Supine hypotension syndrome from anaesthesia textbooks for exam
Supine Hypotension Syndrome (Aortocaval Compression Syndrome)
Definition
Also called: aortocaval compression syndrome or inferior vena caval syndrome — Miller's Anesthesia, 10e
Incidence
| Finding | Incidence |
|---|---|
| IVC compression in supine position (term) | Nearly all term parturients |
| Symptomatic supine hypotension syndrome | 8–10% (Miller's) / ~5% (Morgan & Mikhail) |
| Aortoiliac artery compression | 15–20% of pregnant patients |
Pathophysiology
Step-by-step mechanism:
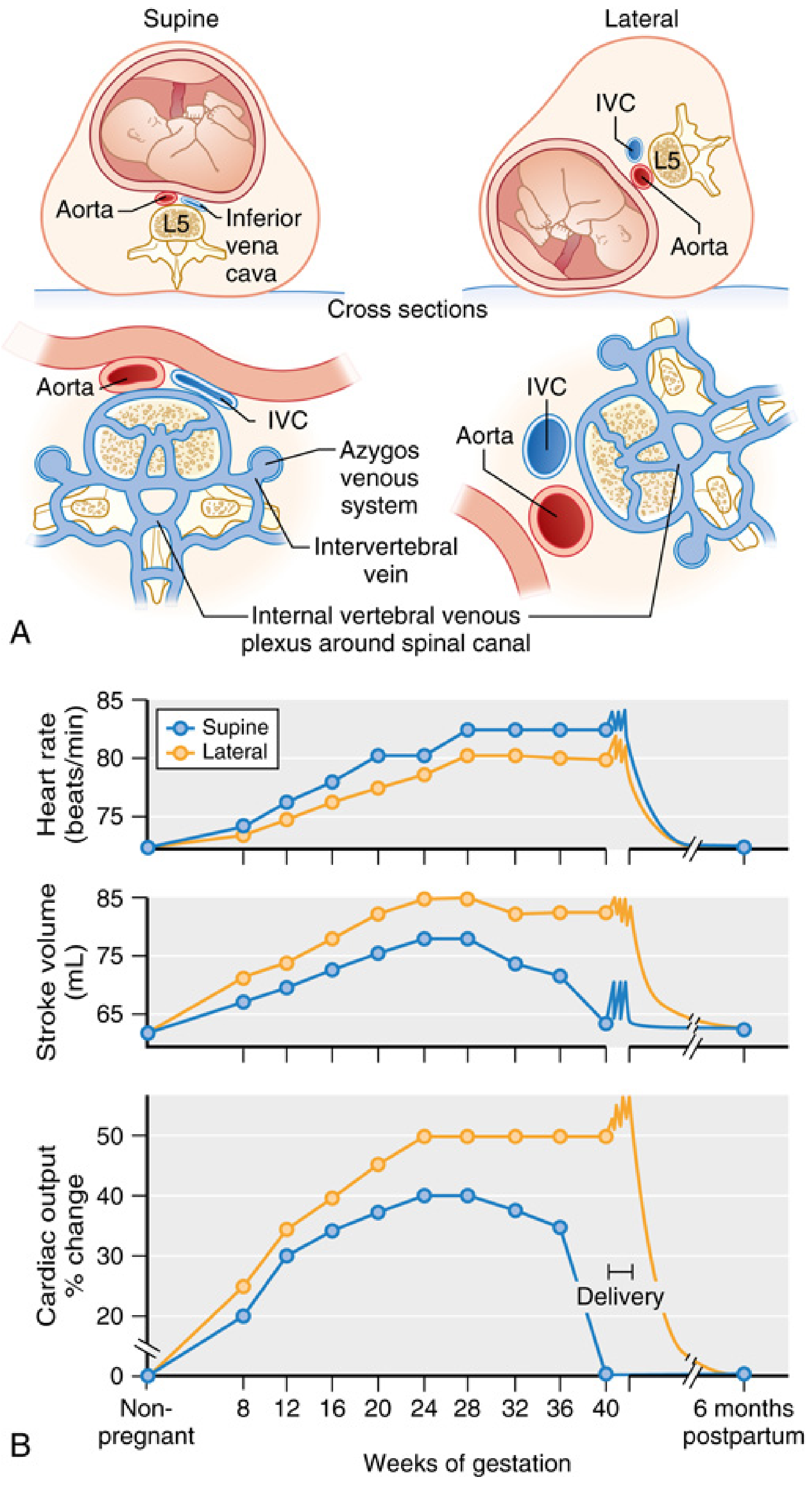
- Gravid uterus (significant from ~20 weeks, maximal at term) compresses the IVC against the lumbar vertebrae (L3–L5) in the supine position
- → Reduced venous return to the right heart → ↓ preload
- → ↓ Stroke volume → ↓ Cardiac output by 10–20% compared to lateral position
- Collateral return via epidural venous plexus, azygos, and vertebral veins (these become engorged)
- Simultaneous aortoiliac compression → ↓ uterine and placental perfusion
Clinical Features
| Symptom | Notes |
|---|---|
| Hypotension | MAP falls >15 mmHg |
| Tachycardia | HR rises >20 bpm (compensatory) |
| Diaphoresis / pallor | Sympathetic activation |
| Nausea and vomiting | Common |
| Dizziness / changes in mentation | Cerebral hypoperfusion |
Why Most Women Remain Asymptomatic
"The reduced sympathetic tone from neuraxial or general anesthetic techniques impairs the compensatory increase in vascular resistance and exacerbates the impact of hypotension from supine positioning." — Miller's Anesthesia, 10e
Consequences for the Fetus
- ↓ Uterine blood flow → fetal hypoxia, acidosis
- Aortoiliac compression reduces uterine artery flow even if maternal BP appears maintained (because collaterals may maintain maternal BP while uterine flow is still reduced)
- Can lead to fetal bradycardia and non-reassuring fetal heart rate patterns
Prevention and Management
Positioning (First-line)
- Left uterine displacement (LUD) — the cornerstone of prevention
- Options: lateral decubitus, right hip elevation 10–15 cm (wedge/blanket/table tilt)
- Historical standard: 15-degree left tilt
Controversy — Does 15° Tilt Work?
In an MRI study, IVC volume did not differ significantly between supine and 15° left-tilt. Only at 30° tilt did IVC volume increase. Additionally, in a RCT of spinal anaesthesia for caesarean section with phenylephrine infusion, there was no difference in neonatal acid-base status between supine and 15° left-tilt positions. — Miller's Anesthesia, 10e
Vasopressors (when positioning alone is insufficient)
| Drug | Notes |
|---|---|
| Phenylephrine (α-agonist) | Currently preferred — more effective, associated with less fetal acidosis than ephedrine |
| Ephedrine (α + β agonist) | Traditional "vasopressor of choice" historically — associated with more fetal acidosis (crosses placenta, stimulates fetal metabolism) |
"Clinical studies suggest that the α-adrenergic agonist phenylephrine is more effective in treating hypotension in pregnant patients and is associated with less fetal acidosis than ephedrine." — Morgan & Mikhail's Clinical Anesthesiology, 7e (Key Concept 6)
Timing — When Is the Risk Highest?
| Timing | Reason |
|---|---|
| ≥20 weeks gestation | Uterus large enough to compress IVC |
| Term (≥36 weeks) | Maximum compression |
| During spinal/epidural anaesthesia | Loss of compensatory sympathetic tone |
| Immediately after delivery | Sudden relief of IVC compression → massive ↑ venous return → CO surges up to 80% above late third-trimester values — greatest cardiac strain |
Additional Sequelae of Chronic IVC Compression
- Ankle oedema
- Varicose veins
- Increased risk of lower extremity DVT (venous stasis)
High-Yield Exam Points
- IVC compressed in nearly ALL term patients; only 5–10% symptomatic
- Definition: MAP ↓ >15 mmHg + HR ↑ >20 bpm
- Mechanism: IVC compression → ↓ venous return → ↓ CO; collaterals via azygos/epidural veins
- Neuraxial and general anaesthesia abolish the sympathetic compensatory response → exacerbate hypotension
- Prevention: left uterine displacement (10–15 cm wedge under right hip)
- Vasopressor of choice: phenylephrine > ephedrine (less fetal acidosis)
- Post-delivery: sudden relief → CO surges 80% → greatest haemodynamic stress
- Aortic compression (not just IVC) can reduce uterine perfusion even when maternal BP is "normal"
How to save this as a pdf ?
ls -la /home/daytona/workspace/
mkdir -p /home/daytona/workspace/notes && echo "done"
~/notes/supine_hypotension.md
# Supine Hypotension Syndrome (Aortocaval Compression Syndrome) ## Definition Supine hypotension syndrome is defined as a **decrease in mean arterial pressure of >15 mm Hg** with a **compensatory increase in heart rate of >20 beats/min** when a term parturient lies supine, caused by compression of the inferior vena cava (IVC) and abdominal aorta by the gravid uterus. Also called: **aortocaval compression syndrome** or **inferior vena caval syndrome** *(Miller's Anesthesia, 10e)* --- ## Incidence | Finding | Incidence | |---|---| | IVC compression in supine position (term) | Nearly **all** term parturients | | Symptomatic supine hypotension syndrome | **8–10%** (Miller's) / **~5%** (Morgan & Mikhail) | | Aortoiliac artery compression | **15–20%** of pregnant patients | The discrepancy between universal IVC compression and low symptomatic incidence is explained by **compensatory mechanisms** (see below). --- ## Pathophysiology ### Step-by-step mechanism: 1. **Gravid uterus** (significant from ~20 weeks, maximal at term) compresses the **IVC against the lumbar vertebrae** (L3–L5) in the supine position 2. → Reduced venous return to the right heart → ↓ preload 3. → ↓ Stroke volume → ↓ Cardiac output by **10–20%** compared to lateral position 4. Collateral return via **epidural venous plexus, azygos, and vertebral veins** (these become engorged) 5. Simultaneous **aortoiliac compression** → ↓ uterine and placental perfusion --- ## Clinical Features | Symptom | Notes | |---|---| | Hypotension | MAP falls >15 mmHg | | Tachycardia | HR rises >20 bpm (compensatory) | | Diaphoresis / pallor | Sympathetic activation | | Nausea and vomiting | Common | | Dizziness / changes in mentation | Cerebral hypoperfusion | *(Morgan & Mikhail's Clinical Anesthesiology, 7e; Miller's Anesthesia, 10e)* --- ## Why Most Women Remain Asymptomatic The key compensatory mechanism is a **reflexive increase in peripheral sympathetic nervous system activity** → ↑ systemic vascular resistance → maintains arterial blood pressure despite ↓ cardiac output. **This is critically important for anaesthesia:** > "The reduced sympathetic tone from neuraxial or general anesthetic techniques **impairs** the compensatory increase in vascular resistance and **exacerbates** the impact of hypotension from supine positioning." *(Miller's Anesthesia, 10e)* This is why spinal/epidural anaesthesia (especially for caesarean section) dramatically increases the risk and severity of hypotension in the supine parturient. --- ## Consequences for the Fetus - ↓ Uterine blood flow → fetal hypoxia, acidosis - Aortoiliac compression reduces uterine artery flow even if maternal BP appears maintained - Can lead to **fetal bradycardia** and **non-reassuring fetal heart rate** patterns --- ## Prevention and Management ### Positioning (First-line) - **Left uterine displacement (LUD)** — the cornerstone of prevention - Options: lateral decubitus, **right hip elevation 10–15 cm** (wedge/blanket/table tilt) - Historical standard: **15-degree left tilt** ### Controversy — Does 15° Tilt Work? > In an MRI study, IVC volume did **not differ significantly** between supine and 15° left-tilt. Only at **30° tilt** did IVC volume increase. In a RCT of spinal anaesthesia for caesarean section with phenylephrine infusion, there was **no difference in neonatal acid-base status** between supine and 15° left-tilt positions. *(Miller's Anesthesia, 10e)* **Practical implication:** With adequate vasopressor support, the 15° tilt may be less critical than previously thought, but LUD remains standard practice. ### Vasopressors (when positioning alone is insufficient) | Drug | Notes | |---|---| | **Phenylephrine** (α-agonist) | **Currently preferred** — more effective, associated with **less fetal acidosis** than ephedrine | | **Ephedrine** (α + β agonist) | Traditional choice historically — associated with **more fetal acidosis** (crosses placenta, stimulates fetal metabolism) | > "Clinical studies suggest that the α-adrenergic agonist **phenylephrine** is more effective in treating hypotension in pregnant patients and is associated with less fetal acidosis than ephedrine." *(Morgan & Mikhail's Clinical Anesthesiology, 7e — Key Concept 6)* --- ## Timing — When Is the Risk Highest? | Timing | Reason | |---|---| | ≥20 weeks gestation | Uterus large enough to compress IVC | | Term (≥36 weeks) | Maximum compression | | **During spinal/epidural anaesthesia** | Loss of compensatory sympathetic tone | | **Immediately after delivery** | Sudden relief of IVC compression → CO surges **up to 80% above late third-trimester values** — greatest cardiac strain | --- ## Additional Sequelae of Chronic IVC Compression - Ankle oedema - Varicose veins - Increased risk of **lower extremity DVT** (venous stasis) --- ## High-Yield Exam Points 1. IVC compressed in **nearly ALL** term patients; only **5–10%** symptomatic 2. Definition: MAP ↓ >15 mmHg + HR ↑ >20 bpm 3. Mechanism: IVC compression → ↓ venous return → ↓ CO; collaterals via **azygos/epidural veins** 4. Neuraxial and general anaesthesia abolish the sympathetic compensatory response → **exacerbate** hypotension 5. Prevention: **left uterine displacement** (10–15 cm wedge under right hip) 6. Vasopressor of choice: **phenylephrine** > ephedrine (less fetal acidosis) 7. Post-delivery: sudden relief → CO surges 80% → greatest haemodynamic stress 8. Aortic compression (not just IVC) can reduce uterine perfusion even when maternal BP is "normal" --- *Sources: Miller's Anesthesia (10e), Morgan & Mikhail's Clinical Anesthesiology (7e)*
pandoc /home/daytona/workspace/notes/supine_hypotension.md -o /home/daytona/workspace/notes/Supine_Hypotension_Syndrome.pdf --pdf-engine=xelatex -V geometry:margin=2cm -V fontsize=11pt -V mainfont="DejaVu Serif" 2>&1
pandoc /home/daytona/workspace/notes/supine_hypotension.md -o /home/daytona/workspace/notes/Supine_Hypotension_Syndrome.pdf --pdf-engine=weasyprint 2>&1 || pandoc /home/daytona/workspace/notes/supine_hypotension.md -o /home/daytona/workspace/notes/Supine_Hypotension_Syndrome.pdf --pdf-engine=wkhtmltopdf 2>&1
python3 -c "import markdown2; print('ok')" 2>&1 && python3 -c "from reportlab.platypus import SimpleDocTemplate; print('reportlab ok')" 2>&1
python3 -c "from reportlab.platypus import SimpleDocTemplate; print('reportlab ok')" 2>&1
~/notes/make_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm
from reportlab.lib import colors
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle, HRFlowable
)
from reportlab.lib.enums import TA_LEFT, TA_CENTER
OUTPUT = "/home/daytona/workspace/notes/Supine_Hypotension_Syndrome.pdf"
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
leftMargin=2*cm, rightMargin=2*cm,
topMargin=2*cm, bottomMargin=2*cm,
title="Supine Hypotension Syndrome"
)
styles = getSampleStyleSheet()
# Custom styles
h1 = ParagraphStyle("H1", parent=styles["Heading1"], fontSize=16, textColor=colors.HexColor("#1a3a5c"), spaceAfter=8)
h2 = ParagraphStyle("H2", parent=styles["Heading2"], fontSize=12, textColor=colors.HexColor("#1a3a5c"), spaceBefore=12, spaceAfter=4)
body = ParagraphStyle("Body", parent=styles["Normal"], fontSize=10, leading=15, spaceAfter=5)
bullet = ParagraphStyle("Bullet", parent=styles["Normal"], fontSize=10, leading=15, leftIndent=18, spaceAfter=3, bulletIndent=6)
blockquote = ParagraphStyle("Quote", parent=styles["Normal"], fontSize=9.5, leading=14,
leftIndent=20, rightIndent=10, textColor=colors.HexColor("#333333"),
backColor=colors.HexColor("#f0f4f8"), borderPadding=(6,6,6,6),
spaceAfter=8)
source = ParagraphStyle("Source", parent=styles["Normal"], fontSize=8.5, textColor=colors.grey, spaceAfter=6, leftIndent=20)
bold_note = ParagraphStyle("BoldNote", parent=styles["Normal"], fontSize=10, leading=14, textColor=colors.HexColor("#c0392b"), spaceAfter=5)
table_header = ParagraphStyle("TH", parent=styles["Normal"], fontSize=9, textColor=colors.white, fontName="Helvetica-Bold")
table_cell = ParagraphStyle("TC", parent=styles["Normal"], fontSize=9, leading=12)
def hr():
return HRFlowable(width="100%", thickness=0.5, color=colors.HexColor("#cccccc"), spaceAfter=6, spaceBefore=4)
def h(text, style=h2):
return Paragraph(text, style)
def p(text):
return Paragraph(text, body)
def b(text):
return Paragraph(f"• {text}", bullet)
def q(text):
return Paragraph(text, blockquote)
def src(text):
return Paragraph(text, source)
def make_table(headers, rows, col_widths=None):
data = [[Paragraph(h, table_header) for h in headers]]
for row in rows:
data.append([Paragraph(str(c), table_cell) for c in row])
t = Table(data, colWidths=col_widths, repeatRows=1)
t.setStyle(TableStyle([
("BACKGROUND", (0,0), (-1,0), colors.HexColor("#1a3a5c")),
("ROWBACKGROUNDS", (0,1), (-1,-1), [colors.HexColor("#f7f9fc"), colors.white]),
("GRID", (0,0), (-1,-1), 0.4, colors.HexColor("#cccccc")),
("TOPPADDING", (0,0), (-1,-1), 5),
("BOTTOMPADDING", (0,0), (-1,-1), 5),
("LEFTPADDING", (0,0), (-1,-1), 6),
("RIGHTPADDING", (0,0), (-1,-1), 6),
("VALIGN", (0,0), (-1,-1), "TOP"),
]))
return t
story = []
# Title
story.append(Paragraph("Supine Hypotension Syndrome", h1))
story.append(Paragraph("Aortocaval Compression Syndrome — Anaesthesia Exam Notes",
ParagraphStyle("sub", parent=styles["Normal"], fontSize=11, textColor=colors.HexColor("#555555"), spaceAfter=4)))
story.append(Paragraph("Sources: <i>Miller's Anesthesia 10e & Morgan & Mikhail's Clinical Anesthesiology 7e</i>",
ParagraphStyle("sub2", parent=styles["Normal"], fontSize=9, textColor=colors.grey, spaceAfter=10)))
story.append(hr())
# Definition
story.append(h("Definition"))
story.append(p("Supine hypotension syndrome is defined as a <b>decrease in mean arterial pressure of >15 mm Hg</b> with a <b>compensatory increase in heart rate of >20 beats/min</b> when a term parturient lies supine, caused by compression of the IVC and abdominal aorta by the gravid uterus."))
story.append(p("Also called: <b>aortocaval compression syndrome</b> or <b>inferior vena caval syndrome</b>"))
# Incidence
story.append(h("Incidence"))
story.append(make_table(
["Finding", "Incidence"],
[
["IVC compression in supine position (term)", "Nearly ALL term parturients"],
["Symptomatic supine hypotension syndrome", "8–10% (Miller's) / ~5% (Morgan & Mikhail)"],
["Aortoiliac artery compression", "15–20% of pregnant patients"],
],
col_widths=[10*cm, 6*cm]
))
story.append(Spacer(1, 6))
story.append(p("The discrepancy between universal IVC compression and low symptomatic incidence is explained by <b>compensatory mechanisms</b> (see below)."))
# Pathophysiology
story.append(h("Pathophysiology"))
story.append(p("<b>Step-by-step mechanism:</b>"))
story.append(b("<b>Gravid uterus</b> (significant from ~20 weeks, maximal at term) compresses the <b>IVC against the lumbar vertebrae (L3–L5)</b> in the supine position"))
story.append(b("→ Reduced venous return to the right heart → ↓ preload"))
story.append(b("→ ↓ Stroke volume → ↓ Cardiac output by <b>10–20%</b> compared to lateral position"))
story.append(b("Collateral venous return via <b>epidural venous plexus, azygos, and vertebral veins</b> (these become engorged)"))
story.append(b("Simultaneous <b>aortoiliac compression</b> → ↓ uterine and placental perfusion"))
# Clinical Features
story.append(h("Clinical Features"))
story.append(make_table(
["Symptom", "Notes"],
[
["Hypotension", "MAP falls >15 mmHg"],
["Tachycardia", "HR rises >20 bpm (compensatory)"],
["Diaphoresis / pallor", "Sympathetic activation"],
["Nausea and vomiting", "Common"],
["Dizziness / altered mentation", "Cerebral hypoperfusion"],
],
col_widths=[7*cm, 9*cm]
))
# Why most remain asymptomatic
story.append(h("Why Most Women Remain Asymptomatic"))
story.append(p("Key compensatory mechanism: <b>reflexive increase in peripheral sympathetic nervous system activity</b> → ↑ systemic vascular resistance → maintains arterial BP despite ↓ cardiac output."))
story.append(q('"The reduced sympathetic tone from neuraxial or general anesthetic techniques <b>impairs</b> the compensatory increase in vascular resistance and <b>exacerbates</b> the impact of hypotension from supine positioning."'))
story.append(src("— Miller's Anesthesia, 10e"))
story.append(p("This is why spinal/epidural anaesthesia (especially for caesarean section) dramatically increases the risk and severity of hypotension."))
# Fetal consequences
story.append(h("Consequences for the Fetus"))
story.append(b("↓ Uterine blood flow → fetal hypoxia, acidosis"))
story.append(b("Aortoiliac compression reduces uterine artery flow even if maternal BP appears maintained (collaterals maintain maternal BP while uterine flow is still reduced)"))
story.append(b("Can lead to <b>fetal bradycardia</b> and <b>non-reassuring fetal heart rate</b> patterns"))
# Prevention and management
story.append(h("Prevention and Management"))
story.append(p("<b>Positioning (First-line):</b>"))
story.append(b("<b>Left uterine displacement (LUD)</b> — cornerstone of prevention"))
story.append(b("Right hip elevation <b>10–15 cm</b> (wedge/blanket/table tilt)"))
story.append(b("Historical standard: <b>15-degree left tilt</b>"))
story.append(Spacer(1, 4))
story.append(p("<b>Controversy — Does 15° Tilt Work?</b>"))
story.append(q("In an MRI study, IVC volume did <b>not differ significantly</b> between supine and 15° left-tilt. Only at <b>30° tilt</b> did IVC volume increase. In a RCT of spinal anaesthesia for caesarean section with phenylephrine infusion, there was <b>no difference in neonatal acid-base status</b> between supine and 15° left-tilt positions."))
story.append(src("— Miller's Anesthesia, 10e"))
story.append(p("<b>Practical implication:</b> With adequate vasopressor support, the 15° tilt may be less critical than previously thought, but LUD remains standard practice."))
story.append(Spacer(1, 4))
story.append(p("<b>Vasopressors (when positioning alone is insufficient):</b>"))
story.append(make_table(
["Drug", "Notes"],
[
["Phenylephrine (α-agonist)", "Currently PREFERRED — more effective, less fetal acidosis than ephedrine"],
["Ephedrine (α + β agonist)", "Traditional choice — more fetal acidosis (crosses placenta, stimulates fetal metabolism)"],
],
col_widths=[5*cm, 11*cm]
))
story.append(Spacer(1, 4))
story.append(q('"Clinical studies suggest that the α-adrenergic agonist <b>phenylephrine</b> is more effective in treating hypotension in pregnant patients and is associated with less fetal acidosis than ephedrine."'))
story.append(src("— Morgan & Mikhail's Clinical Anesthesiology, 7e (Key Concept 6)"))
# Timing
story.append(h("When Is the Risk Highest?"))
story.append(make_table(
["Timing", "Reason"],
[
["≥20 weeks gestation", "Uterus large enough to compress IVC"],
["Term (≥36 weeks)", "Maximum compression"],
["During spinal/epidural anaesthesia", "Loss of compensatory sympathetic tone"],
["Immediately after delivery", "Sudden relief of IVC → CO surges up to 80% above late 3rd trimester — greatest cardiac strain"],
],
col_widths=[6*cm, 10*cm]
))
# Additional sequelae
story.append(h("Additional Sequelae of Chronic IVC Compression"))
story.append(b("Ankle oedema"))
story.append(b("Varicose veins"))
story.append(b("Increased risk of <b>lower extremity DVT</b> (venous stasis)"))
# High-yield exam points
story.append(h("High-Yield Exam Points ★"))
exam_points = [
"IVC compressed in <b>nearly ALL</b> term patients; only <b>5–10%</b> symptomatic",
"Definition: MAP ↓ >15 mmHg + HR ↑ >20 bpm",
"Mechanism: IVC compression → ↓ venous return → ↓ CO; collaterals via <b>azygos/epidural veins</b>",
"Neuraxial and general anaesthesia abolish sympathetic compensation → <b>exacerbate</b> hypotension",
"Prevention: <b>left uterine displacement</b> (10–15 cm wedge under right hip)",
"Vasopressor of choice: <b>phenylephrine</b> > ephedrine (less fetal acidosis)",
"Post-delivery: sudden IVC relief → CO surges 80% → greatest haemodynamic stress",
"Aortic compression (not just IVC) can reduce uterine perfusion even when maternal BP appears normal",
]
for ep in exam_points:
story.append(b(ep))
story.append(Spacer(1, 12))
story.append(hr())
story.append(Paragraph(
"<i>Sources: Miller's Anesthesia, 2-Volume Set, 10e (ISBN 9780323935920) & Morgan and Mikhail's Clinical Anesthesiology, 7e (ISBN 9781260473797)</i>",
ParagraphStyle("footer", parent=styles["Normal"], fontSize=8.5, textColor=colors.grey, alignment=TA_CENTER)
))
doc.build(story)
print(f"PDF saved to {OUTPUT}")
python3 /home/daytona/workspace/notes/make_pdf.py 2>&1
Supine Hypotension Syndrome
PDF Document · PDF