Pulmonary hypertension
Reading File
Finding Sources
Searching PubMed
"pulmonary hypertension"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Finding Sources
Searching PubMed
"pulmonary hypertension"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Finding Sources
Searching PubMed
"pulmonary arterial hypertension"[MeSH Terms] AND "drug therapy"[MeSH Terms]
Reading File
Finding Sources
Reading Article
PMID: 40167274
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I have all the material needed for a comprehensive answer. Let me now compose it.
Pulmonary Hypertension
Definition
Pulmonary hypertension (PH) is a syndrome of elevated pulmonary pressures leading to increased right ventricular (RV) afterload, which can progress to RV failure and death. Per the 6th World Symposium on Pulmonary Hypertension (WSPH), PH is now defined as a mean pulmonary artery pressure (mPAP) > 20 mm Hg measured by right heart catheterization (RHC) - revised down from the prior threshold of 25 mm Hg. Normal mPAP is 14 ± 3.3 mm Hg.
- Murray & Nadel's Textbook of Respiratory Medicine
WHO Classification (6th WSPH)
There are 5 clinical groups, each with distinct mechanisms and treatments:
| Group | Category | Mechanism | Examples |
|---|---|---|---|
| 1 | Pulmonary Arterial Hypertension (PAH) | Pulmonary vascular remodeling | Idiopathic (~50%), CTD (~25%), heritable (BMPR2), drug/toxin-induced, HIV, portal HTN, CHD |
| 2 | PH due to Left Heart Disease | Elevated PCWP (postcapillary) | HFrEF, HFpEF, valvular disease |
| 3 | PH due to Lung Disease/Hypoxia | Hypoxic vasoconstriction, loss of vascular bed | COPD, IPF, sleep apnea |
| 4 | Chronic Thromboembolic PH (CTEPH) | Mechanical obstruction + remodeling | 2-3% of PE survivors; ~1/3 have no known PE history |
| 5 | PH with unclear/multifactorial mechanisms | Mixed | Sarcoidosis, hemolytic anemia, metabolic disorders |
Hemodynamic subtypes (Table 83.1):
| Type | mPAP | PCWP | PVR | Groups |
|---|---|---|---|---|
| Precapillary PH | >20 mmHg | ≤15 mmHg | ≥3 WU | 1, 3, 4, 5 |
| Isolated postcapillary PH | >20 mmHg | >15 mmHg | <3 WU | 2, 5 |
| Combined pre+postcapillary PH | >20 mmHg | >15 mmHg | ≥3 WU | 2, 5 |
- Murray & Nadel's Textbook of Respiratory Medicine
Pathobiology (Group 1 PAH)
The PAH vasculopathy predominantly affects small pulmonary arterioles and is characterized by:
- Intimal hyperplasia
- Medial hypertrophy
- Adventitial proliferation and metalloprotease activation
- In situ thrombosis
- Plexiform lesions (pathognomonic)
- Inflammation
Genetic basis: The best-characterized defect is mutation in BMPR2 (bone morphogenetic protein receptor type 2), a member of the TGF-β signaling family. Less common mutations involve ALK-1, endoglin (associated with hereditary hemorrhagic telangiectasia), CAV1, SMAD9, and KCNK3 (a channelopathy representing TGF-β-independent disease).
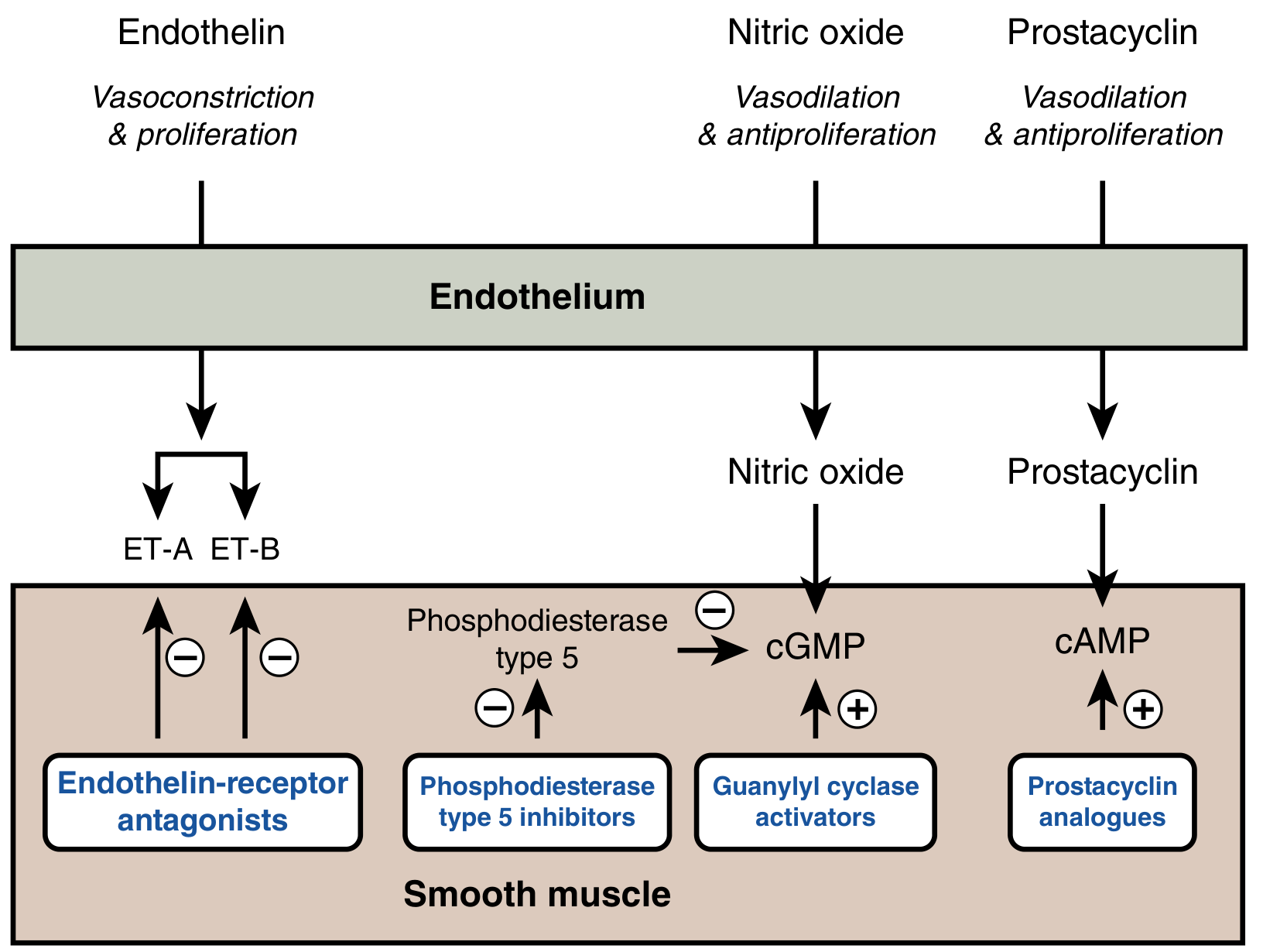
Vasoactive mediator imbalance:
| Mediator | Change in PAH | Effect |
|---|---|---|
| Prostacyclin | ↓ (reduced synthase) | Loss of vasodilation + antiproliferation |
| Nitric oxide | ↓ (reduced NOS) | Loss of vasodilation; ↓ cGMP |
| PDE-5 | ↑ (upregulated) | Further ↓ cGMP |
| Endothelin-1 | ↑ | Vasoconstriction + smooth muscle proliferation |
| Thromboxane | ↑ | Vasoconstriction + platelet aggregation |
The "multiple-hit hypothesis" proposes that PAH develops from the interaction of a predisposing state (e.g., BMPR2 mutation) plus one or more inciting stimuli.
- Goldman-Cecil Medicine
Clinical Features
Symptoms (insidious onset, often delayed diagnosis by 2-3 years):
- Dyspnea on exertion (most common presenting complaint)
- Fatigue
- Exercise intolerance
- Syncope or pre-syncope (indicates severely reduced cardiac output)
- Chest pain (RV ischemia)
- Peripheral edema, ascites (right heart failure)
Signs:
- Loud P2 (pulmonic component of S2)
- Right-sided S3 or S4
- Tricuspid regurgitation murmur (systolic, increases with inspiration)
- Elevated JVP, hepatomegaly, ascites, peripheral edema
- Left parasternal heave (RV hypertrophy)
- Central cyanosis
Diagnosis
Diagnosis requires a systematic stepwise approach:
Step 1: Initial Workup
- NT-proBNP / BNP - elevated in PH; normal does not exclude
- ECG - right axis deviation, RV hypertrophy, right atrial enlargement, anterior ST/T changes (RV strain)
- Chest X-ray - enlarged proximal PAs with peripheral pruning; increased retrosternal space loss on lateral (RV enlargement)
Step 2: Echocardiography (screening cornerstone)
- Estimates RV systolic pressure via tricuspid regurgitation jet velocity (modified Bernoulli equation)
- Identifies: RA and RV enlargement, flattened interventricular septum ("D-sign"), underfilled LV
- Evaluates left-sided causes of PH (systolic/diastolic dysfunction, valvular disease, CHD)
- Note: Echo is prone to error especially in parenchymal lung disease
Step 3: Exclude CTEPH
- V/Q scan is the study of choice - shows mismatched perfusion defects
- CT pulmonary angiogram - good for acute PE but can miss chronic disease
- Pulmonary angiography if V/Q or CTPA shows abnormality
Step 4: Further workup
- Pulmonary function tests - mild restrictive/obstructive pattern, reduced DLCO in PAH; identifies significant lung disease (Group 3)
- Polysomnography - excludes sleep apnea (Group 3)
- Serology: ANA, anti-Scl-70, anti-centromere (CTD screening); HIV; liver function tests; hepatitis screen
- 6-minute walk test (6MWT) - functional capacity, baseline, prognosis
- CT chest - lung parenchyma, mediastinum
Step 5: Right Heart Catheterization (mandatory for definitive diagnosis)
-
Only tool providing definitive hemodynamic diagnosis
-
Measures: mPAP, PCWP, PVR, cardiac output
-
Acute vasodilator testing (with inhaled nitric oxide, adenosine, or IV epoprostenol) in Group 1 PAH:
- Positive response: mPAP falls ≥10 mmHg to <40 mmHg with stable/increased CO
- ~7% of idiopathic PAH are responders - these may benefit from calcium channel blockers
-
Goldman-Cecil Medicine; Murray & Nadel's Textbook of Respiratory Medicine
Drug and Toxin Causes of PAH (Group 1)
Definite risk: Aminorex, fenfluramine, dexfenfluramine, benflurex, methamphetamines, dasatinib, toxic rapeseed oil
Possible risk: Cocaine, amphetamines, interferon-α/β, alkylating agents, SSRIs (neonatal), bosutinib, direct-acting antivirals
- Murray & Nadel's Textbook of Respiratory Medicine
Treatment
General Measures (All PH Groups)
- Refer to a specialized PH center
- Supplemental O2 if SpO2 < 90% (goal >90% at rest and >90% with exercise)
- Low-level graded aerobic exercise; specialized pulmonary rehabilitation
- Avoid high altitude and strenuous activity
- Sodium restriction (<2400 mg/day); fluid restriction if RV failure present
- Vaccinations: influenza, pneumococcal, COVID-19
- Pregnancy avoidance - hemodynamic changes are potentially life-threatening; mortality historically 30-50%
- Diuretics (furosemide ± spironolactone) for RV volume overload - monitor electrolytes/renal function
- Anticoagulation: NOT routinely recommended unless other indications exist
Group 1 PAH: Targeted Therapies
The therapeutic targets reflect the three key abnormal endothelial mediator pathways:
1. Calcium Channel Blockers (CCBs)
- Reserved for acute vasoreactor responders only (~7% of idiopathic PAH)
- Agents: long-acting nifedipine (90-180 mg/day), diltiazem (360-720 mg/day), amlodipine (10-20 mg/day)
- Avoid verapamil (negative inotropic effects)
- Must closely monitor for safety and efficacy; if not achieving FC I-II, add targeted therapy
2. Endothelin Receptor Antagonists (ERAs)
- Block ET-A and/or ET-B receptors, reducing vasoconstriction and smooth muscle proliferation
- Bosentan (dual ERA): 62.5 mg BID → up to 125 mg BID; requires monthly LFTs (hepatotoxic); increases OCP metabolism
- Ambrisentan (selective ET-A): lower liver toxicity rate
- Macitentan: once-daily; longest duration of action
- Class precaution: All ERAs are teratogenic - require monthly pregnancy testing + 2 reliable contraception methods
3. PDE-5 Inhibitors
- Inhibit cGMP-specific phosphodiesterase type 5, enhancing NO-cGMP signaling → vasodilation + antiproliferation
- Sildenafil (Revatio): 20 mg TID (pivotal SUPER-1 trial)
- Tadalafil: once-daily dosing
- Generally well tolerated; avoid in combination with nitrates
4. Soluble Guanylate Cyclase (sGC) Stimulators
- Riociguat: stimulates sGC directly and sensitizes it to endogenous NO, ↑ cGMP
- Also approved for CTEPH (group 4)
5. Prostacyclin Pathway Agents
- Replaces deficient prostacyclin, promoting vasodilation + antiproliferation via cAMP
- Epoprostenol (IV): most potent; first-line for FC IV and highest-risk patients; very short half-life (requires continuous IV infusion)
- Treprostinil: SC, IV, inhaled, or oral; longer stability
- Iloprost: inhaled prostacyclin
- Selexipag: oral selective IP receptor agonist
6. Targeting the BMP Pathway (Novel)
- Sotatercept: a fusion protein (activin receptor type IIA - Fc fusion) that corrects TGF-β/BMP pathway imbalance
- Dose: 0.3 mg/kg SC every 3 weeks, escalated to 0.7 mg/kg
- Reduces PVR, improves 6MWT, lowers NT-proBNP
Treatment Algorithm
Risk stratification is central to treatment decisions. Low-risk profile targets: 6MWT >440 m, WHO FC I/II, normal/near-normal NT-proBNP.
- Non-vasoreactors without comorbidities: Initial dual combination therapy (ERA + PDE5i) is standard of care
- Non-vasoreactors with cardiopulmonary comorbidities: Initial oral monotherapy (PDE5i preferred)
- High-risk (FC III/IV): Triple therapy including IV/SC prostacyclin analogue
- Vasoreactors: CCB trial; escalate if no improvement to FC I/II
Invasive Therapies
- Pulmonary endarterectomy (PEA): Potentially curative surgical treatment for operable CTEPH (Group 4)
- Balloon pulmonary angioplasty (BPA): For inoperable CTEPH
- Atrial septostomy: Creates R-to-L interatrial shunt to decompress RV; reserved for refractory cases at specialized centers (significant morbidity/mortality)
- Bilateral lung or heart-lung transplantation: For patients with FC III/IV refractory to optimized therapy including prostanoids; referral at time of diagnosis in selected patients
Group 2 (PH due to LHD)
- No approved PAH-specific therapy
- Focus on treating underlying heart failure (reduce pulmonary venous pressure)
- PAH-targeted drugs are NOT indicated and may be harmful
Group 3 (PH due to Lung Disease)
- Treat underlying lung disease; supplemental oxygen
- PAH therapies generally reserved for patients with pre-capillary component (PVR ≥3 WU)
Group 4 (CTEPH)
- Anticoagulation (lifelong)
- Surgical PEA is first-line for accessible disease
- Riociguat for inoperable or persistent/recurrent CTEPH
- BPA for non-surgical candidates
Prognosis and Risk Stratification
Poor prognostic factors:
- WHO Functional Class III or IV
- Low 6MWT distance (<165 m = very high risk)
- Elevated NT-proBNP/BNP
- RV dysfunction on imaging (TAPSE <1.8 cm, pericardial effusion)
- Low cardiac index, high PVR
- Syncope
Recent Evidence (2024-2025)
Sotatercept has emerged as a major therapeutic advance:
-
STELLAR trial (FC II/III PAH): Sotatercept added to background therapy improved 6MWT, PVR, and time to clinical worsening vs. placebo.
-
ZENITH trial (PMID: 40167274) - NEJM, 2025: Among high-risk PAH patients (FC III/IV, REVEAL Lite 2 score ≥9) on maximum background therapy, sotatercept reduced the composite of death, lung transplantation, or hospitalization by 76% (HR 0.24, 95% CI 0.13-0.43; P<0.001). The trial was stopped early for efficacy. Death occurred in 8.1% vs. 15.1% (sotatercept vs. placebo).
-
PHOENIX trial (PMID: 41025556) - NEJM, 2025: Sotatercept within the first year after PAH diagnosis showed significant benefit.
-
Macitentan + tadalafil initial combination (PMID: 38966990) - Eur J Heart Fail, 2024: Initial combination therapy effective even with cardiac comorbidities.
These trials confirm sotatercept as a third therapeutic pillar targeting the BMP/activin pathway, distinct from the classical endothelin, NO, and prostacyclin pathways.
Sources: Murray & Nadel's Textbook of Respiratory Medicine | Goldman-Cecil Medicine | Braunwald's Heart Disease | Humbert et al., NEJM 2025 (PMID 40167274) | McLaughlin et al., NEJM 2025 (PMID 41025556)
This is a shared conversation. Sign in to Orris to start your own chat.