Guide me about management and diagnosis of tinea capitis with reference to latest updates
Reading File
Finding Sources
Searching PubMed
"tinea capitis" AND diagnosis AND treatment
Searching the Web
tinea capitis diagnosis management guidelines 2024 2025 latest update
Reading File
Reading File
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC12707599
Reading Article
PMID: 39396816
Reading File
Reading File
Searching PubMed
"tinea capitis" AND terbinafine AND griseofulvin
Reading File
Reading Article
PMID: 38786712
Loading Image
Loading Image
Loading Image
Finding Sources
I now have comprehensive, authoritative data from multiple dermatology textbooks plus the latest 2024-2025 evidence. Let me compose the full answer.
Tinea Capitis: Diagnosis and Management
Overview
Tinea capitis is a dermatophyte infection of the scalp and hair follicles, caused exclusively by species in the genera Trichophyton and Microsporum. It is primarily a disease of children (ages 3-14), though adults - especially postmenopausal women and immunocompromised individuals - can also be affected. A critical feature is that oral systemic therapy is always required because topical agents cannot penetrate the hair follicle.
Epidemiology and Causative Organisms
- United States/UK: T. tonsurans accounts for >90% of cases; has a predilection for individuals with Afro-textured hair. African American and Latino children are disproportionately affected.
- Europe: M. canis historically dominant, but T. tonsurans has emerged as a major agent reflecting immigration patterns. T. violaceum incidence is also rising in western/Mediterranean Europe.
- Asia: T. violaceum and M. ferrugineum predominate in East Asia.
- Africa: T. soudanense, T. violaceum, T. schoenleinii, and Microsporum spp. drive large-scale epidemics.
- Pets: M. canis (cats/dogs) is the main zoonotic cause worldwide.
2024-2025 update: T. violaceum infections are increasingly reported in the US and Europe, likely due to immigration. Antifungal-resistant strains are an emerging concern - particularly in Europe, with resistance to terbinafine and even voriconazole being described. Antifungal stewardship is now emphasized. (Hill et al., J Fungi 2024, PMID: 38786712)
Patterns of Hair Invasion
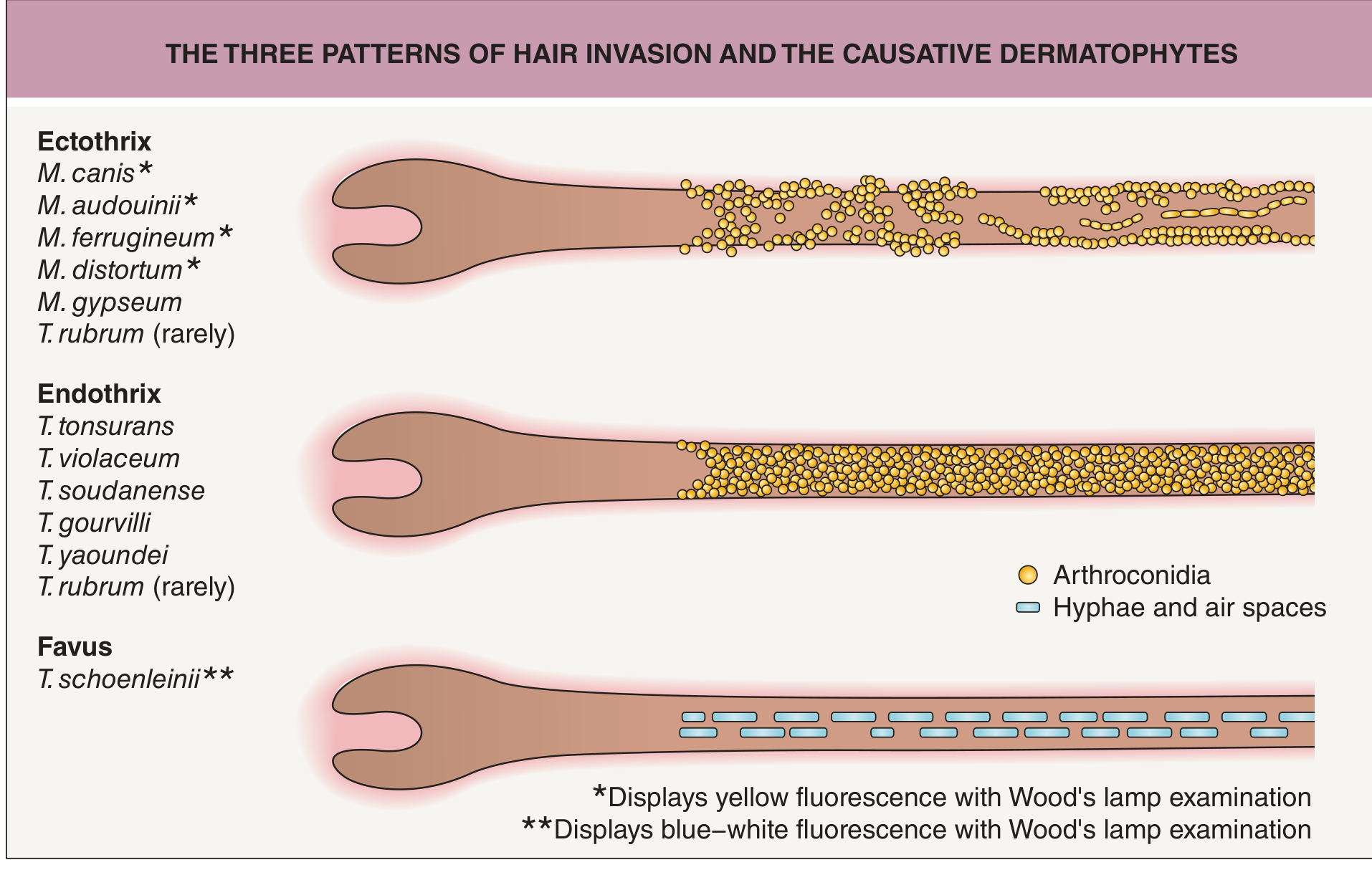
| Pattern | Organism | Wood's Lamp | Mechanism |
|---|---|---|---|
| Endothrix | T. tonsurans, T. violaceum, T. soudanense | Non-fluorescent | Arthroconidia within the hair shaft; hair breaks at scalp level ("black dots") |
| Ectothrix | M. canis, M. audouinii, M. ferrugineum, M. distortum, M. gypseum | Yellow-green fluorescent* | Arthroconidia outside the hair shaft; cuticle destruction |
| Favus | T. schoenleinii | Blue-white fluorescent | Hyphae and air spaces within hair; sulfur-yellow crusts (scutula); may cause scarring alopecia |
*Ectothrix Microsporum species fluoresce; some Trichophyton ectothrix species do not.
Clinical Presentations
Tinea capitis has a wide spectrum of presentations:
1. Non-inflammatory / Seborrheic Type
Subtle scalp scaling resembling dandruff or seborrheic dermatitis. Often caused by T. tonsurans. Easily missed.
2. Gray Patch Tinea Capitis
Dry, scaly, round patches of alopecia with dull, grey, broken hairs. Typical of M. audouinii. Less inflammatory.
3. Black Dot Tinea Capitis
Hair breaks off at the scalp surface, leaving black dots at follicular openings. Caused by endothrix organisms (T. tonsurans, T. violaceum). The image below shows this presentation:

4. Kerion Celsii (Inflammatory Type)
A boggy, tender, purulent, crusted mass on the scalp representing an exaggerated inflammatory host response to the dermatophyte. Associated with pus-discharging follicles, marked alopecia, and painful regional lymphadenopathy. Can cause permanent scarring alopecia if not treated promptly.

5. Favus
Extremely rare in the US. Concave sulfur-yellow crusts (scutulae) around loose, wiry hairs. "Mousy" odor. Can lead to smooth, scarred, paper-white patches.
Key associated finding: Posterior cervical and posterior auricular lymphadenopathy is a helpful distinguishing feature from non-fungal alopecia (e.g., alopecia areata).
Diagnosis
Clinical Diagnosis
Typical tinea capitis - pruritus, scalp scaling, alopecia with broken hairs, and posterior cervical/suboccipital lymphadenopathy - can be treated empirically in children. If lymphadenopathy is absent, confirmatory testing is recommended before starting oral antifungals. (PMC12707599, 2025)
1. Wood's Lamp (UV 365 nm)
- Positive (yellow-green fluorescence): M. canis, M. audouinii, M. ferrugineum, M. distortum (ectothrix organisms)
- Positive (blue-white): T. schoenleinii (favus)
- Negative: T. tonsurans, T. violaceum (most common US/UK organisms) - do NOT fluoresce
- Dandruff fluoresces bright blue-white; infected hair fluoresces yellow-green due to pteridine
2025 update: Wood's lamp is most useful for M. canis in children, with recent studies confirming its role in early detection. Since T. tonsurans does not fluoresce, a negative Wood's lamp does NOT rule out tinea capitis.
2. KOH (Potassium Hydroxide) Preparation
- Sensitivity: 59-73%
- Collect broken hairs (black dots) or scalp scrapings
- Endothrix: chains of large spores inside the hair shaft
- Ectothrix: spores outside the hair shaft, cuticle destruction
3. Fungal Culture (Gold Standard)
- Sensitivity: 51-97% (higher than KOH)
- Method: Moisten a cotton swab or toothbrush with tap water and rub over scalp lesion, then inoculate Sabouraud dextrose agar or dermatophyte test medium (DTM)
- Results in 1-4 weeks
- High false-negative rate in kerion due to inflammatory immune response destroying hyphae
- Important for species identification (affects drug choice)
4. Dermoscopy / Trichoscopy
- Increasingly used as a non-invasive adjunct
- Characteristic findings: "comma hairs," "corkscrew hairs," "morse code hairs," and dystrophic broken hairs are pathognomonic for tinea capitis
- Highly useful for distinguishing from alopecia areata (which shows exclamation mark hairs, yellow dots)
5. PCR Testing
- Emerging modality; faster than culture
- Especially useful for identifying species and detecting resistance mutations
- Now included in updated guidelines as a confirmatory test option (PMC12707599, 2025)
6. Histopathology (Periodic Acid-Schiff / PAS Stain)
- Shows arthroconidia and hyphae within the hair shaft to the level of Adamson's fringe
- Used when other tests are inconclusive
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Seborrheic dermatitis | No alopecia, greasy scale, KOH negative |
| Alopecia areata | Exclamation mark hairs, no scale, no lymphadenopathy |
| Psoriasis of scalp | Thick silvery scale, nail changes, family history |
| Bacterial folliculitis / abscess | Culture bacteria, rule out kerion before draining |
| Trichotillomania | Irregular broken hairs, no scale, psychiatric history |
Key pitfall: Before draining a scalp abscess in a child, always consider kerion and send fungal culture. - Andrews' Diseases of the Skin
Management
Principle: Always Use Systemic (Oral) Antifungals
Topical antifungals alone are ineffective because they cannot penetrate the hair follicle. Oral therapy + adjunctive antifungal shampoo is the standard approach.
First-Line Systemic Agents
Terbinafine (Preferred for Trichophyton spp.)
- Mechanism: Allylamine - inhibits squalene epoxidase, accumulates in keratin
- Children:
- <20 kg: 62.5 mg/day
- 20-40 kg: 125 mg/day
-
40 kg: 250 mg/day
- Adults: 250 mg/day
- Duration:
- T. tonsurans: 2-6 weeks
- M. canis: 8-12 weeks (terbinafine less effective for Microsporum)
- Evidence: A Cochrane review of RCTs confirms terbinafine is equally effective to griseofulvin with shorter treatment courses. (Grade A, PMC12707599)
- Note: Terbinafine granules can be mixed with food (for younger children). Crushed generic tablets are an off-label alternative if granules are unavailable.
Griseofulvin (Preferred for Microsporum spp.)
- Mechanism: Fungistatic; binds microtubules and disrupts mitosis; concentrates in keratin
- Dose: Microsize: 20-25 mg/kg/day (max 1g/day); Ultramicrosize: 10-15 mg/kg/day
- Duration: 6-8 weeks (longer than terbinafine)
- Take with fatty meal to enhance absorption
- FDA approved for tinea capitis in children >2 years
- Superior to terbinafine for M. canis infections
- 2024 update: Griseofulvin availability has become limited in some countries, raising questions about alternative first-line agents. (Bonifaz et al., Expert Rev Anti Infect Ther 2024, PMID: 39297581)
Alternative Systemic Agents
| Drug | Dose | Duration | Notes |
|---|---|---|---|
| Itraconazole | 5 mg/kg/day | 2-4 weeks | Alternative for both Trichophyton and Microsporum; pulse therapy also effective |
| Fluconazole | 6 mg/kg/day (pulse: weekly 8 mg/kg) | 3-6 weeks | FDA approved in infancy for fungal infections; useful when griseofulvin unavailable |
| Voriconazole | Not routinely used | - | Consider for resistant or unusual strains only |
Adjunctive Topical Therapy (Reduces Transmission)
- Selenium sulfide 2.5% shampoo or ketoconazole 2% shampoo or ciclopirox 1.5% shampoo
- Use every other day or twice weekly for the first 2 weeks of oral therapy
- Reduces spore shedding and transmission to household contacts
- Household/close contacts should also use sporicidal shampoo for 2-4 weeks
Management of Kerion
- Start oral antifungal immediately - do not wait for culture results
- Consider short course of oral corticosteroids (e.g., prednisolone 1 mg/kg/day for 1-2 weeks) alongside antifungals to reduce inflammation and risk of scarring alopecia
- Do not incise and drain - this is not a bacterial abscess
- Antibacterials are NOT routinely required (secondary bacterial infection is uncommon)
- Hair typically regrows after adequate treatment, but delay risks permanent scarring
Management of Asymptomatic Carriers
- 5-15% of urban children in Western countries have positive scalp cultures but no symptoms
- In one study, 60% of African American children with positive cultures were asymptomatic
- Asymptomatic contacts: No KOH/culture needed but consider empiric sporicidal shampoo for 2-4 weeks
Infection Control and Prevention
- Children may return to school after starting oral therapy (no need to miss school)
- For the first 14 days: avoid sharing combs, brushes, hats, helmets, or pillowcases
- Avoid head-to-head contact sports (wrestling) for 14 days
- Discard or disinfect combs, brushes, and headwear used by the patient
- Screen all household members clinically (but not necessarily with cultures)
- Antifungal shampoo for all household contacts until patient is cured
Follow-Up
- Clinical reassessment at end of treatment course
- Routine follow-up cultures are not needed if there is clear clinical improvement
- If no improvement: check adherence, consider culture for species ID and resistance testing
Special Populations
Adults with Tinea Capitis
- Postmenopausal women and immunocompromised adults are most affected
- No widely accepted separate adult guidelines exist; same drugs used as in children at adult doses
- Risk factors: crowded living, animal exposure, immunosuppression, household contact with infected child
- Delayed diagnosis is common in adults, raising risk of scarring alopecia (Hill et al., J Fungi 2024 - PMID: 38786712)
Immunocompromised Patients
- May require longer courses or higher doses
- Species identification and susceptibility testing are especially important
- Consider itraconazole or fluconazole as alternatives
Summary: Drug-Species Matching Guide
| Causative Species | Preferred Drug |
|---|---|
| T. tonsurans (US/UK dominant) | Terbinafine (4-6 wks) |
| T. violaceum | Terbinafine |
| M. canis (worldwide) | Griseofulvin (6-8 wks) |
| M. audouinii | Griseofulvin |
| Griseofulvin unavailable | Itraconazole or Fluconazole |
| Antifungal-resistant strains | Specialist referral; susceptibility testing |
2024-2025 Key Updates
- Terbinafine is now the preferred first-line agent for Trichophyton species - Cochrane evidence (Grade A) confirms equivalence to griseofulvin with shorter courses. (PMC12707599, 2025)
- PCR testing is now listed alongside KOH and culture as a diagnostic option in updated guidelines.
- Griseofulvin supply issues in some countries are reshaping first-line therapy decisions, with itraconazole and fluconazole positioned as alternatives (PMID: 39297581).
- Emerging antifungal resistance - particularly among T. violaceum and related species in Europe - requires antifungal stewardship; avoid combination antifungal-corticosteroid products as they promote resistance (PMC12707599).
- Adults with tinea capitis (especially postmenopausal Black women) are a neglected and under-recognized population; screening awareness needs to improve (PMID: 38786712).
- Wood's lamp with LED technology is being re-evaluated for M. canis detection in children (Sun et al., Photodiagnosis Photodyn Ther 2025).
Sources:
- Dermatology: 2-Volume Set 5e (Elsevier), p. 1609
- Andrews' Diseases of the Skin 13e, p. 344
- Fitzpatrick's Dermatology 9e, Vol. 1-2
- Goodman & Gilman's Pharmacological Basis of Therapeutics
- Harriet Lane Handbook 23e (terbinafine dosing)
- PMC12707599 - "Diagnosis and Management of Tinea Infections," updated AAFP guidelines (2025)
- Hill RC et al., J Fungi 2024, PMID: 38786712 - Comprehensive review of tinea capitis in adults
- Bonifaz A et al., Expert Rev Anti Infect Ther 2024, PMID: 39297581 - Griseofulvin availability crisis
This is a shared conversation. Sign in to Orris to start your own chat.