Thymus gland with pics
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I have all the content and images I need. Let me now compile the comprehensive answer.
Thymus Gland
The thymus is a primary (central) lymphoid organ - the site where T lymphocytes develop, mature, and become immunocompetent. It is one of the most important organs in immunology, yet one of the least appreciated because it involutes after puberty.
1. Location & Gross Anatomy
The thymus sits in the superior mediastinum, immediately posterior to the manubrium of the sternum, anterior to the heart and great vessels. Its upper pole can extend into the neck as high as the thyroid gland; its lower portion extends into the anterior mediastinum over the pericardial sac.
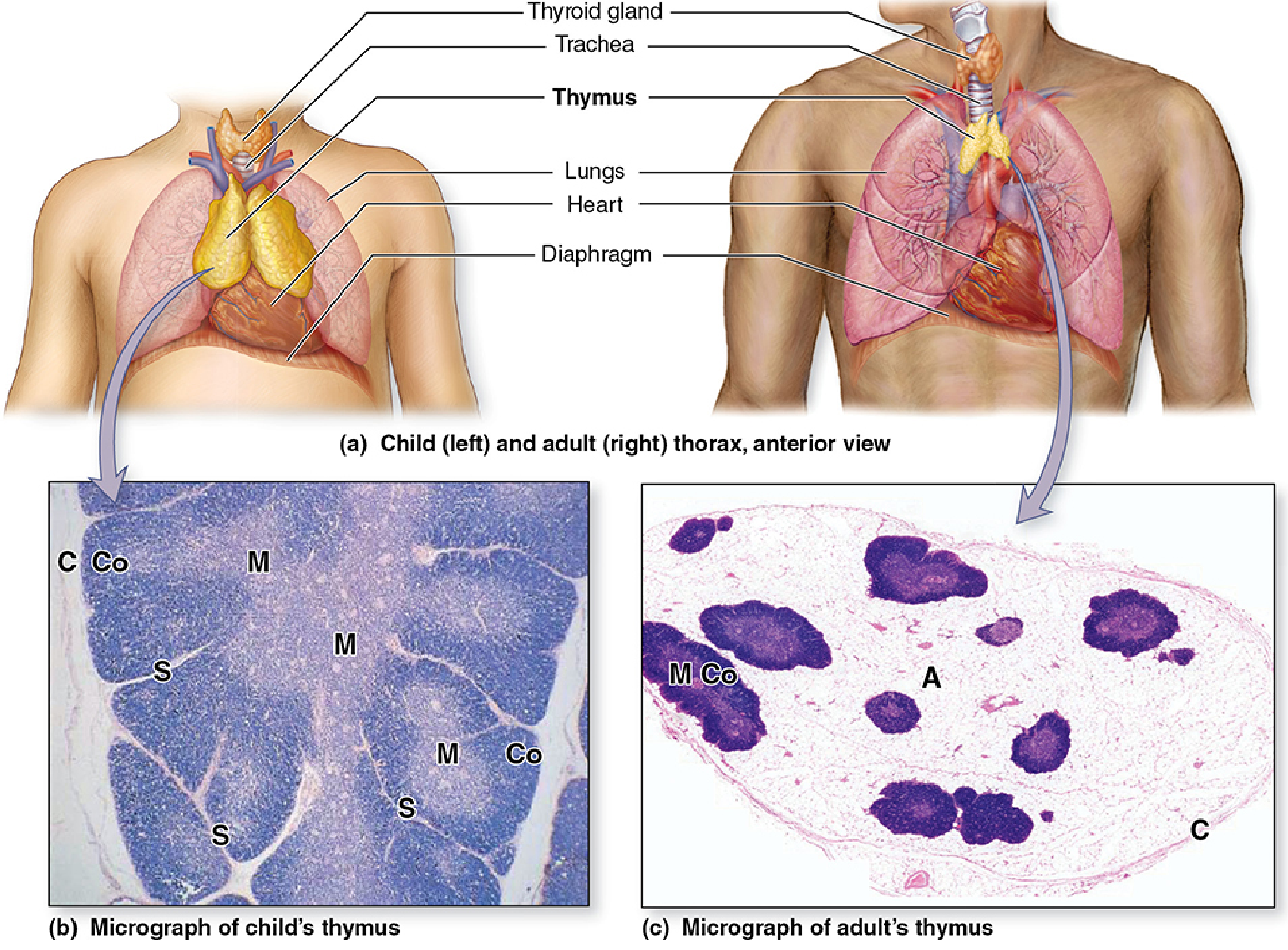
The bilobed thymus in a child (left) is large and prominent between the lungs anterior to the heart. After puberty (right), it involutes and is replaced by adipose tissue.
Key gross features:
- Bilobed structure - two asymmetric, fused lobes enclosed by a thin fibrous capsule
- Fibrous septa/trabeculae from the capsule divide each lobe into incompletely separated lobules
- At birth: weighs 10-35 g; grows to 20-50 g at puberty (its maximum), then involutes to 5-15 g in older adults
- Can involute early (in children/young adults) with severe illness or HIV infection
Blood supply: Small branches of the internal thoracic arteries
Venous drainage: Left brachiocephalic vein and internal thoracic veins
Lymphatic drainage: To parasternal nodes, tracheobronchial nodes, and root of neck nodes
(Gray's Anatomy for Students, p. 252; Robbins, Cotran & Kumar, p. 591)
2. Histology - General Architecture
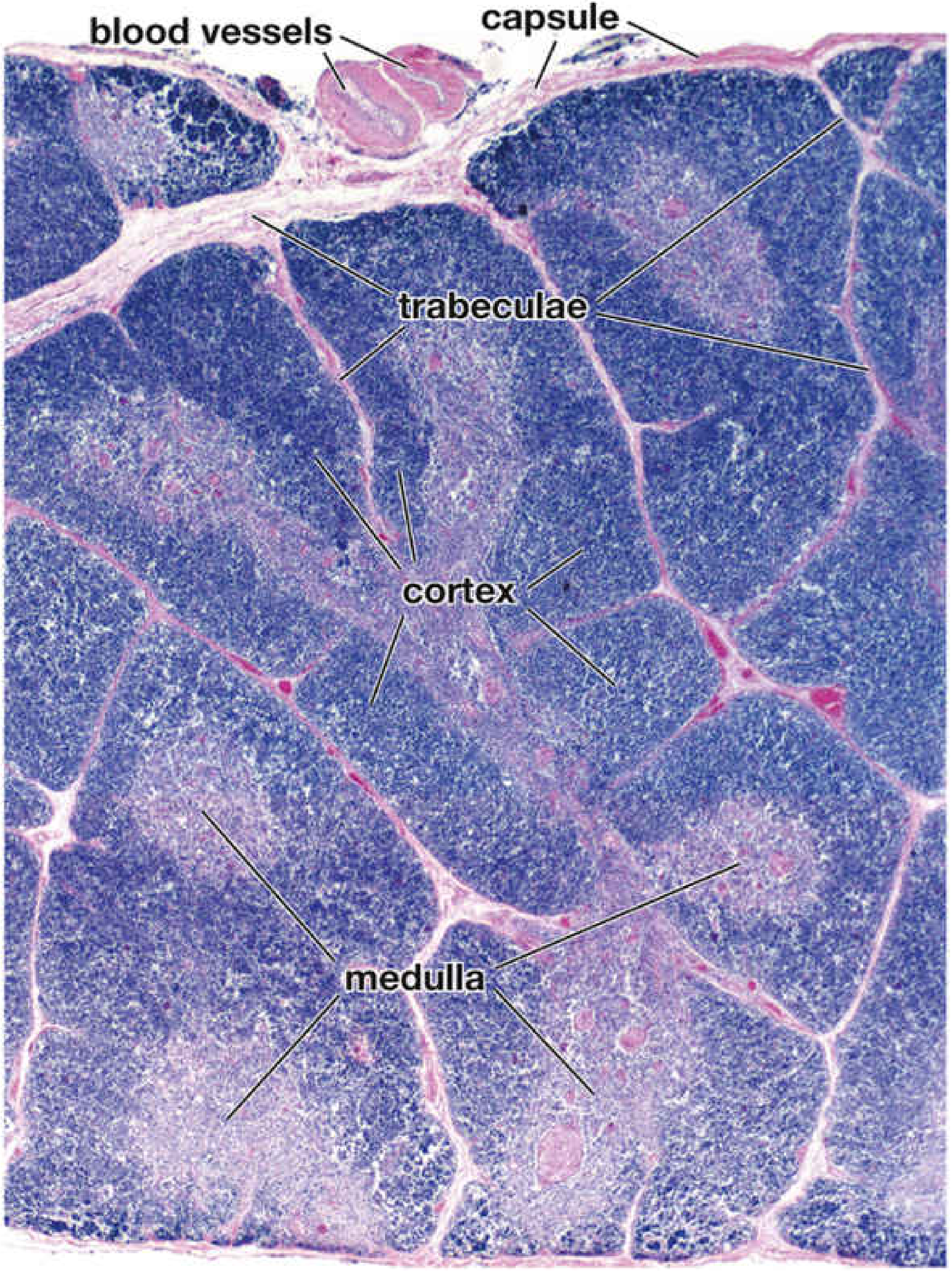
Low-power H&E: The capsule sends trabeculae inward, creating lobules. Each lobule has a dark outer cortex (densely packed lymphocytes) and a paler inner medulla (fewer lymphocytes, more epithelioreticular cells). The medulla is actually a single continuous branching mass, not truly separate islands.
Each lobule has two distinct zones:
| Feature | Cortex | Medulla |
|---|---|---|
| Staining | Dark (basophilic) | Pale (eosinophilic) |
| Cells | Densely packed thymocytes + macrophages | Loosely packed T cells + epithelioreticular cells |
| Characteristic structure | Blood-thymus barrier | Hassall (thymic) corpuscles |
| Function | T-cell proliferation + positive selection | Negative selection + export |
(Histology: A Text and Atlas, p. 1227-1229)
3. Cells of the Thymus
Thymocytes (developing T cells)
Common lymphoid progenitors from the bone marrow enter the thymus and proliferate massively in the cortex. They are called thymocytes during their development. Approximately 98% die by apoptosis within the thymus (phagocytosed by cortical macrophages) because they fail the selection tests.
Epithelioreticular Cells (TECs) - The Key Stromal Cells
Unlike other lymphoid organs (which have reticular cells + reticular fibers as stroma), the thymus uses epithelioreticular cells as its scaffold. These cells have features of both epithelium (desmosomes, intermediate filaments) and reticular cells (stellate shape, cytoplasmic processes). There are 6 types classified by location and function:
In the Cortex:
| Type | Location | Function |
|---|---|---|
| Type I | Capsule/trabecula/perivascular boundary | Forms part of blood-thymus barrier; separates parenchyma from CT |
| Type II | Cortical interior | Compartmentalizes cortex; expresses MHC I and MHC II |
| Type III | Corticomedullary junction | Barrier between cortex and medulla; expresses MHC I and II |
In the Medulla:
| Type | Location | Function |
|---|---|---|
| Type IV | Near corticomedullary junction | Cooperates with type III to form junction barrier |
| Type V | Throughout medulla | Framework of medulla (analogous to type II in cortex) |
| Type VI | Medulla | Forms Hassall corpuscles |
(Histology: A Text and Atlas, p. 1230-1232)
4. The Blood-Thymus Barrier
A critical feature unique to the thymic cortex is the blood-thymus barrier, which prevents circulating antigens from entering the cortex and activating immature (not yet educated) thymocytes prematurely.
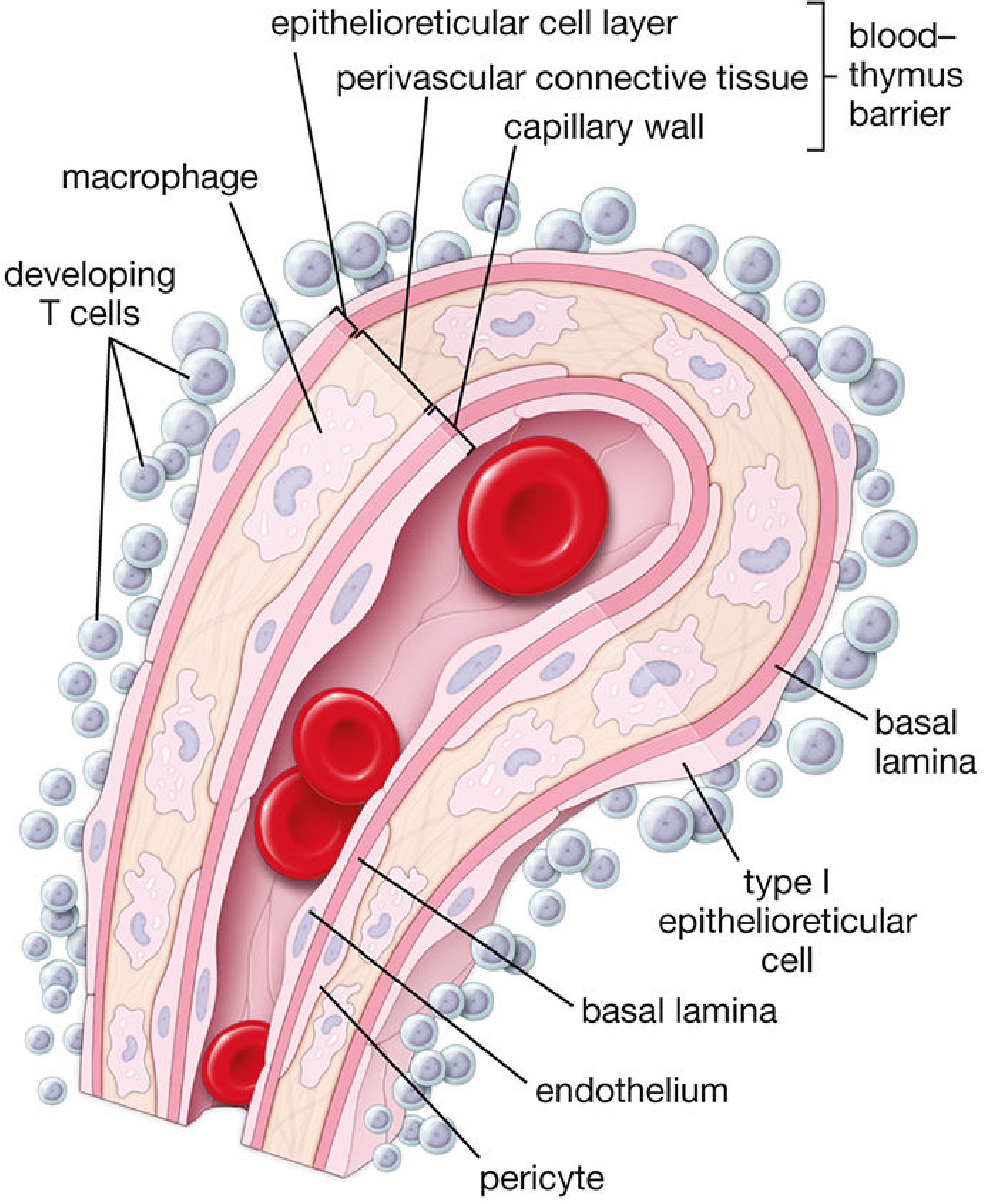
The blood-thymus barrier, from lumen outward:
- Continuous capillary endothelium with tight junctions (most impermeable layer)
- Endothelial basal lamina + pericytes
- Perivascular connective tissue space with macrophages (phagocytose any antigen that leaks through)
- Type I epithelioreticular cells with occluding junctions + their basal lamina
Note: The medulla does NOT have a blood-thymus barrier - antigen CAN enter the medulla, which is actually needed for negative selection.
(Histology: A Text and Atlas, p. 1235)
5. Hassall (Thymic) Corpuscles
The pathognomonic histologic feature of the thymus. Found only in the medulla.
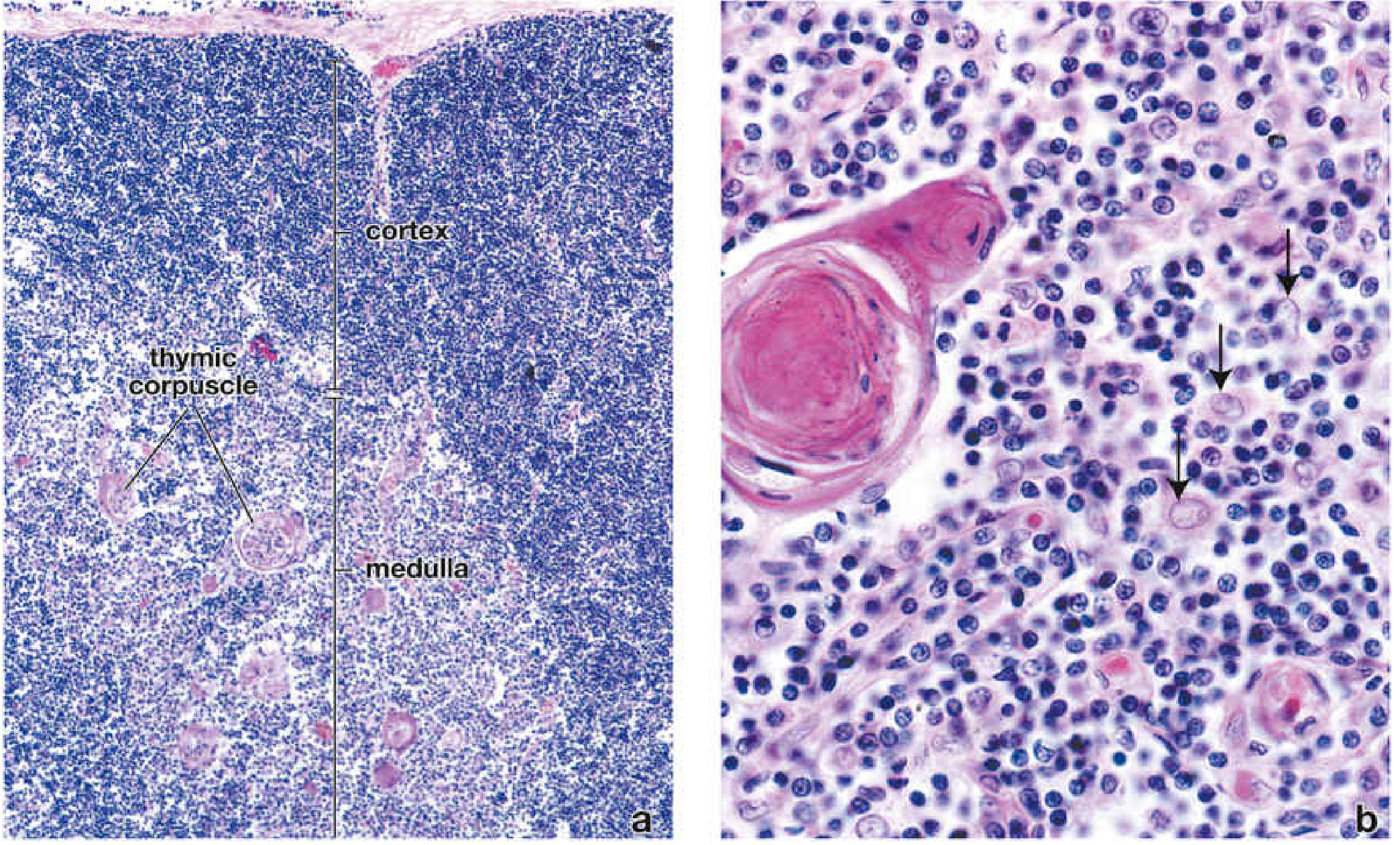
(a) Low power: cortex is densely cellular (dark blue), medulla is lighter with eosinophilic whorls = Hassall corpuscles
(b) High power: a single Hassall corpuscle with concentrically arranged type VI epithelioreticular cells (flattened nuclei), fully keratinized center. Arrows indicate type V epithelioreticular cells in the surrounding medulla.
Electron microscopy of a Hassall corpuscle:
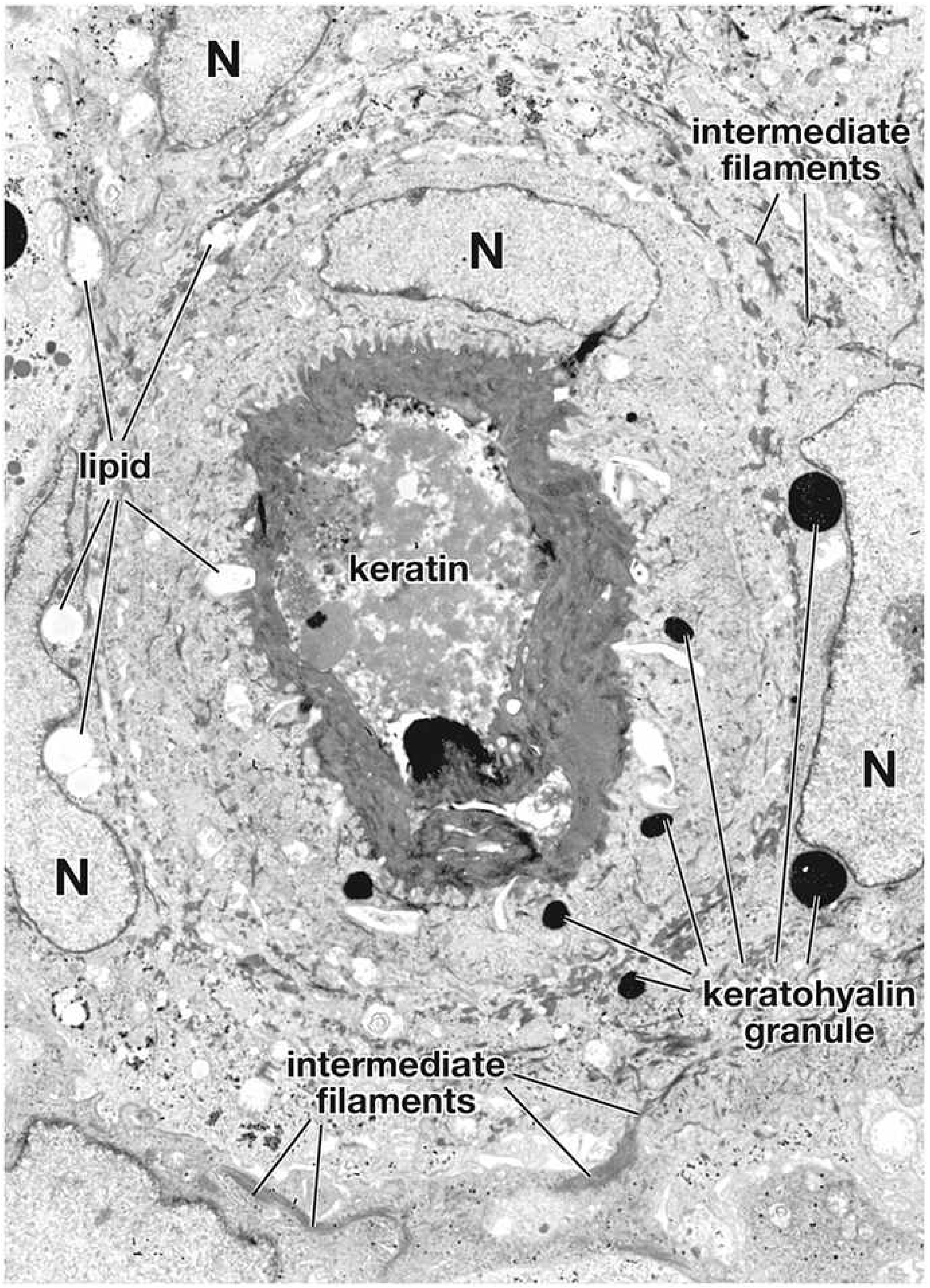
TEM at x5,000: Nuclei (N) of concentrically arranged type VI epithelioreticular cells surround a fully keratinized core. Cytoplasm contains intermediate filaments, keratohyalin granules, and lipid droplets - reflecting their origin from oropharyngeal (endodermal) epithelium.
Key features of Hassall corpuscles:
- Whorls of degenerated, keratinized medullary epithelial cells (type VI TECs)
- Contain keratohyalin granules, intermediate filaments, lipid droplets
- Produce IL-4 and IL-7 - promote T-cell differentiation
- Unique to the thymus (no other lymphoid organ has them)
(Histology: A Text and Atlas, p. 1232-1234; Robbins, p. 591)
6. T-Cell Education (Thymic Selection)
The thymus operates like a "university" for T cells. The process:
Step 1 - Arrival & Proliferation
Bone marrow-derived lymphoid progenitors enter the cortex via venules. They proliferate and begin TCR gene rearrangement. Initially they are "double negative" (CD4-, CD8-), then become "double positive" (CD4+, CD8+).
Step 2 - Positive Selection (Cortex)
Thymocytes must show that their TCR can recognize self-MHC presented by type II TECs.
- Recognizes MHC I → becomes CD8+ cytotoxic T cell
- Recognizes MHC II → becomes CD4+ helper T cell
- Fails to recognize either → dies by apoptosis (neglect)
- This generates MHC restriction
Step 3 - Negative Selection (Medulla)
Cells passing positive selection move to the medulla. Here type IV-VI TECs (expressing AIRE - autoimmune regulator protein) display tissue-specific self-antigens from every organ of the body. T cells that bind these with too high avidity are deleted by apoptosis.
- Eliminates autoreactive clones
- Generates central tolerance
- AIRE mutations → APECED syndrome (multiorgan autoimmunity)
Result: Only ~2% of thymocytes survive to leave as mature naïve T cells.
(Histology: A Text and Atlas, p. 1237-1240)
7. Thymic Involution
| Age | Appearance |
|---|---|
| Birth - puberty | Large, active; prominent cortex and medulla |
| After puberty | Progressive replacement by adipose tissue |
| Elderly | Barely identifiable; mostly fat with small residual lymphoid islands |
The involuted thymus still retains residual function - T-cell production can be re-stimulated (e.g., after bone marrow transplantation). Rapid involutional changes also occur with severe illness, malnutrition, and HIV infection.
(Junqueira's Basic Histology, p. 685-686)
8. Development & Clinical Correlates
Embryology: From the 3rd (and sometimes 4th) pharyngeal pouch (endoderm). The same pouch also gives rise to the inferior parathyroid glands - hence ectopic parathyroid tissue is a common finding within the thymus.
| Condition | Mechanism | Feature |
|---|---|---|
| DiGeorge syndrome | 22q11 deletion → absent 3rd pharyngeal pouch development | Thymic aplasia/hypoplasia → absent T cells → severe cell-mediated immunodeficiency; also hypoparathyroidism, cardiac defects |
| Thymic follicular hyperplasia | B-cell germinal centers appear in thymus (normally absent) | Associated with myasthenia gravis (70% of cases); also other autoimmune diseases |
| Thymoma | Neoplasm of thymic epithelial cells | Associated with myasthenia gravis, pure red cell aplasia, hypogammaglobulinemia |
| Thymic cysts | Incidental; lined by stratified-columnar epithelium | Usually <4 cm, rarely significant alone; must rule out neoplasm if symptomatic |
| APECED syndrome | AIRE gene mutation | Multiorgan autoimmunity + mucocutaneous candidiasis |
(Robbins, Cotran & Kumar, p. 591-592)
Sources:
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology, pp. 1227-1240
- Junqueira's Basic Histology - Text and Atlas, 17e, pp. 685-686
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 591-592
- Gray's Anatomy for Students, pp. 252-253
This is a shared conversation. Sign in to Orris to start your own chat.