T >38°C or <36°C; Pulse >90 bpm; RR >20; WBC >12,000 or <4,000 |
Step 5: Investigations
A. Vascular Assessment
Ankle-Brachial Index (ABI) - mandatory for all patients with foot ulcers:
- Normal: 0.9 - 1.2
- Values >1.3 = non-compressible (calcified) vessels - falsely elevated in diabetics
- ABI <0.5 = ulcer unlikely to heal without vascular intervention
- Ankle systolic pressure >60 mmHg (diabetics need >90 mmHg) required for healing
- ABI difference >0.15 between limbs = significant, warrants further investigation
Toe-Brachial Index (TBI) - preferred in diabetics with calcified tibial vessels:
- Normal toe/brachial index: >0.7
- Toe pressure >40 mmHg = associated with wound healing
- Absolute toe pressure should be >70 mmHg for healing
Doppler waveform analysis:
- Triphasic = normal
- Biphasic = moderate PAD
- Monophasic = severe PAD
Duplex ultrasound - maps the arterial tree, identifies stenoses and occlusions
CT angiography / MR angiography - detailed anatomical roadmap for revascularisation planning
Transcutaneous oxygen pressure (TcPO₂):
-
40 mmHg = adequate perfusion for healing
- <20 mmHg = severe ischaemia, healing unlikely
B. Neurological Assessment
- Semmes-Weinstein monofilament (10g) - primary screening tool
- Neurothesiometer/biothesiometer - quantifies vibration perception threshold (VPT >25 V = high risk)
- Nerve conduction studies/electromyography - reserved for complex cases (rarely needed in routine practice)
C. Laboratory Investigations
| Test | Purpose |
|---|---|
| HbA1c | Glycaemic control; >7% = independent risk factor for DFU; higher HbA1c predicts complications and non-healing |
| Fasting glucose / random glucose | Acute glycaemic state |
| FBC (CBC) | Leucocytosis (infection); anaemia (impairs wound healing) |
| ESR | ESR >70 mm/h strongly suggestive of osteomyelitis (LR+ = 11) |
| CRP | Marker of infection/inflammation; useful for baseline and treatment response |
| Urea, creatinine, eGFR | Renal function - diabetic nephropathy, renal failure patients are very high-risk |
| Serum albumin | Nutritional status; hypoalbuminaemia impairs healing |
| Serum zinc, vitamin C | Nutritional cofactors for wound healing if deficiency suspected |
| Wound cultures | See below |
D. Microbiological Assessment
Rules for culturing diabetic foot ulcers (Symptom to Diagnosis, 4th ed.):
- Do NOT culture clinically uninfected ulcers - commensal bacteria will mislead
- Do NOT swab the wound surface - superficial swabs are unreliable for identifying deep organisms
- Cleanse and debride the wound first before obtaining the specimen
- If purulent secretions present: aspirate with a sterile needle/syringe
- Gold standard: tissue specimen by scraping the base of the debrided ulcer with a sterile scalpel or dermal curette
- Deep infections: bone biopsy (see below)
Expected microbiology by infection severity:
- Mild/acute infections: Usually monomicrobial - Staphylococcus aureus, Streptococcus spp.
- Moderate: S. aureus, Streptococcus, Enterobacteriaceae, anaerobes
- Severe/chronic infections: Polymicrobial (3-5 isolates) including anaerobes; gram-negative organisms (including Pseudomonas) overrepresented
- MRSA present in at least 15-30% of foot ulcers
E. Imaging
Plain Radiograph (first-line, always obtain)
Indicated when: ulcer extends beyond skin; gas in soft tissues; bone exposure; positive probe-to-bone test; or at initial assessment of any significant ulcer.
Look for:
- Demineralisation, loss of normal bone trabecular pattern
- Periosteal reaction
- Cortical erosion, destruction of joint spaces
- Gas in soft tissues (gas-forming organisms)
- Charcot arthropathy (joint destruction, fragmentation, subluxation)
- Foreign bodies
Limitations: Sensitivity only 54%, specificity 68% for osteomyelitis (LR+ 2.3, LR- 0.63). Early osteomyelitis may not be visible for 2-4 weeks.
MRI (investigation of choice for suspected osteomyelitis)
- Sensitivity 90%, Specificity 79% (LR+ 5.1, LR- 0.12)
- Most accurate imaging test for osteomyelitis in the diabetic foot
- Findings: decreased T1 signal, increased T2/STIR signal in bone marrow
- Distinguishes soft tissue infection, abscess, septic arthritis from osteomyelitis
- Useful for surgical planning once diagnosis confirmed
- Limitation: differentiating osteomyelitis from Charcot arthropathy can be difficult
- Weight-bearing radiographs → MRI if soft-tissue abscess or osteomyelitis suspected
CT Scanning
- Shows bone architecture in multiple planes, sequestra, cortical disruptions
- Useful for surgical planning for deformity correction
- Not routinely used in isolation for evaluation; weight-bearing CT excellent for Charcot planning
Bone Scintigraphy
| Scan Type | Sensitivity | Specificity | Notes |
|---|---|---|---|
| Three-phase bone scan (Tc-99m) | 81% | 28% | Not specific; Charcot causes false positive |
| Leukocyte scan (In-111/Tc-99m WBC) | 74% | 68% | More specific than bone scan |
| SPECT/CT (Tc-99m WBC) | High | Higher | Emerging technique; limited evidence |
Scintigraphy useful when MRI is contraindicated.
PET/CT
- FDG-PET shows increased uptake at sites of active inflammation
- Mixed evidence vs. MRI; insufficient evidence to recommend routine use currently
Complete Imaging Summary for Osteomyelitis (Table 91.3 - Campbell's Orthopaedics):
| Diagnostic Modality | Sensitivity (%) | Specificity (%) |
|---|---|---|
| Probe-to-bone/exposed bone | 60 | 91 |
| Radiography | 54 | 68 |
| MRI | 90 | 79 |
| Bone scan | 81 | 28 |
| Leukocyte scan | 74 | 68 |
F. Diagnosing Osteomyelitis - Evidence-Based Approach
| Finding | LR+ | LR- | Interpretation |
|---|---|---|---|
| Bone exposure on inspection | 9.2 | 0.7 | Very suggestive |
| Ulcer area >2 cm² | 7.2 | 0.48 | Moderate-high risk |
| Positive probe-to-bone | 6.4 | 0.39 | Strongly suggestive |
| ESR >70 mm/h | 11 | 0.34 | High LR+ and LR- |
| MRI positive | 5.1 | 0.12 | Best negative predictive test |
| Plain radiograph positive | 2.3 | 0.63 | Moderate |
| Ulcer inflammation | 1.5 | 0.84 | Not discriminatory |
Osteomyelitis develops in 20% of mild infections and 50-60% of moderate-to-severe infections.
Gold standard for osteomyelitis diagnosis: Open bone biopsy with culture and histopathology
- Needle bone biopsy: sensitivity 87%, specificity 93% (LR+ 12.4, LR- 0.14) but subject to sampling error
Diagnosis is clinically confirmed by the combination of:
- Probe-to-bone positive, AND
- Elevated inflammatory markers, AND
- Abnormal plain radiograph
Step 6: Multidisciplinary Assessment
A non-healing foot ulcer optimally requires input from:
| Specialist | Role |
|---|---|
| Diabetologist / Endocrinologist | Glycaemic optimisation, systemic disease management |
| Vascular surgeon / Interventional radiologist | PAD assessment, revascularisation (angioplasty/bypass) |
| Orthopaedic/Podiatric surgeon | Deformity correction, debridement, amputation level |
| Infectious disease | Complex antibiotic management, osteomyelitis |
| Wound care nurse / Podiatrist | Wound dressing, offloading, patient education |
| Nutritionist | Nutritional optimisation |
| Nephrologist | If dialysis-dependent (extremely high-risk group) |
Step 7: Assessment of Factors Impairing Healing
| Factor | Assessment |
|---|---|
| Glycaemic control | HbA1c; target <7% |
| Nutritional status | Albumin, pre-albumin, BMI |
| Ischaemia | ABI, TBI, TcPO₂ |
| Infection | Clinical grade, cultures, inflammatory markers |
| Osteomyelitis | Probe-to-bone, ESR/CRP, MRI |
| Offloading | Is pressure being adequately relieved? |
| Footwear | Correct fit and pressure distribution |
| Patient adherence | Compliance with dressings and offloading |
Key Prognostic Points
- Ulcers ≥50% reduced in area after 4 weeks of treatment = significantly better 12-week healing outcomes
- Ulcers infected + ischaemic: 90× more likely to require amputation
- Presence of infected ulcer: 40-55% chance of some form of amputation
- Patient education reduces lower extremity amputation risk by 50-85%
- A 5-year survival of only 56% after first DFU - aggressive management is warranted
Key Sources
- Campbell's Operative Orthopaedics, 15th ed. 2026 - Chapter 91: Diabetic Foot (pp. 5054-5061): History, physical exam, Wagner/Brodsky classification, ABI, imaging, osteomyelitis
- Symptom to Diagnosis: An Evidence-Based Guide, 4th ed. (pp. 10495-10676): Disease highlights, risk factors, infection classification, osteomyelitis diagnostic LRs, microbiology
- Bailey and Love's Short Practice of Surgery, 28th ed. (p. 7443-7484): Diabetic foot infection, clinical presentation, MRI, probe-to-bone
- Schwartz's Principles of Surgery, 11th ed. - Chronic wounds chapter
- PMID 37302121 - IWGDF 2023 Guidelines on Prevention of Foot Ulcers in Diabetes (Practice Guideline + Systematic Review)
This is a shared conversation. Sign in to Orris to start your own chat.