Eales disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
Eales disease retinal vasculitis
Reading File
Reading File
Searching Images
Eales disease peripheral retinal periphlebitis neovascularization fundus
Reading File
I now have comprehensive information. Let me compile the full answer.
Eales Disease
Overview
Eales disease is an idiopathic occlusive peripheral periphlebitis (inflammation and obliteration of peripheral retinal veins). It is rare in White populations but is a significant cause of visual morbidity among young South Asian males (typically 20–40 years of age). It is bilateral in most cases, though often asymmetrical, and is considered a diagnosis of exclusion after other causes of retinal vasculitis are ruled out.
— Kanski's Clinical Ophthalmology, 10th ed.
Aetiology
- Idiopathic — the exact cause remains unknown.
- Tubercular protein hypersensitivity is the most widely proposed mechanism: Mycobacterium tuberculosis antigens are thought to trigger a delayed-type hypersensitivity reaction in the peripheral retinal vessels, even in the absence of active systemic TB. PCR for TB DNA has been detected in vitreous specimens of some patients.
- Oxidative stress and immunological dysregulation may play additional roles.
- Evidence for TB association is conflicting; some patients are classified as having true tubercular vasculitis, while others have truly idiopathic disease.
Pathology & Stages
The disease passes through three overlapping stages:
| Stage | Features |
|---|---|
| 1 — Inflammatory | Perivenous sheathing (periphlebitis), superficial retinal haemorrhages, cotton-wool spots, mild anterior uveitis |
| 2 — Occlusive | Branch retinal vein occlusion; peripheral capillary non-perfusion; microaneurysms, vascular tortuosity, shunts |
| 3 — Neovascular | Retinal neovascularization (NVE/NVD) at the junction of perfused and non-perfused retina; recurrent vitreous haemorrhage (in ~1/3 of eyes) |
Clinical Features
Symptoms
- Floaters or sudden, painless visual loss due to vitreous haemorrhage
- Neurological features (myelopathy, hemiplegia) have been reported rarely — Eales disease appears under spinal cord disorders in some neurology texts
Fundus Findings
- Peripheral periphlebitis: vascular sheathing, perivascular exudates
- Peripheral capillary non-perfusion: leads to neovascularization at the ischaemic border
- Vitreous haemorrhage: often recurrent and usually self-limited, absorbing over weeks
- Macular involvement: uncommon but possible
Complications
- Tractional retinal detachment
- Macular epiretinal membrane
- Neovascular glaucoma
- Cataract
Investigations
- Fluorescein angiography (FA): key investigation — identifies periphlebitis, areas of capillary non-perfusion, and neovascularization; wide-field imaging is especially valuable
- OCT: assess macular pathology
- Investigations to exclude other causes: chest X-ray, Mantoux/PPD, QuantiFERON-TB Gold, ACE level (sarcoidosis), FBC with haemoglobin electrophoresis (haemoglobinopathies), VDRL/TPHA (syphilis), ANA/ANCA
Fundus Images
Clinical appearance (Kanski's, Fig. 13.59):
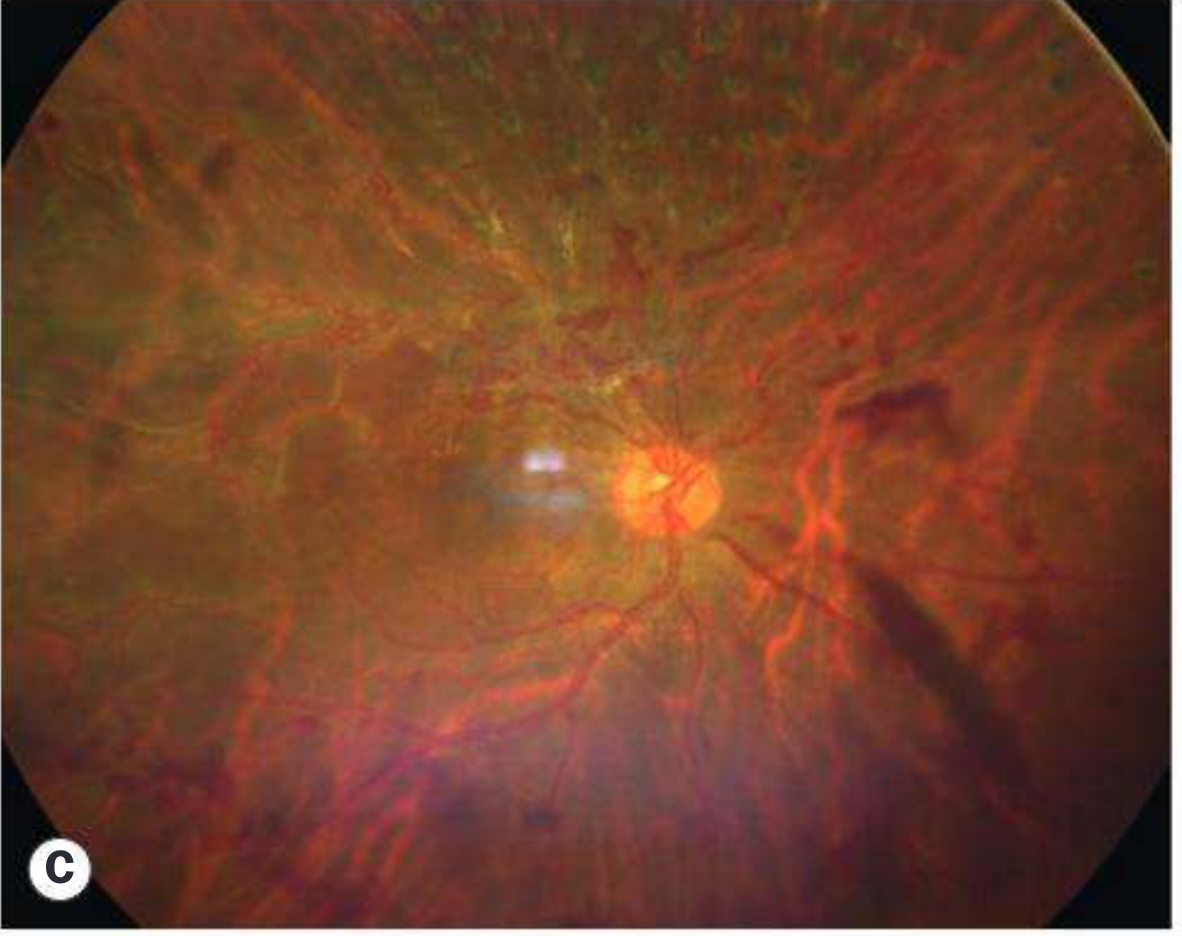

From the literature:


Treatment
Inflammatory Stage
- Topical, periocular, systemic, or intravitreal corticosteroids to suppress active vasculitis
- Antitubercular therapy (ATT): controversial but advocated by many (especially in South Asian populations); recommended when QuantiFERON/Mantoux is strongly positive, or active TB is suspected; ATT with steroids reduces recurrence risk
Occlusive/Neovascular Stage
- Scatter (sectoral) photocoagulation or cryotherapy to non-perfused peripheral retina — reduces neovascular stimulus (analogous to treatment of diabetic retinopathy)
- Intravitreal anti-VEGF (bevacizumab, ranibizumab): widely used for active neovascularization
Surgical Stage
- Pars plana vitrectomy: for persistent non-clearing vitreous haemorrhage, tractional retinal detachment, or macular epiretinal membrane
Prognosis
- Generally good for central vision if macular involvement is absent and treatment is prompt
- Recurrent vitreous haemorrhages are the main cause of morbidity; most clear spontaneously
- Late complications (tractional detachment, neovascular glaucoma) carry a worse prognosis
Key Differentials
| Condition | Distinguishing Feature |
|---|---|
| Sarcoidosis | Hilar lymphadenopathy, elevated ACE, "candle wax drippings" |
| Tuberculosis (ocular) | Active systemic TB, choroidal granulomas |
| Sickle cell retinopathy | Haemoglobin electrophoresis abnormal, "sea-fan" NVE |
| Pars planitis | Snowball/snowbank vitreous opacities, younger patients |
| Behçet disease | Oral/genital ulcers, arteriolar as well as venous involvement |
— Kanski's Clinical Ophthalmology 10th ed.; Wills Eye Manual
Recent evidence note: Two 2026 systematic reviews from the International Uveitis Study Group (IUSG ReViSe study) address work-up and treatment in retinal vasculitis broadly, including Eales disease [PMID 40972796, PMID 40983164]. These may update protocols for investigation and immunosuppressive management.
This is a shared conversation. Sign in to Orris to start your own chat.