Pathophysiology, histology and classification of HCM
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypertrophic cardiomyopathy"[MeSH Terms] AND classification
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive, rich content from multiple authoritative textbooks. Let me compile the full answer.
Hypertrophic Cardiomyopathy (HCM): Pathophysiology, Histology, and Classification
Definition
HCM is defined as unexplained left ventricular (LV) hypertrophy in the absence of abnormal loading conditions (severe hypertension, valve disease, congenital heart defects) sufficient to account for the degree of hypertrophy. It is characterized by a thick-walled, heavy, hypercontractile heart with preserved (or supranormal) systolic function but impaired diastolic relaxation - the opposite of dilated cardiomyopathy.
- Prevalence: ~1:500 in echocardiographic studies; clinically evident in ~1:2500
- Slight male predominance (60-65%)
- Can manifest at any age, most commonly during the postpubertal growth spurt
Classification
1. By Etiology (Fuster & Hurst, 15th Ed.)
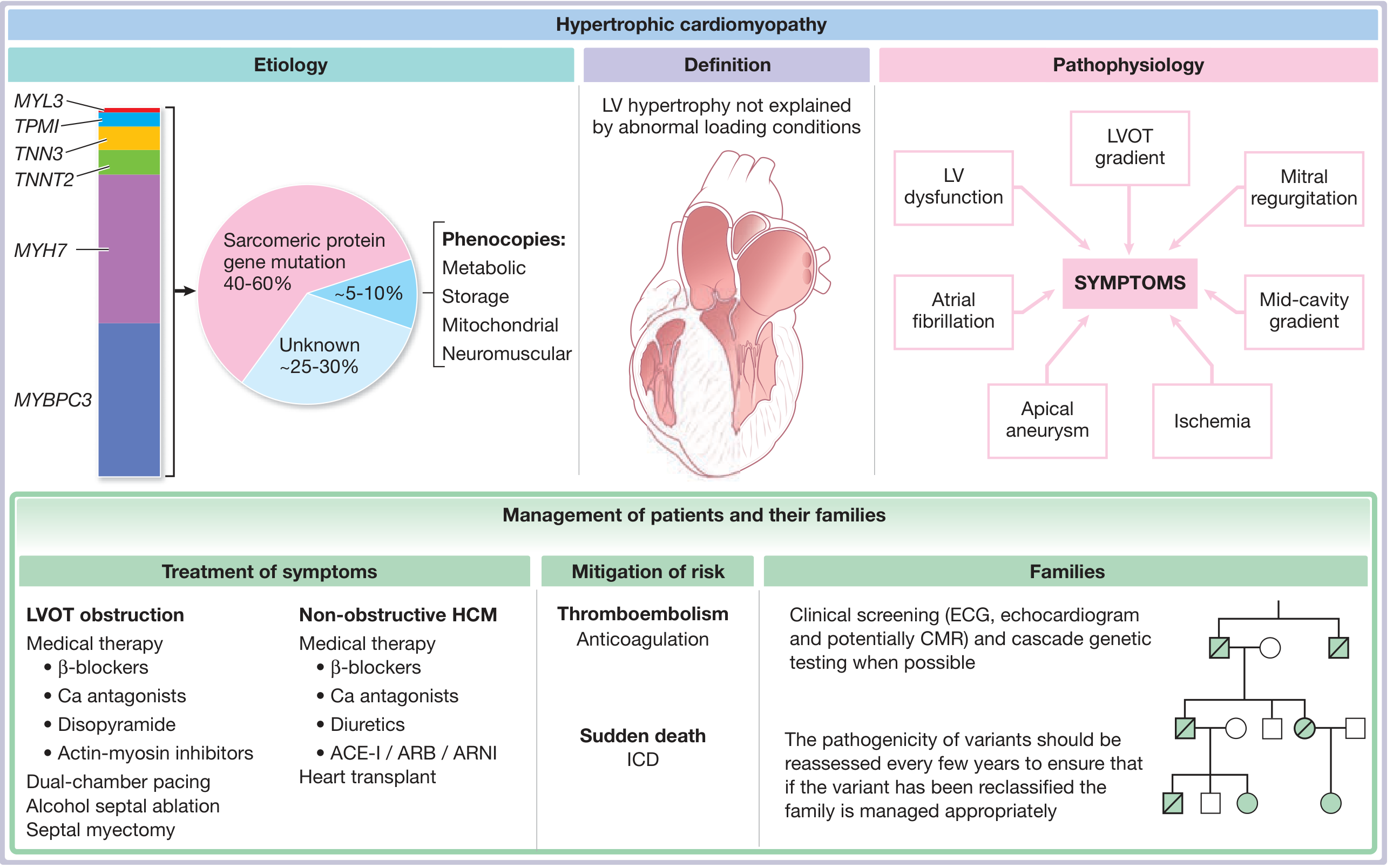
Fig. 42 Fuster & Hurst: HCM etiology, pathophysiology, and management overview
| Category | Proportion | Notes |
|---|---|---|
| Sarcomeric protein gene mutations (familial/genetic) | 40-60% | Autosomal dominant, incomplete penetrance |
| Phenocopies | 5-10% | Same phenotype, different etiology |
| Unknown/sporadic | ~25-30% | Genotype-negative |
Phenocopies include:
- Metabolic/storage disorders: Anderson-Fabry disease, Danon disease, glycogen storage diseases (Pompe)
- Mitochondrial disorders (respiratory chain defects)
- Neuromuscular disorders: Friedreich ataxia, neurofibromatosis
- Chromosome abnormalities
- Genetic syndromes: Noonan syndrome, LEOPARD syndrome, cardio-facial-cutaneous syndromes (RASopathies)
2. By LVOT Obstruction (Hemodynamic Classification)
| Type | Description |
|---|---|
| Obstructive HCM | LVOT gradient ≥30 mmHg at rest (most important subtype) |
| Latent/Provocable HCM | Gradient ≥30 mmHg only with provocation (Valsalva, exercise); absent at rest |
| Non-obstructive HCM | No significant gradient at rest or with provocation |
| Midcavity obstructive HCM | Gradient at midventricular level (~10% of cases); hypertrophied septum contacts lateral wall; associated with apical aneurysm in ~1/3 of cases |
About 50% of all HCM patients develop LVOT obstruction at rest or with exercise.
3. By Morphological Pattern (Goldman-Cecil)
| Pattern | Notes |
|---|---|
| Asymmetric septal hypertrophy (ASH) | Classic form; preferential anteroseptal wall involvement; >90% of cases |
| Concentric hypertrophy | ~10% of cases; uniform wall thickening |
| Apical HCM | Hypertrophy confined to the LV apex; "ace-of-spades" appearance on ventriculography |
| Midventricular HCM | Hypertrophy at mid-cavity; prone to obstruction and apical aneurysm |
| Basal septal HCM | Older individuals; sigmoid-shaped septum; often sporadic, genotype-negative |
| Right ventricular involvement | RV free wall and papillary muscles can be affected |
Genetics and Molecular Basis
HCM is the most common inherited cardiac disease with autosomal dominant transmission and variable expressivity. More than 1400 pathogenic mutations have been identified across sarcomeric and non-sarcomeric genes:
| Gene | Protein | Proportion of genotype+ cases |
|---|---|---|
| MYH7 | β-Myosin heavy chain | ~35-40% |
| MYBPC3 | Myosin binding protein C | ~35-40% |
| TNNT2 | Troponin T | ~5% |
| TNNI3 | Troponin I | ~5% |
| TPM1 | α-Tropomyosin | ~5% |
| MYL2, MYL3 | Myosin light chains | <5% each |
| ACTC1 | Cardiac actin | <1% |
MYH7 and MYBPC3 together account for 75-80% of cases where a mutation is identified. A key molecular principle: these are gain-of-function mutations (enhanced myofilament function), in contrast to DCM where the same genes carry loss-of-function mutations. Patients with MYH7 mutations tend to have worse outcomes, particularly advanced heart failure compared to MYBPC3 variants. - Robbins Basic Pathology, p. 373; Fuster & Hurst, p. 1346
Pathophysiology
The pathophysiology is multifactorial and consists of five interrelated mechanisms:
1. Sarcomeric Dysfunction and Energy Imbalance
Gain-of-function sarcomere mutations cause hypercontractility and inefficient ATP utilization. The sarcomere produces excess force but at the cost of excessive energy consumption, creating a chronic negative energy balance. Compensatory hypertrophy follows but perpetuates abnormal cellular metabolism. - Goldman-Cecil, p. 502
2. Diastolic Dysfunction (Primary Abnormality)
This is the most universal functional consequence of HCM. Multiple mechanisms contribute:
- Impaired ventricular relaxation: non-uniformity of contraction/relaxation, delayed myosin-actin detachment from abnormal intracellular calcium reuptake, disruption of the myosin interacting heads motif
- Increased chamber stiffness: from myocardial fibrosis and hypertrophy
- Supply-demand mismatch: ischemia causes delayed relaxation
- Result: elevated LV filling pressures → increased pulmonary venous pressure → exertional dyspnea
A minority (~5%) develop a restrictive phenotype with biatrial dilation, atrial fibrillation, and pulmonary hypertension. A separate 3-8% undergo "burnt-out" or "end-stage" HCM with LV cavity enlargement, wall thinning, loss of LVOT gradient, and extensive fibrosis - this carries the worst prognosis. - Fuster & Hurst, p. 1347
3. LVOT Obstruction (in ~50% of patients)
Dynamic outflow obstruction arises from two mechanisms working together:
- Systolic anterior motion (SAM) of the anterior mitral leaflet: the leaflet is dragged into the outflow tract during systole by the Venturi effect and/or drag forces from high-velocity LVOT flow. The leaflet contacts the hypertrophied septum, creating obstruction and reducing effective orifice area
- Asymmetric septal hypertrophy (ASH): the bulging septum narrows the LVOT
This obstruction is dynamic - it worsens with:
- Reduced preload (dehydration, standing, Valsalva, vasodilators)
- Increased contractility (exercise, catecholamines)
- Reduced afterload (vasodilators, alcohol)
- Ingestion of food or large meals
The resulting LVOT gradient can reach 100 mmHg or more in severe cases.
4. Mitral Regurgitation
SAM-related obstruction prevents complete coaptation of the mitral valve leaflets, causing functional mitral regurgitation (MR). The severity of MR fluctuates with the LVOT gradient. In some patients, additional intrinsic mitral valve pathology exists (leaflet prolapse, elongation, abnormal chordal insertions).
5. Myocardial Ischemia
Ischemia occurs even without epicardial coronary artery disease due to:
- Increased oxygen demand from hypertrophy and elevated filling pressures
- Abnormal intramural coronary arteries (medial and intimal hyperplasia, reduced luminal diameter, impaired vasodilation)
- LVOT obstruction raises LV systolic pressure further, compressing intramyocardial vessels
- High intracavity systolic pressure in midcavity obstruction → apical aneurysm formation from regional ischemia/scarring
Ischemia manifests as exertional chest pain, and also contributes to diastolic dysfunction via impaired relaxation.
6. Arrhythmia Substrate
- Atrial fibrillation: affects ~20-25% of HCM patients over time; elevated filling pressures → LA dilation → AF. Carries high thromboembolic risk
- Ventricular arrhythmias: myocyte disarray and interstitial fibrosis create re-entry circuits → VF → sudden cardiac death (SCD)
HCM is the #1 cause of sudden cardiac death in athletes under 35 years of age, responsible for nearly one-third of such deaths. - Robbins Basic Pathology, p. 374
Gross Pathology (Morphology)
- Massive myocardial hypertrophy without ventricular dilation
- 90% of cases: asymmetric septal hypertrophy (septal:free wall ratio >1.5)
- 10% of cases: concentric hypertrophy
- LV cavity on longitudinal section: "banana-shaped" due to septal compression
- Fibrous endocardial plaque on the ventricular septum where the anterior mitral leaflet makes repeated systolic contact
- Mitral leaflets: consistently elongated; anterior displacement and hypertrophy of papillary muscles; abnormal chordal insertions
- Left (and sometimes right) atrium dilated in advanced disease
- Epicardial coronary arteries usually normal; may follow an intramural course and be compressed during systole
- Robbins Basic Pathology, p. 373-374; Goldman-Cecil, p. 502
Histology
Three hallmark histological features define HCM:
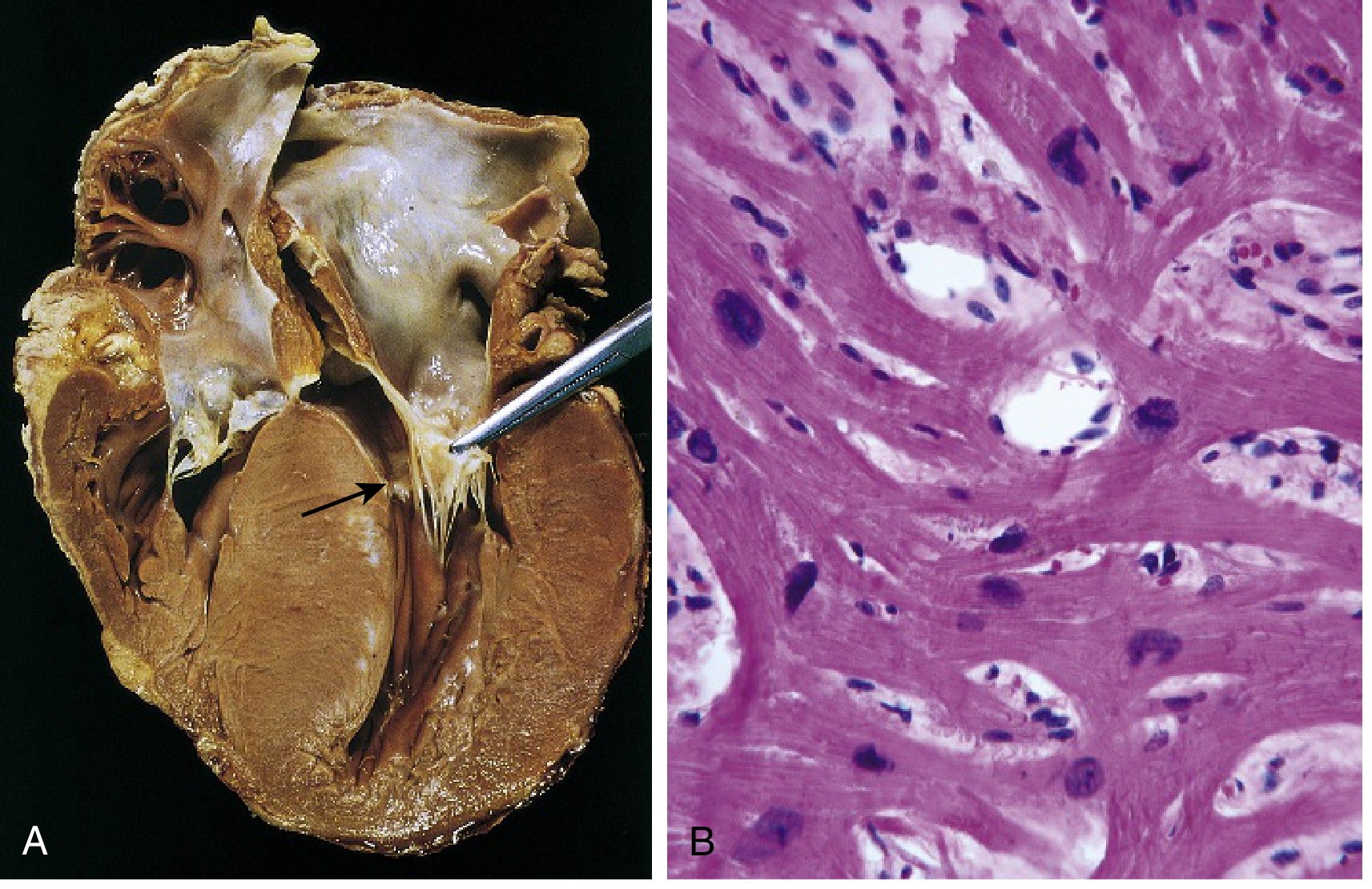
FIG. 9.27 (Robbins): (A) Asymmetric septal hypertrophy producing "banana-shaped" LV lumen with fibrous endocardial plaque (arrow). (B) Histology showing myocyte disarray, extreme hypertrophy, branching, and interstitial fibrosis.
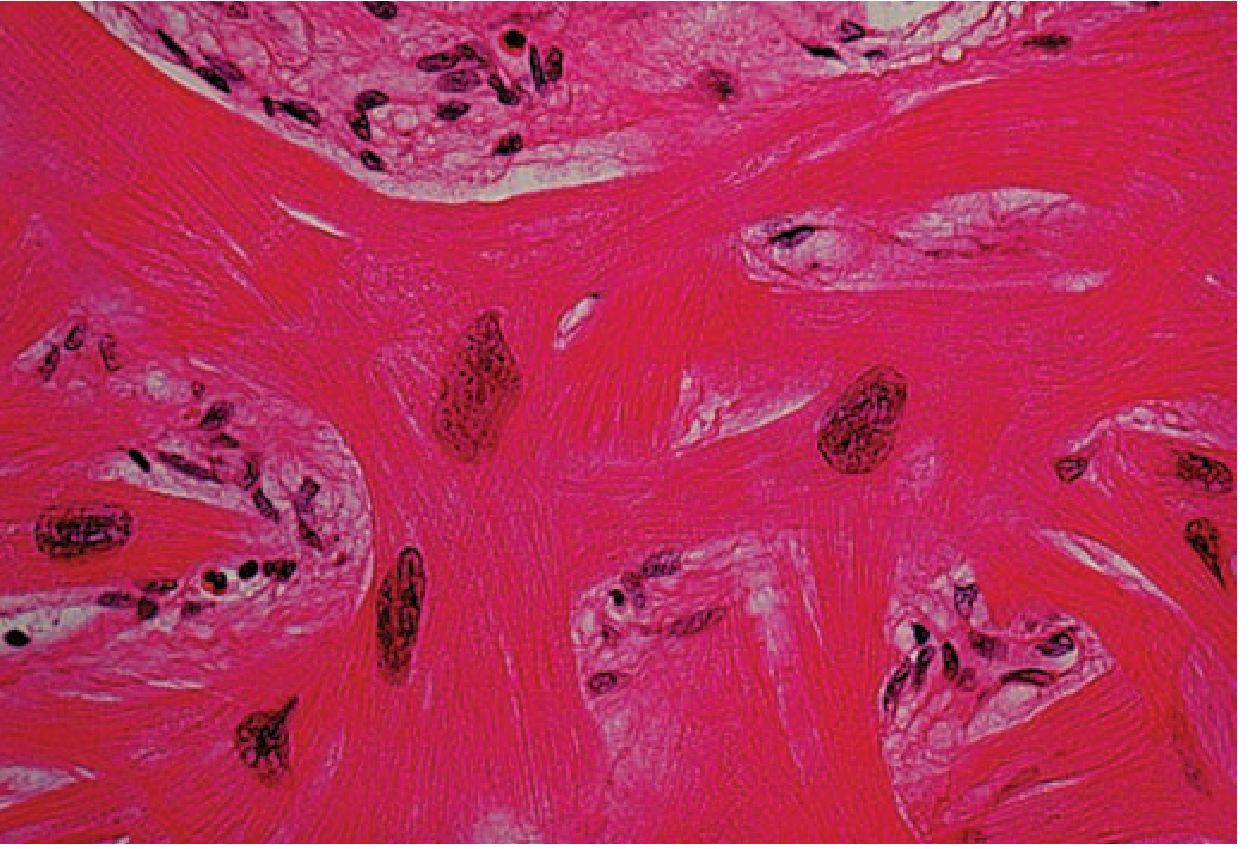
Fig. 42-4 (Fuster & Hurst): Myocyte disarray - adjacent cardiomyocytes running obliquely and perpendicularly to each other, a pathognomonic feature of HCM.
1. Myocyte Hypertrophy
- Extreme enlargement of individual cardiomyocytes
- Bizarrely shaped, enlarged nuclei ("box-car" or "owl-eye" nuclei)
- Abnormal intracellular myofibrillar architecture (myofibrillar disarray within individual cells)
2. Myocyte/Myofiber Disarray (Pathognomonic)
- Architectural disorganization of the myocardium: adjacent myocytes run obliquely or perpendicular to each other instead of in the normal parallel arrangement
- Affects >20% of myocardium (vs. <5% in normal hearts or other conditions)
- Found most prominently in the interventricular septum
- The myofibrillar architecture within each myocyte is also disorganized
- This disarray is the arrhythmogenic substrate for re-entrant ventricular arrhythmias
3. Interstitial and Replacement Fibrosis
- Increased interstitial collagen deposition around myocytes (interstitial fibrosis)
- Focal areas of replacement fibrosis (scar)
- Contributes to diastolic stiffness and arrhythmia substrate
- Progressive fibrosis correlates with symptom severity and SCD risk
4. Dysplastic Intramural Arterioles
- Medial and intimal hyperplasia of small intramyocardial coronary arteries
- Reduces vessel luminal diameter and impairs vasodilation
- Key substrate for microvascular ischemia even with normal epicardial coronaries
- Robbins Basic Pathology, p. 374; Fuster & Hurst, p. 1411; Goldman-Cecil, p. 502
Summary Table
| Feature | HCM |
|---|---|
| Inheritance | Autosomal dominant, incomplete penetrance |
| Most common genes | MYH7, MYBPC3 (75-80% of genotype+ cases) |
| Mutation type | Gain-of-function sarcomeric mutations |
| Key gross feature | Asymmetric septal hypertrophy, "banana" LV cavity |
| Hallmark histology | Myocyte disarray + hypertrophy + interstitial fibrosis |
| Primary physiology | Diastolic dysfunction |
| Obstructive mechanism | SAM of anterior mitral leaflet + ASH |
| Ischemia mechanism | Microvascular disease + supply-demand mismatch |
| SCD risk | Leading cause in athletes <35 years |
Sources: Robbins & Kumar Basic Pathology (9780323790185) | Goldman-Cecil Medicine (9780323930345) | Fuster & Hurst's The Heart, 15th Ed. (9781264257560)
This is a shared conversation. Sign in to Orris to start your own chat.