Galactocele, duct ectasia ,fibroadenosis ,breast abscess treatment
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple textbooks. Let me compile the full answer.
Benign Breast Conditions: Treatment
1. Galactocele
A galactocele is a milk retention cyst - round, well-circumscribed, and easily movable - occurring during or just after lactation, typically when breastfeeding frequency declines or ceases. It is caused by inspissated milk blocking a lactiferous duct.
Treatment
- Needle aspiration is both diagnostic and therapeutic - it produces thick, creamy material (may be tinged dark green or brown). Despite the appearance, the fluid is usually sterile.
- Single aspiration is usually curative; the cyst disappears completely in most cases.
- If it recurs, re-aspiration is done, or a nylon strand (2/0) may be passed to clear the blocked duct.
- Lactating mothers should be encouraged to continue breastfeeding.
- Surgical excision is rarely indicated, reserved only for symptomatic patients or infected galactoceles.
- Complications (inspissated material, calcification) are uncommon.
Bailey and Love's Short Practice of Surgery, 28th Ed; Sabiston Textbook of Surgery
2. Duct Ectasia
Duct ectasia is dilatation of the major milk ducts (>3 mm on ultrasound), filled with debris. It is a disorder of involution (part of ANDI - Aberrations of Normal Development and Involution). The debris acts as an irritant causing periductal inflammation and fibrosis, leading to nipple retraction. Much more common in smokers. Can progress to subareolar abscess and mammary duct fistula.
Presentation: Toothpaste-like or coloured (brown, green, mud) nipple discharge; central non-cyclical pain; subareolar tender mass. Can mimic carcinoma.
Treatment
- Triple assessment first (clinical + imaging + cytology/histology).
- Antibiotic therapy if inflammation or infection is present:
- Co-amoxiclav, flucloxacillin, ciprofloxacin, or cefixime plus anti-anaerobic cover (metronidazole or tinidazole) for 2-3 weeks.
- Coverage for aerobic and anaerobic organisms is essential.
- Needle aspiration of any associated abscess.
- Major mammary duct excision (Hadfield's operation) is indicated for:
- Profuse nipple discharge
- Subareolar abscess that does not resolve conservatively
- Mammary duct fistula
- Recurrent subareolar infections (excision of the entire subareolar duct complex after the acute phase resolves)
- In rare cases of recurrent infections, excision of the nipple and areola may be needed.
Bailey and Love's Short Practice of Surgery, 28th Ed; Sabiston Textbook of Surgery
3. Fibroadenosis (Fibrocystic Breast Changes / ANDI)
Fibroadenosis represents a spectrum of clinical and histologic findings (including adenosis, sclerosis, cysts, apocrine metaplasia, epithelial hyperplasia, and stromal fibrosis) most common in women aged 30-50 years. It is driven by an exaggerated response to hormones and growth factors.
Presentation: Cyclic or non-cyclic mastalgia, diffuse nodularity, tenderness, occasionally discrete cysts.
Treatment
Step 1 - Exclude cancer (triple assessment if any discrete mass)
Step 2 - Non-pharmacological (first line)
- Reassurance that the condition is benign
- Well-fitting firm support brassiere (especially a sports bra during the day)
- Flax seed 30 g daily or oil of evening primrose (rich in omega-3 fatty acids and γ-linolenic acid)
- Topical NSAIDs - diclofenac or piroxicam cream applied 4 times daily (useful for mild-moderate mastalgia)
Step 3 - Pharmacological (if VAS pain score >3/10)
| Drug | Dose | Duration |
|---|---|---|
| Tamoxifen | 10 mg daily | 3-6 months |
| Danazol | 50-300 mg daily | 3-6 months |
| Ormeloxifene (Centchroman) | 30 mg twice weekly | 3-6 months (effective for both cyclical and non-cyclical mastalgia and nodularity) |
| LHRH agonist ± antioestrogen | Short course | 3 months for recalcitrant pain |
For cysts:
- Simple cysts confirmed on ultrasound without symptoms require no treatment.
- Aspiration resolves pain and is diagnostic; fluid is usually straw-coloured or dark green.
- Large recurrent cysts: percutaneous excision with a vacuum-assisted device for definitive treatment.
For nodularity without pain:
- Triple assessment; reassurance if no discrete lesion.
- Antioestrogens (tamoxifen or ormeloxifene) control nodularity within weeks if needed.
Bailey and Love's Short Practice of Surgery, 28th Ed; Sabiston Textbook of Surgery
4. Breast Abscess
Two main categories: lactational and non-lactational (periductal/subareolar).
Causative organisms
- Lactational: Staphylococcus aureus (possibly MRSA if hospital-acquired), streptococci
- Non-lactational: Mixed aerobic and anaerobic skin flora (staphylococci, enterococci, anaerobic streptococci, Bacteroides)
A. Lactational Breast Abscess
At the cellulitic (mastitis) stage:
- Anti-staphylococcal antibiotics: cloxacillin, flucloxacillin, or erythromycin
- Encourage breastfeeding every 2 hours from both breasts, followed by complete emptying
- Breast support garment, cold compresses, analgesia
- Send milk for culture and sensitivity
When abscess forms:
- Ultrasound-guided aspiration is the preferred first-line drainage - gives excellent cosmetic result, does not hamper breastfeeding, can be done as day care.
- Incision and drainage (I&D) may cause a non-healing milk fistula.
- For abscesses >3 cm or containing >30 mL pus: insert a vacuum suction catheter under ultrasound guidance.
- Review clinically + on ultrasound on alternate days; aspirate any residual collection.
- Surgical I&D is reserved for abscesses not resolving with aspiration + antibiotics (usually multiloculated).
- Incision: radial near nipple/areola (to minimise duct damage); following Langer's lines elsewhere.
- Loculi are broken down digitally; necrotic material is curetted out.
- If drainage is problematic, dependent drainage via a counter-incision with a soft rubber drain.
Note: If antibiotics are continued without drainage, a sterile antibioma may form - a hard mass similar to carcinoma. Treat by aspiration or formal drainage.
B. Non-lactational (Subareolar/Periductal) Abscess
- Warm soaks + oral antibiotics (covering aerobes and anaerobes) at early stage
- Needle aspiration + antibiotics if abscess develops
- Surgical I&D for abscesses not responding to conservative measures
- Excision of the entire subareolar duct complex (after acute infection fully resolves, with IV antibiotic cover) for recurrent infections
- Rarely: Excision of nipple and areola for repeated recurrences
Bailey and Love's Short Practice of Surgery, 28th Ed; Pye's Surgical Handicraft; Sabiston Textbook of Surgery
Quick Summary Table
| Condition | Key Treatment |
|---|---|
| Galactocele | Single needle aspiration (usually curative); surgery rarely needed |
| Duct Ectasia | Antibiotics (co-amoxiclav + metronidazole); major duct excision for persistent/recurrent cases |
| Fibroadenosis | Reassurance + support bra; topical NSAIDs; tamoxifen/danazol/ormeloxifene for severe pain; cyst aspiration if symptomatic |
| Breast Abscess | Antibiotics ± ultrasound-guided aspiration; surgical I&D reserved for failures; subareolar duct excision for recurrent non-lactational abscess |
What will be methods and material in a thesis topic Clinicopathological study of benign breast disease
Searching PubMed
clinicopathological study benign breast disease
Searching PubMed
benign breast disease clinicopathological study methodology
Finding Sources
Reading Article
Reading File
Searching the Web
clinicopathological study benign breast disease thesis methodology materials methods FNAC histopathology
Reading Web Page
methods materials study design inclusion exclusion criteria data collection FNAC histopathology
Finding Sources
I now have all the information needed to write a thorough, thesis-standard Methods & Materials section. Here it is:
Materials and Methods
Thesis: "A Clinicopathological Study of Benign Breast Disease"
1. Study Design
A prospective observational study (hospital-based cross-sectional or cohort, depending on duration) conducted over a defined period, typically 1-2 years (e.g., January 2024 to December 2025).
Prospective design is preferred as it allows standardised data collection, planned investigations, and cytohisto-correlation from the outset.
2. Study Setting
- Department of General Surgery (and Pathology), [Name of Institution] - a tertiary care teaching hospital.
- Patients presenting to the Surgery OPD and ward with complaints referable to the breast.
3. Study Population
Inclusion Criteria
- All female patients (and male patients if presenting with breast disease) attending Surgery OPD/ward with symptoms or signs of benign breast disease
- Age: any (usually 15-65 years to capture the full ANDI spectrum)
- Patients willing to give written informed consent
- Patients in whom at least clinical + one pathological investigation (FNAC or biopsy) is available
Exclusion Criteria
- Patients with clinically obvious or confirmed malignancy at first presentation
- Patients with a prior history of breast malignancy or radiotherapy to the breast
- Patients who refuse consent or investigations
- Pregnant and lactating women may be included or excluded depending on scope (state your decision and rationale)
- Patients lost to follow-up before diagnosis is established
4. Sample Size
Calculated using standard formula for proportions:
n = Z² × p × (1-p) / d²
- Z = 1.96 (at 95% confidence interval)
- p = expected prevalence of fibroadenoma as the commonest benign lesion (~48-55% from published studies)
- d = allowable error (10%)
- Minimum sample size = approximately 100 patients (consistent with published clinicopathological studies such as Sangma et al., 2013, PMID: 23634406)
A convenience/consecutive sampling method is used - all eligible patients presenting during the study period are enrolled.
5. Data Collection
5.1 Proforma / Case Record Form
A structured proforma is designed for each patient capturing:
A. Demographic Data
- Name, age, sex, registration number
- Occupation, socioeconomic status (Modified Kuppuswamy scale)
- Residence (urban/rural)
B. History
- Chief complaint: lump/pain/nipple discharge/skin change (onset, duration, progression)
- Menstrual history: age at menarche, cycle regularity, LMP, parity, age at first childbirth
- Obstetric history: gravida, para, abortions; breastfeeding history
- Contraceptive use (oral contraceptive pills)
- Family history of breast disease or breast cancer
- Past history of breast disease, surgery, or radiation
- Habits: smoking, alcohol
C. Clinical Examination
General examination: BMI, lymph node assessment (axillary, supraclavicular, cervical)
Local breast examination (both breasts):
- Inspection: skin changes, nipple retraction, peau d'orange, erythema, visible lumps
- Palpation:
- Site (quadrant), size (in cm), shape, surface, consistency
- Margins (well/ill-defined), mobility (freely mobile / attached to skin or chest wall)
- Tenderness, transillumination
- Nipple discharge (type: serous, blood-stained, purulent, milky, coloured)
- Axillary lymph nodes
Clinical diagnosis: documented at the time of examination, before investigations
6. Investigations
6.1 Triple Assessment (Gold Standard)
All patients undergo Triple Assessment comprising:
A. Imaging
Ultrasonography (USG) of both breasts and axillae
- Equipment: High-frequency linear transducer (7.5-15 MHz)
- Assessment: number, site, size, shape, echogenicity, margins, posterior enhancement/shadowing, vascularity on Doppler, axillary nodes
- Categorised as ACR BI-RADS (Breast Imaging Reporting and Data System):
- BI-RADS 1: Normal
- BI-RADS 2: Benign
- BI-RADS 3: Probably benign - short interval follow-up
- BI-RADS 4: Suspicious - biopsy recommended
- BI-RADS 5: Highly suggestive of malignancy
Mammography
- Indicated in women >35 years or where USG is inconclusive
- Standard views: craniocaudal (CC) and mediolateral oblique (MLO)
- Reported using ACR BI-RADS classification
B. Cytological Examination - Fine Needle Aspiration Cytology (FNAC)
Procedure:
- Performed in the OPD / procedure room under aseptic precautions
- 22-24 gauge needle attached to a 10-20 mL syringe (with or without Cameco syringe holder)
- For palpable lumps: free-hand technique; for impalpable or deep lesions: ultrasound-guided FNAC
- Multiple passes through the lesion with suction; material expelled onto glass slides
- Smear preparation: air-dried (May-Grünwald-Giemsa/Diff-Quik stain) and wet-fixed (Papanicolaou stain / Haematoxylin & Eosin stain)
- For cystic lesions: fluid aspirated, centrifuged, and smears prepared from the deposit
Cytological Reporting - UK Royal College of Pathologists (RCPath) / Standardised System:
| Category | Meaning |
|---|---|
| C1 | Inadequate / unsatisfactory |
| C2 | Benign |
| C3 | Atypical - probably benign |
| C4 | Suspicious of malignancy |
| C5 | Malignant |
FNAC smears reported by a senior pathologist using standardised criteria, classifying into:
- Non-proliferative lesion
- Proliferative lesion without atypia
- Atypical proliferative lesion
- Frank carcinoma (excluded from study or noted separately)
C. Histopathological Examination (HPE)
Core Needle Biopsy (CNB):
- Performed using a 14-16 gauge automated core biopsy needle (Tru-cut or spring-loaded gun)
- USG-guided for accuracy
- Minimum 2 cores taken; placed in 10% formalin for fixation
- Indicated when FNAC is: C1 (inadequate), C3/C4 (atypical/suspicious), or clinical-cytological discordance exists
Excision Biopsy / Surgical Specimen:
- Performed for:
- Discrete lumps requiring excision (fibroadenoma >3 cm, age >30, atypical FNAC)
- Breast abscess after drainage (wall biopsy)
- Lesions on major duct excision (duct ectasia/fistula surgery)
- Specimen sent fresh or in 10% neutral buffered formalin to histopathology
Histopathological Processing:
- Grossing: Specimen measured, described (size, colour, consistency, cut surface), representative sections taken
- Processing: Tissue processor - dehydration through graded alcohols, clearing with xylene, paraffin embedding
- Sectioning: Microtome at 4-5 µm thickness
- Staining: Routine Haematoxylin & Eosin (H&E); special stains as needed (PAS, Ziehl-Neelsen for TB, etc.)
- Reporting: By a consultant histopathologist; classified per the WHO Classification of Tumours of the Breast (5th Edition, 2022)
7. Classification of Benign Breast Disease
Lesions are classified according to the Cardiff ANDI (Aberrations of Normal Development and Involution) Classification and the WHO/histopathological risk-based classification:
Histopathological Risk Classification (Page & Dupont):
- Nonproliferative (no increased risk): cysts, mild hyperplasia, duct ectasia, simple fibroadenoma, mastitis, apocrine metaplasia
- Proliferative without atypia (RR 1.5-2.0): complex fibroadenoma, papilloma, sclerosing adenosis, moderate/severe hyperplasia
- Proliferative with atypia (RR 4.5-5.0): atypical ductal hyperplasia (ADH), atypical lobular hyperplasia (ALH)
(Mulholland & Greenfield's Surgery, 7th Ed.)
Clinical disease categories studied:
- Fibroadenoma (simple and complex)
- Fibrocystic change / Fibroadenosis
- Breast cysts
- Breast abscess (lactational and non-lactational)
- Duct ectasia / Periductal mastitis
- Galactocele
- Intraductal papilloma
- Fat necrosis
- Gynaecomastia (if male patients included)
- Others (lipoma, sebaceous cyst, hamartoma)
8. Outcomes / Variables Measured
| Variable | Measurement |
|---|---|
| Clinical diagnosis | Clinician's assessment before investigations |
| USG/mammography diagnosis | Radiologist report + BI-RADS category |
| FNAC diagnosis | C1-C5 category |
| Histopathological diagnosis | WHO classification, histological type |
| Diagnostic accuracy | Clinical vs. cytological vs. histological correlation |
| Sensitivity, specificity of FNAC | Against HPE as gold standard |
| Age-wise distribution | Grouped (e.g., 10-20, 21-30, 31-40, 41-50, >50 years) |
| Symptom profile | Lump, pain, discharge, etc. |
| Hormonal/reproductive correlates | Age at menarche, parity, OCP use |
9. Ethical Considerations
- Ethical clearance obtained from the Institutional Ethics Committee (IEC) before commencement.
- Written informed consent obtained from each patient (in local language if needed).
- Patient data kept confidential; identified by registration number only in records.
- All investigations done as part of standard clinical care; no additional harm to patients.
- Study conducted in accordance with the Declaration of Helsinki (2013 revision).
10. Statistical Analysis
Software: SPSS version 26.0 / MedCalc / GraphPad Prism (state which one)
Methods:
- Descriptive statistics: Frequency and percentage for categorical variables; mean ± SD (or median with IQR for non-normal data) for continuous variables
- Inferential statistics:
- Chi-square test / Fisher's exact test: for association between categorical variables
- Student's t-test / Mann-Whitney U test: for continuous variable comparisons
- Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV): FNAC and USG vs. HPE as gold standard
- Kappa statistics: for agreement between clinical, cytological, and histological diagnoses
- Significance level: p-value <0.05 considered statistically significant
11. Operational Definitions
- Benign breast disease: Any non-malignant disorder of the breast confirmed by clinical, radiological, and/or pathological assessment
- Triple assessment: Combined evaluation using clinical examination + imaging (USG/mammography) + tissue diagnosis (FNAC/CNB)
- Clinicopathological correlation: Comparison of clinical diagnosis with pathological (cytological or histological) diagnosis
- Diagnostic accuracy: Proportion of cases where clinical/FNAC diagnosis matched the final histopathological diagnosis
Reference Publications for Methods
- Sangma MB, Panda K, Dasiah S. A clinico-pathological study on benign breast diseases. J Clin Diagn Res. 2013;7(3):503-506. [PMID: 23634406]
- Chalya PL et al. Clinicopathological pattern of benign breast diseases among female patients at a tertiary health institution in Tanzania. Tanz J Health Res. 2016;18(1).
- Bagale P et al. Clinicopathological study of benign breast diseases. Int J Health Sci Res. 2013;3(2):47-54.
Key methodological principle: Triple assessment is the gold standard, with histopathological examination (HPE) as the definitive diagnostic reference against which clinical and FNAC accuracy are measured. All cases where the clinical impression suggests benign disease but pathology shows atypia or malignancy must be documented and analysed separately, as they represent the critical diagnostic safety net of the study.
Sonomammography in benign breast disease
Reading File
Finding Sources
Finding Sources
Searching PubMed
sonomammography benign breast disease diagnosis
Searching the Web
sonomammography benign breast disease BI-RADS ultrasound mammography correlation findings
Finding Sources
Finding Sources
Searching PubMed
ultrasound mammography breast lesion diagnosis accuracy BI-RADS
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Excellent - I now have rich textbook content and images. Here is the comprehensive answer:
Sonomammography in Benign Breast Disease
Sonomammography is the combined use of ultrasonography (USG) and mammography to evaluate the breast. Together, these two modalities form the imaging component of the triple assessment - the gold standard for evaluating all breast lesions. Each modality has complementary strengths, and their combination significantly improves sensitivity and diagnostic accuracy over either modality used alone.
Combined USG + mammography sensitivity: ~85% vs. USG alone ~68-69% or mammography alone ~72% (PMC8590403)
1. Ultrasonography (Sonography)
Equipment
- High-frequency linear transducer: 7.5-15 MHz
- Real-time B-mode imaging, with Doppler capability for vascularity assessment
Why USG is Especially Valuable in Benign Breast Disease
- Primary modality in young women (<35 years) with dense breast tissue where mammography is difficult to interpret
- Best for distinguishing cystic from solid masses - this is its single most important role
- Palpable lesions can be scanned in real time, correlating directly with the patient's complaint
- No ionizing radiation - safe in pregnancy, lactation, and young women
- Guides interventional procedures (FNAC, core biopsy, cyst aspiration)
- Higher false-positive rate than mammography
Sonographic Assessment Parameters (ACR BI-RADS Ultrasound Lexicon)
Each lesion is characterised systematically across these parameters:
| Parameter | Benign Features | Suspicious Features |
|---|---|---|
| Shape | Oval, round | Irregular |
| Orientation | Parallel ("wider than tall") | Not parallel ("taller than wide") |
| Margin | Circumscribed, smooth | Indistinct, angular, microlobulated, spiculated |
| Echo pattern | Anechoic (cyst), homogeneous hypoechoic | Heterogeneous, complex |
| Posterior features | Enhancement (cyst), no effect | Shadowing |
| Boundary | Abrupt, well-defined | Echogenic halo |
| Vascularity (Doppler) | None/peripheral | Internal/hypervascular |
| Calcifications | Macrocalcifications | Microcalcifications |
Sonographic Features of Specific Benign Conditions
A. Simple Breast Cyst (BI-RADS 2)
- Anechoic (completely echo-free interior)
- Well-circumscribed, round or oval
- Posterior acoustic enhancement (increased echoes behind the cyst - pathognomonic)
- Thin, smooth wall; no solid components, no internal Doppler signal
- No further evaluation required if all simple cyst criteria are met
B. Complicated Cyst
- Not purely anechoic - contains low-level internal echoes (debris, blood, proteinaceous fluid)
- May have thin septations
- Still shows posterior acoustic enhancement
- BI-RADS 3 (short-interval follow-up); aspiration confirms diagnosis
C. Complex Cyst
- Thick wall, thick septations, solid components, or mural nodule
- Requires biopsy (BI-RADS 4) - may rarely harbour intracystic carcinoma
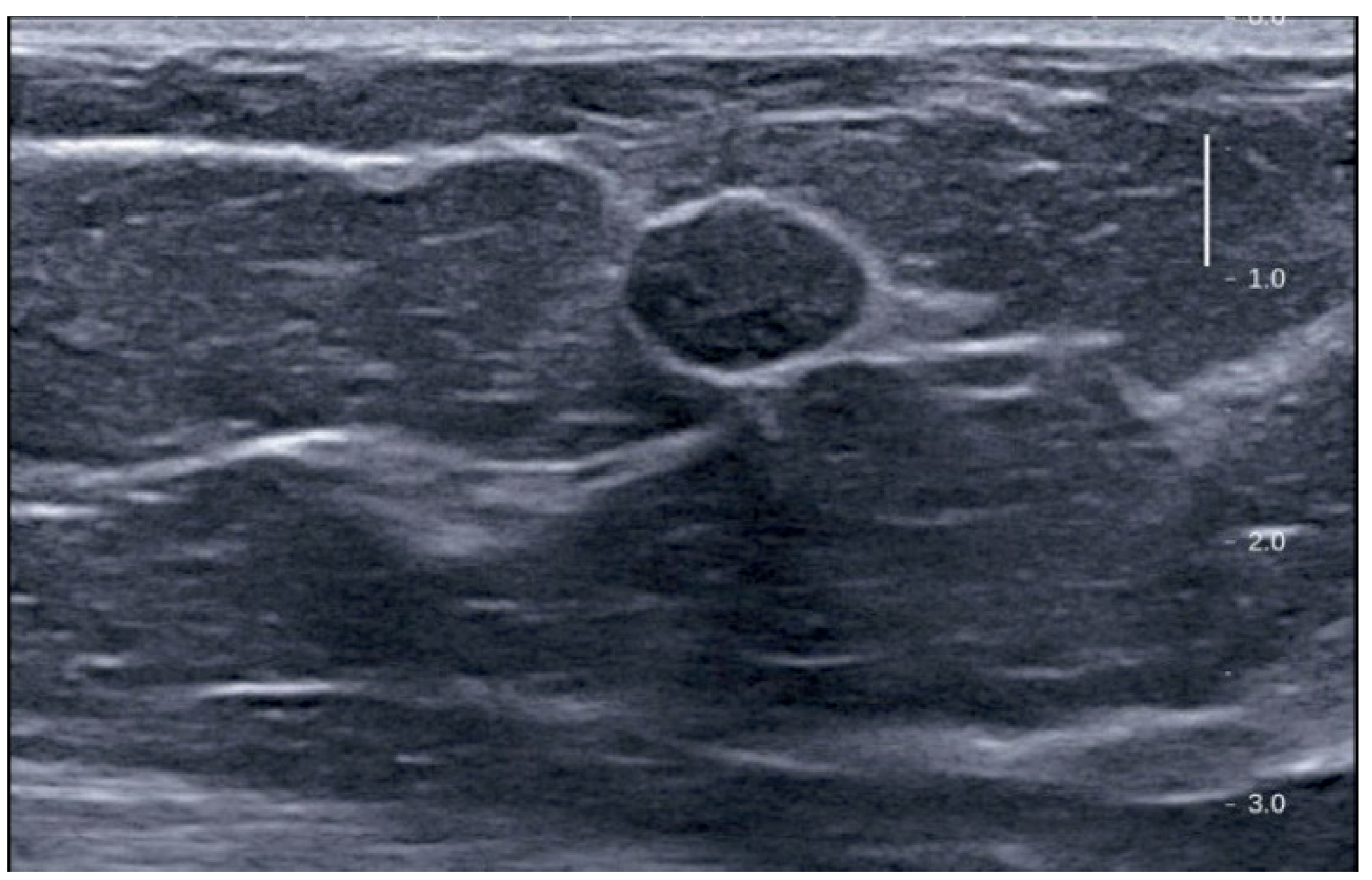
D. Fibroadenoma (BI-RADS 2-3)
- Oval, well-circumscribed, smooth margins
- Homogeneous hypoechoic or isoechoic solid mass
- Wider than tall (parallel orientation)
- 2-3 gentle lobulations may be present
- No posterior shadowing; may show mild posterior enhancement
- No internal vascularity on Doppler
- In a young woman under 25, if USG features are pathognomonic, biopsy may be deferred
E. Duct Ectasia
- Dilated major milk ducts >3 mm in diameter seen in the subareolar region
- May contain echogenic debris within the duct lumen
- Surrounding periductal echogenicity if inflammation (periductal mastitis) is present
- +/- Subareolar hypoechoic collection if abscess has formed
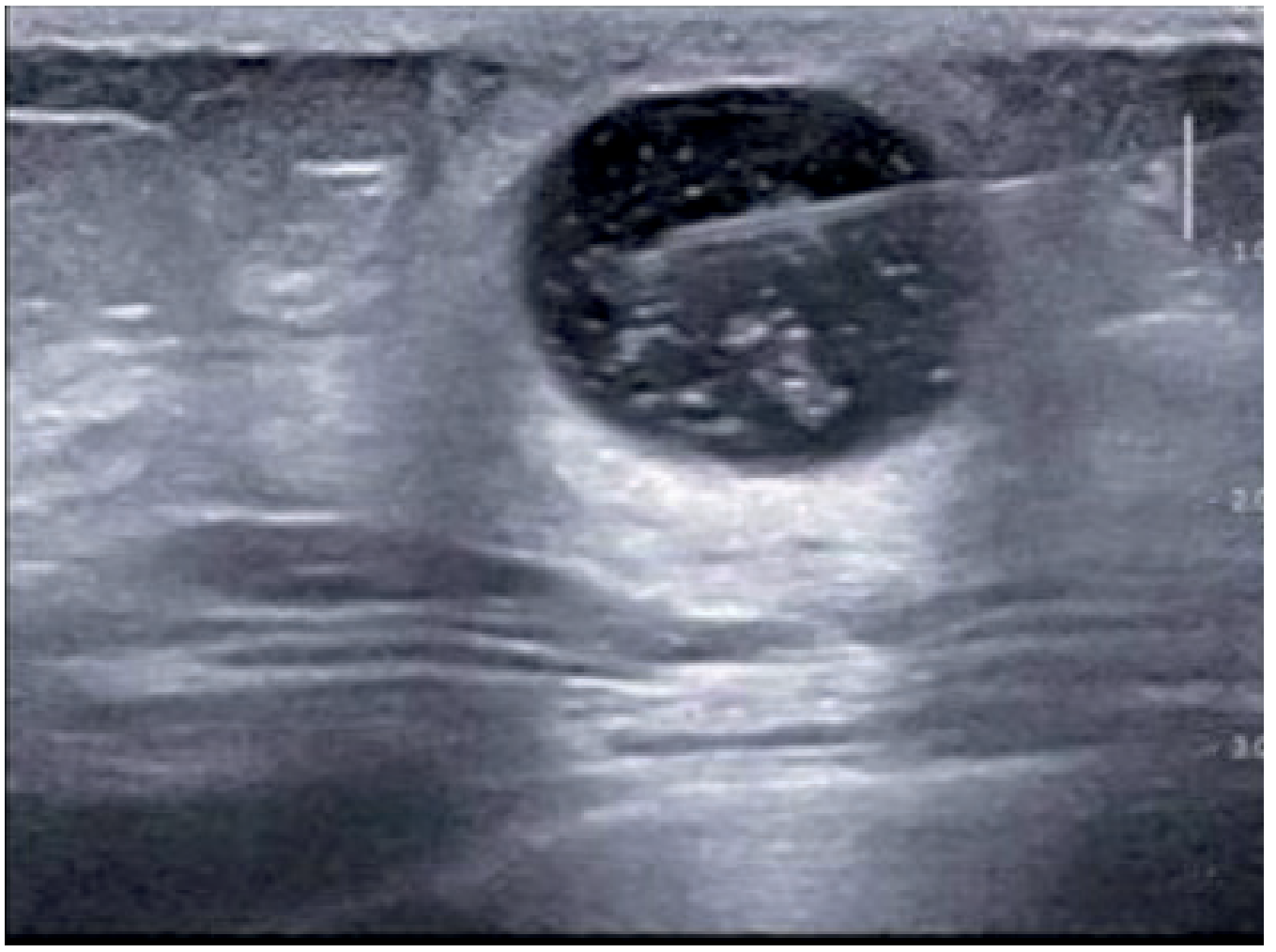
F. Breast Abscess
- Hypoechoic collection with:
- Floating internal echoes (debris) that change with posture - characteristic sign
- Thick irregular wall
- Surrounding hyperechoic tissue (cellulitis/inflammation)
- Cellulitis stage appears as an area of increased echogenicity without a discrete collection
- USG also guides aspiration and catheter placement
- Abscesses >3 cm or >30 mL: vacuum catheter drainage under USG guidance
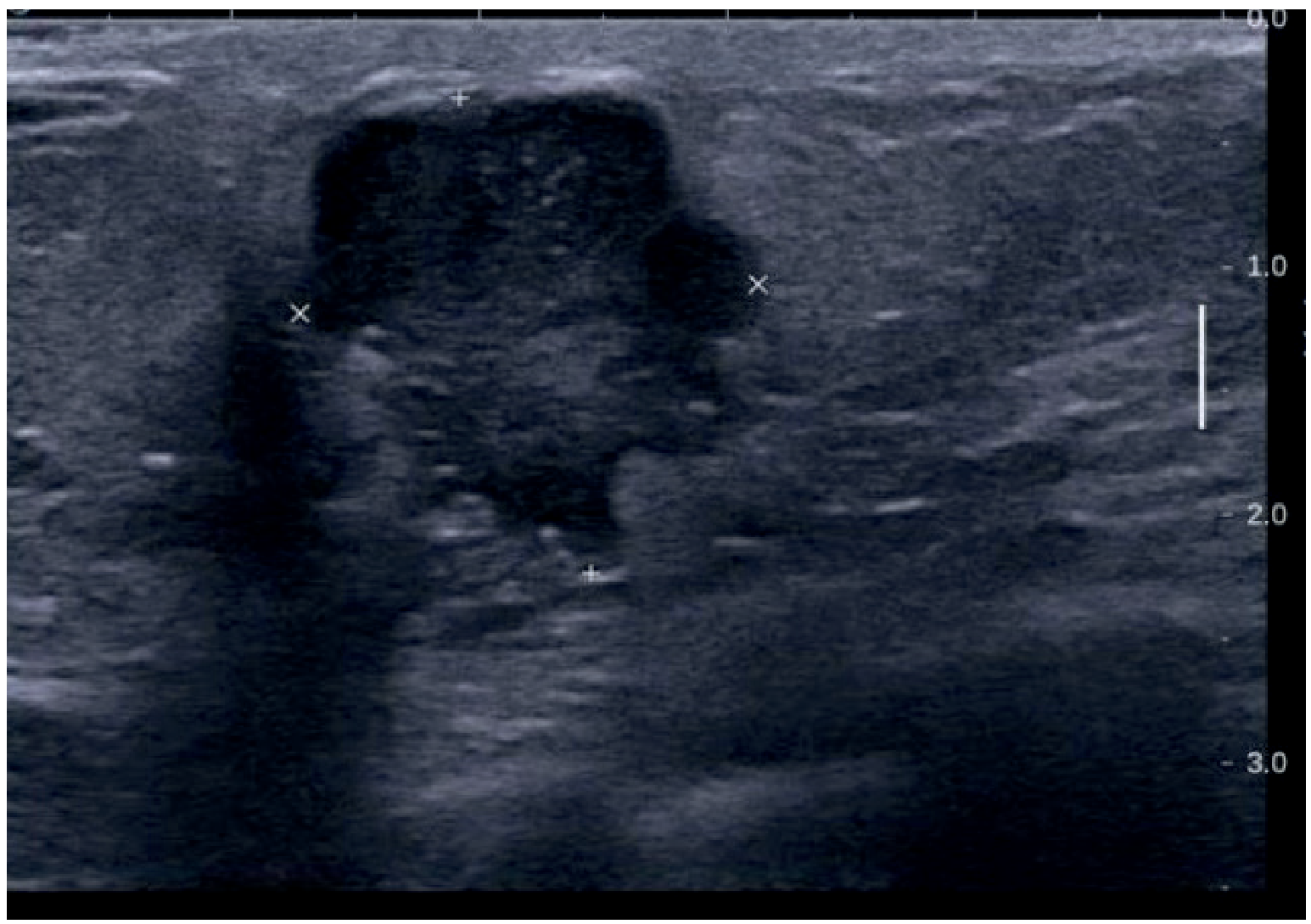
G. Galactocele
- Round, well-circumscribed mass
- Variable echogenicity (depends on fat and protein content of milk)
- May be anechoic (early/fluid-filled) to hyperechoic (inspissated milk)
- Located central/subareolar
H. Fibrocystic Changes / Fibroadenosis
- Diffuse heterogeneous echotexture
- Multiple small cysts scattered throughout breast parenchyma
- Increased fibroglandular density
- No dominant solid mass; if present, requires separate assessment
I. Intraductal Papilloma
- Small hypoechoic mass within a dilated duct
- Duct dilatation with or without an intraluminal lesion
- Colour Doppler may show internal vascularity
- Requires biopsy
Indications for Breast Ultrasonography (Berek & Novak's Gynecology)
- Palpable abnormality
- Ambiguous or equivocal mammographic findings
- Mass in women <30 years, lactating, or pregnant
- Guidance for interventional procedures (FNAC, core biopsy, aspiration, drainage)
- Possible adjunct screening in women with dense breasts (BI-RADS density C or D)
- Evaluation of silicone implant integrity
Limitations of USG
- Cannot reliably detect microcalcifications (mammography is superior)
- Not useful in fatty breasts
- Operator-dependent (highly skilled ultrasonographer required)
- Higher false-positive rate than mammography
2. Mammography
Types
| Type | Indication |
|---|---|
| Screening mammography | Asymptomatic women ≥40 years (2 views per breast) |
| Diagnostic mammography | Symptomatic women (lump, pain, discharge), recall after BI-RADS 0 |
Standard Views
- Craniocaudal (CC) - top-down view
- Mediolateral oblique (MLO) - angled lateral view
- Additional views: spot compression, magnification, tangential views for problem-solving
Breast Density (BI-RADS Composition Categories)
| Category | Description |
|---|---|
| A | Almost entirely fatty |
| B | Scattered fibroglandular density |
| C | Heterogeneously dense - may obscure small masses |
| D | Extremely dense - lowers sensitivity |
- Mammography sensitivity: ~80% overall; lower (~48-60%) in dense (C/D) breasts
- Mammography specificity: 80-95%
Mammographic Features of Benign Lesions
| Condition | Mammographic Appearance |
|---|---|
| Simple cyst | Oval/round, smooth, well-circumscribed, isodense mass; "halo sign" (thin lucent rim); not distinguishable from solid mass - needs USG correlation |
| Fibroadenoma | Oval, smooth, well-circumscribed, isodense; may have "popcorn calcifications" (coarse dystrophic calcification in older lesions) |
| Fibrocystic change | Diffuse or focal radiodense tissue; multiple bilateral ill-defined nodular densities; calcifications (round/punctate/eggshell) |
| Duct ectasia | Tubular densities in subareolar region; "rod-like" or "plasma cell" calcifications parallel to ducts (secretory calcifications) |
| Fat necrosis | Oil cyst (lucent round lesion with thin capsule); eggshell calcifications |
| Lipoma | Radiolucent encapsulated lesion |
| Galactocele | Well-circumscribed mass; may show fat-fluid level (pathognomonic on horizontal beam) |
| Skin calcifications | Lucent centres, located in the skin |
Mammographic Signs Suggesting Malignancy (for comparison/exclusion)
- Spiculated mass with irregular margins
- Pleomorphic, fine linear, or branching microcalcifications in segmental/linear distribution
- Architectural distortion
- Asymmetric density
- Skin thickening or nipple retraction
3. The BI-RADS Classification System
Developed by the American College of Radiology (ACR) for standardised reporting of both mammography and ultrasound. Applies to both modalities.
| BI-RADS Category | Assessment | Probability of Malignancy | Action |
|---|---|---|---|
| 0 | Incomplete | N/A | Additional imaging needed / compare priors |
| 1 | Negative | ~0% | Routine annual screening |
| 2 | Benign finding | ~0% | Routine annual screening |
| 3 | Probably benign | >0% but ≤2% | Short-interval follow-up (6 months) |
| 4a | Low suspicion | >2% to ≤10% | Biopsy should be considered |
| 4b | Intermediate suspicion | >10% to ≤50% | Biopsy |
| 4c | Moderate concern | >50% to <95% | Biopsy |
| 5 | Highly suggestive of malignancy | ≥95% | Biopsy / surgical treatment |
| 6 | Known biopsy-proven malignancy | N/A | Surgical management |
Key rule: When both USG and mammography are performed, the final BI-RADS category is the most suspicious finding from either modality. Biopsy/tissue diagnosis is mandatory for BI-RADS 4 or 5.
4. Role of Sonomammography (Combined USG + Mammography) - Practical Summary
| Scenario | Preferred Modality | Reason |
|---|---|---|
| Age <35 years | USG first | Dense breasts; mammography less sensitive |
| Age >35-40 years with lump | Both | Mammography for overview; USG for characterisation |
| Cyst vs. solid distinction | USG | Definitive differentiation |
| Microcalcifications | Mammography | USG cannot reliably detect these |
| Lactating/pregnant women | USG only | No radiation; mammography avoided |
| Equivocal mammogram | Add USG | Resolves most ambiguous findings |
| Breast abscess | USG | Confirms collection, guides drainage |
| Dense breast (BI-RADS C/D) | USG as adjunct | Increases cancer detection rate |
| Screening asymptomatic women | Mammography | USG not standard for population screening |
5. Other Advanced Imaging (Adjuncts)
- MRI: Highest sensitivity (>90%) for breast pathology; reserved for high-risk screening (>20% lifetime risk), implant evaluation, equivocal USG/mammography, neoadjuvant chemotherapy response monitoring. Not routine for benign disease.
- Digital breast tomosynthesis (DBT/3D mammography): Reduces false-positive recall rates; improves detection of architectural distortion; cancer detection rate improved from 1.2 to 4.6 per 1,000 over 2D mammography alone.
- Ductography (galactography): Contrast injected into a duct; primary indication is blood-stained nipple discharge to localise intraductal papilloma or duct ectasia.
- Sonoelastography: Assesses tissue stiffness; malignant lesions are harder (stiffer) than benign; useful adjunct but not routine.
Summary: Sonomammography in Specific Benign Breast Diseases
| Disease | USG Findings | Mammography Findings | BI-RADS |
|---|---|---|---|
| Simple cyst | Anechoic, posterior enhancement, no wall nodule | Round smooth well-circumscribed density | 2 |
| Complicated cyst | Low-level echoes internally, posterior enhancement | Similar to simple cyst | 3 |
| Fibroadenoma | Oval, well-circumscribed, homogeneous hypoechoic, parallel | Oval circumscribed mass ± popcorn calcification | 2-3 |
| Fibroadenosis | Heterogeneous, multiple small cysts, no dominant mass | Diffuse nodular densities, bilateral | 2 |
| Duct ectasia | Dilated ducts >3mm, periductal echogenicity | Tubular densities, rod-like calcifications | 2 |
| Breast abscess | Hypoechoic collection, debris changing with posture, hyperechoic surround | May show focal density; limited role | 4 (if uncertain) |
| Galactocele | Variable echo, subareolar, round | Well-circumscribed mass; fat-fluid level | 2-3 |
| Intraductal papilloma | Hypoechoic mass in dilated duct | Focal density subareolar | 3-4 |
| Fat necrosis | Variable - may mimic carcinoma | Oil cyst, eggshell calcification | 2-4 |
| Sclerosing adenosis | Poorly defined hypoechoic area | Spiculated mass / architectural distortion - can mimic carcinoma | 4 (needs biopsy) |
Bailey and Love's Short Practice of Surgery, 28th Ed; Berek & Novak's Gynecology; Schwartz's Principles of Surgery, 11th Ed; Fischer's Mastery of Surgery, 8th Ed
This is a shared conversation. Sign in to Orris to start your own chat.