Describe the types, clinical features and management of a new-born baby with tracheo- esophageal fistula. [2+3+5]
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from the textbooks. Let me compile the full answer.
Tracheo-Esophageal Fistula (TEF) in the Newborn
1. Types (2 marks)
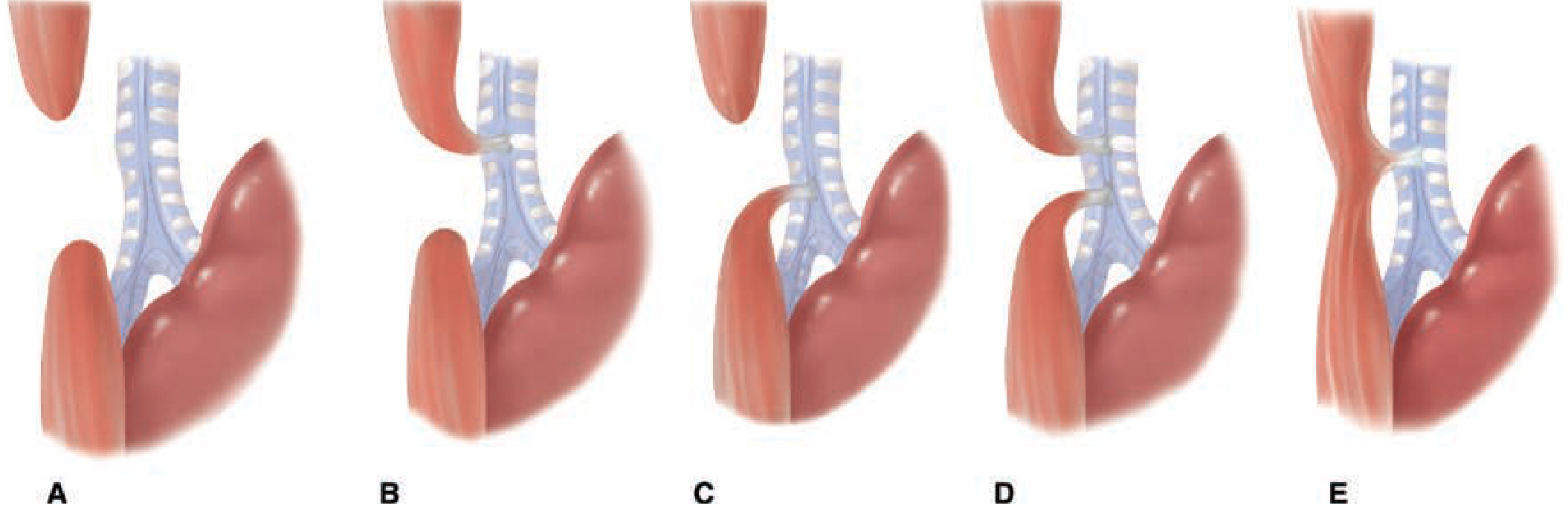
TEF occurs in approximately 1 in 1,500-3,000 live births, with a mild male predominance. In over 85% of cases, TEF is associated with esophageal atresia (EA). There are five anatomic types (Gross/Vogt classification):
| Type | Description | Incidence |
|---|---|---|
| A | Pure esophageal atresia (no fistula) - blind proximal pouch, blind distal pouch | 8-10% |
| B | EA + TEF between the proximal esophageal segment and trachea | ~1% |
| C (most common) | EA + TEF between distal esophagus and trachea (proximal blind pouch + distal fistula) | ~85% |
| D | EA + TEF between both proximal and distal esophageal segments and trachea | ~2% |
| E (H-type) | TEF without esophageal atresia - an oblique fistula resembling the letter "H" | ~8% |
- Type C (proximal EA + distal TEF) is by far the most prevalent; the proximal blind pouch typically ends roughly 1-2 vertebral body lengths above the carina, and the TEF inserts into the membranous trachea proximal to the carina.
- Type E (H-type) is the subtlest - presents later in infancy with recurrent chest infections.
(Schwartz's Principles of Surgery, 11e; Sabiston Textbook of Surgery)
2. Clinical Features (3 marks)
Prenatal Clues
- Polyhydramnios on antenatal ultrasound (failure of fetal swallowing in types with atresia means amniotic fluid cannot be absorbed)
- Failure to visualize the gastric bubble on ultrasound (pure EA)
Postnatal Presentation (at birth / first feeds)
- Excessive salivation / drooling - saliva accumulates in the proximal blind pouch and overflows
- Choking, coughing, and cyanosis immediately with first feed - milk/fluid aspirated through the blind pouch or fistula
- Abdominal distension - in type C/D, air passes from the trachea through the distal TEF into the stomach and bowel during crying/breathing; the abdomen becomes tympanic
- Respiratory distress - caused by:
- Aspiration of saliva/milk into the lungs
- Reflux of gastric contents through the TEF causing chemical pneumonitis
- Progressive atelectasis
- Inability to pass a nasogastric/orogastric tube into the stomach - the tube coils in the proximal blind pouch (this is a key diagnostic sign)
- H-type TEF (Type E) presents more subtly, often post-neonatally, with recurrent episodes of choking, coughing with feeds, recurrent aspiration pneumonia, and sometimes abdominal bloating
Diagnosis
- CXR: Shows the NG tube coiled in the upper esophageal pouch; air below the diaphragm confirms a distal TEF
- Plain radiograph: Dilated proximal pouch visible; absence of GI air suggests pure EA
- Contrast study: Oral contrast is contraindicated (aspiration risk); water-soluble contrast may delineate the upper pouch
- Bronchoscopy: Confirms TEF location, assesses for tracheomalacia
- Echocardiography + renal USS: Mandatory to identify associated anomalies (VACTERRL syndrome - vertebral, anorectal, cardiac, tracheo-esophageal, renal, radial limb defects)
Associated anomalies are present in 60-70% of cases: cardiac (38%), skeletal (19%), neurological (15%), renal (15%), anorectal (8%).
(Schwartz's Principles of Surgery, 11e; Sabiston Textbook of Surgery)
3. Management (5 marks)
A. Pre-operative (Initial Stabilization)
- Position: Nurse in an infant warmer with the head elevated at 30-45° (upright-prone) to reduce aspiration of saliva and gastric reflux
- Sump suction: Place a Replogle (double-lumen sump) catheter in the upper esophageal pouch on continuous low suction to keep it decompressed and dry
- IV access and fluids: Warmed electrolyte solution; avoid right upper extremity for IV (may interfere with surgical positioning)
- IV broad-spectrum antibiotics: Started immediately to treat/prevent aspiration pneumonia
- Ventilatory caution: Avoid endotracheal intubation and positive-pressure ventilation if possible - positive pressure preferentially drives air through the TEF into the GI tract, causing gastric distension and worsening ventilation. If ventilation is mandatory, place the ETT distal to the fistula or use an occlusive balloon catheter in the fistula
- Investigations: CXR, echocardiogram (anatomy of aortic arch and cardiac defects), renal USS, spinal X-rays
- Emergency gastrostomy: If severe respiratory compromise occurs due to gastric distension, an emergent gastrostomy (placed to water seal) can decompress the stomach and relieve the ventilatory burden
B. Timing of Surgery
- Definitive repair is rarely a surgical emergency
- If the neonate is hemodynamically stable and oxygenating well, repair is performed within 1-2 days of birth
- This window allows full assessment of coexisting anomalies and selection of an experienced team
- Premature neonates or those with severe associated anomalies may need staged repair
C. Definitive Surgical Repair (Type C - the commonest)
- Pre-operative bronchoscopy (optional by some surgeons): Defines fistula location and degree of tracheomalacia; Fogarty catheter placement aids dissection in recurrent cases
- Right extrapleural thoracotomy (standard approach): Right-sided unless a right-sided aortic arch is present
- Thoracoscopic repair: Increasingly preferred minimally invasive approach with comparable outcomes
- Steps:
- Divide the azygos vein to expose the fistula
- Ligate and divide the TEF close to the trachea; close the tracheal defect with absorbable interrupted sutures
- Mobilize the upper esophageal pouch maximally (good blood supply allows this; limit mobilization of the lower pouch due to its segmental vascular supply - to avoid ischemia)
- Perform a primary esophageal anastomosis (end-to-end, single or double layer, interrupted sutures)
- Post-op: Parenteral nutrition, chest drain, anastomotic leak check at ~5-7 days
D. Special Situations
- Pure EA (Type A) / Long-gap EA: Primary anastomosis not feasible in the neonatal period; gastrostomy for feeding is placed; esophageal lengthening techniques (e.g., Foker traction sutures, colon interposition, gastric pull-up) are used once the infant grows
- H-type TEF (Type E): Surgical division of the fistula via a right cervical approach (fistula is usually in the neck/upper thorax)
E. Prognosis
- Modern survival rates exceed 90% in full-term neonates without major cardiac defects
- The main determinants of mortality are associated cardiac anomalies and prematurity
- Long-term complications include anastomotic stricture (requiring dilatation), gastro-esophageal reflux, tracheomalacia, and recurrent TEF
(Schwartz's Principles of Surgery, 11e; Sabiston Textbook of Surgery, 21e; The Developing Human - Clinically Oriented Embryology)
Discuss various causes for vomiting in a newborn.
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have very comprehensive information from multiple authoritative textbooks. Let me compile the full answer.
Causes of Vomiting in a Newborn
Vomiting in a neonate is a common but important symptom. A key clinical distinction is whether the vomit is bilious (green) or non-bilious, as this localizes the level of the problem relative to the ampulla of Vater and determines urgency.
Bilious vomiting = abnormality distal to the ampulla of Vater - always a potential surgical emergency (1/3 to 1/2 will have a surgical lesion). Non-bilious vomiting = abnormality proximal to the ampulla of Vater - more often medical/feeding-related, but can still be surgical.
I. Surgical / Obstructive Causes
A. Non-Bilious Obstructions (above ampulla of Vater)
- Esophageal Atresia / TEF - blind proximal pouch; infant cannot swallow, drools, and chokes immediately at first feed; NG tube fails to pass into stomach
- Hypertrophic Pyloric Stenosis (HPS) - most common surgical cause of gastric outlet obstruction in infants; typically presents at 3-6 weeks of age with projectile, non-bilious vomiting after feeds; visible peristaltic waves; palpable "olive" mass in the right hypochondrium; causes hypochloraemic, hypokalaemic metabolic alkalosis
- Pyloric Atresia / Gastric Web - rare; congenital mucosal web or diaphragm at the pylorus or antrum; non-bilious vomiting from birth; large gastric bubble on X-ray; associated with epidermolysis bullosa
- Pre-ampullary Duodenal Obstruction - duodenal web or atresia proximal to ampulla of Vater (rare minority, ~20%); non-bilious vomiting
- Enteric Duplication Cysts (gastric) - rare; located near the antrum/pylorus; cause gastric outlet obstruction with non-bilious vomiting and a palpable mass; confirmed by USS showing characteristic "gut signature" wall
B. Bilious Obstructions (below ampulla of Vater)
- Malrotation with Midgut Volvulus - the most dangerous cause; presents in the first few days-weeks of life with sudden onset bilious vomiting, abdominal pain, rapid deterioration; midgut twists around the superior mesenteric artery pedicle causing ischaemic necrosis; classic "corkscrew" on upper GI contrast study; requires emergency Ladd's procedure
- Duodenal Atresia - failure of recanalization during 5th-6th week of gestation; 80% occur distal to ampulla (bilious vomiting); classic "double-bubble" sign on X-ray (dilated stomach + first part duodenum, no distal gas); associated with Down syndrome (30%), cardiac defects, malrotation, VACTERL
- Jejuno-Ileal Atresia - intrauterine vascular accident; bilious vomiting, abdominal distension; multiple dilated loops on X-ray; "triple-bubble" or ladder-pattern
- Meconium Ileus - inspissated meconium obstructs the terminal ileum; almost always associated with cystic fibrosis; bilious vomiting, abdominal distension, failure to pass meconium; "soap bubble" appearance (Neuhauser sign) on X-ray; may be complicated by perforation, peritonitis, or volvulus
- Hirschsprung's Disease (congenital aganglionic megacolon) - absence of ganglion cells in the distal bowel (most often rectosigmoid); bilious vomiting, abdominal distension, failure to pass meconium >48 hours; rectal examination may release explosive stool and gas (decompression sign); confirmed by rectal biopsy
- Anorectal Malformations / Imperforate Anus - visible on inspection of perineum; causes low obstruction with bilious vomiting and abdominal distension
- Annular Pancreas - ring of pancreatic tissue encircling the duodenum; causes extrinsic duodenal obstruction; bilious or non-bilious depending on level; associated with Down syndrome and duodenal atresia
- Ladd's Bands - peritoneal bands from malrotation crossing the duodenum; cause partial or complete duodenal obstruction with bilious vomiting
- Incarcerated Inguinal Hernia - bowel incarcerated in the hernia sac; bilious vomiting, irreducible groin swelling; more common in premature males
II. Non-Surgical / Medical Causes
C. Physiological / Feeding-Related (most common overall)
- Gastroesophageal Reflux (GER) - passive effortless regurgitation of feeds; non-bilious; very common; the neonate is otherwise well and gaining weight; lower oesophageal sphincter immaturity; distinguished from true vomiting (no forceful expulsion)
- Overfeeding - excessive feed volume; regurgitation/spitting up after feeds; resolves with feed volume reduction
- Incorrect feeding technique - poor latch, swallowing of air (aerophagia)
- Cow's Milk Protein Allergy / Intolerance - may cause vomiting with loose stools, blood in stool, and eczema
D. Infectious Causes
- Neonatal Sepsis - vomiting is one of many non-specific signs; may be accompanied by temperature instability, lethargy, poor feeding, bulging fontanelle
- Meningitis - raised intracranial pressure causes vomiting; tense/bulging fontanelle, seizures, irritability
- Gastroenteritis - viral (rotavirus, adenovirus) or bacterial; vomiting with diarrhoea
- Urinary Tract Infection (UTI) - vomiting with fever, poor feeding; urine culture confirms diagnosis
- TORCH infections (congenital) - systemic illness with vomiting as part of broader clinical picture
E. Metabolic / Endocrine Causes
- Inborn Errors of Metabolism (IEM) - urea cycle defects, organic acidaemias (propionic, methylmalonic acid), amino acidopathies (maple syrup urine disease); vomiting often begins after first feeds (protein intake); accompanied by lethargy, encephalopathy, abnormal odour
- Congenital Adrenal Hyperplasia (CAH) - salt-wasting form (21-hydroxylase deficiency); vomiting, hyponatraemia, hyperkalaemia, shock; females may be virilised
- Galactosaemia - vomiting, jaundice, and liver disease after starting milk feeds; cataracts, E. coli sepsis
F. Neurological Causes
- Intracranial Haemorrhage - birth trauma (subdural, subarachnoid bleeds); raised ICP; vomiting, bulging fontanelle, seizures, altered tone
- Hydrocephalus - raised ICP causes vomiting with head circumference enlargement
- Cerebral Oedema - post-asphyxia or metabolic encephalopathy; vomiting as part of ICP rise
- Kernicterus - bilirubin encephalopathy; vomiting is an early feature before frank neurological signs
G. Renal Causes
- Obstructive Uropathy - hydronephrosis, pelvi-ureteric junction obstruction; may present with vomiting, palpable renal mass, poor urinary stream
- Renal Insufficiency - any cause; uraemia leads to vomiting
H. Miscellaneous
- Necrotising Enterocolitis (NEC) - primarily in premature neonates; ischaemic injury to the gut wall; bilious vomiting, abdominal distension, bloody stools, pneumatosis intestinalis on X-ray
- Adrenal Insufficiency - cortisol/aldosterone deficiency; vomiting with hypoglycaemia, hyponatraemia, hyperkalaemia
- Drug effects - maternal opioids, erythromycin (a motilin agonist in neonates); iatrogenic
- Ileus - secondary to sepsis, electrolyte imbalance, or post-operative states; functional obstruction
Summary Table
| Category | Key Diagnoses | Vomit Character |
|---|---|---|
| Gastric outflow obstruction | Pyloric stenosis, pyloric atresia, gastric web | Non-bilious, projectile |
| Upper GI anomaly | EA/TEF, duodenal atresia (pre-ampullary) | Non-bilious |
| Small bowel obstruction | Malrotation/volvulus, duodenal atresia, jejunoileal atresia | Bilious |
| Large bowel obstruction | Hirschsprung's, meconium ileus, imperforate anus | Bilious + abdominal distension |
| Physiological | GER, overfeeding | Non-bilious, effortless |
| Infectious | Sepsis, meningitis, UTI | Variable |
| Metabolic | IEM, CAH, galactosaemia | Non-bilious, after feeds |
| Neurological | ICH, hydrocephalus | Non-bilious, with raised ICP signs |
| Surgical emergency | Malrotation + volvulus, NEC, incarcerated hernia | Bilious, systemic compromise |
(Tintinalli's Emergency Medicine; Grainger & Allison's Diagnostic Radiology; Fischer's Mastery of Surgery, 8e; Schwartz's Principles of Surgery, 11e)
This is a shared conversation. Sign in to Orris to start your own chat.