Sinusitis
Reading File
Finding Sources
Searching PubMed
sinusitis diagnosis management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from Harrison's 22E, Cummings Otolaryngology, Scott-Brown's, Robbins, and K.J. Lee's. Let me now compile the full, detailed response.
Sinusitis
Sinusitis (rhinosinusitis) is inflammation of the paranasal sinuses. It is one of the most common diagnoses in outpatient medicine and a leading driver of unnecessary antibiotic prescribing.
Definition and Classification
Sinus symptoms are classified by duration:
| Category | Duration |
|---|---|
| Acute | < 4 weeks |
| Subacute | 4-12 weeks |
| Chronic | ≥ 12 weeks |
| Recurrent acute | ≥ 4 episodes/year without symptoms between episodes |
- Harrison's Principles of Internal Medicine 22E, p.299
Etiology and Pathophysiology
Acute sinusitis is caused primarily by respiratory viruses. Although bacteria cause fewer than 2% of sinusitis episodes (most often S. pneumoniae, H. influenzae, or M. catarrhalis), antibiotics are prescribed at over 70% of office visits. According to guideline criteria, probably no more than 20-50% of adults meet antibiotic prescribing criteria.
Pathophysiologically, most cases are preceded by rhinitis, which produces mucosal edema that impairs sinus drainage. Maxillary sinusitis can also arise by extension of a periapical dental infection through the bony sinus floor. Outflow obstruction occurs most often in the frontal and anterior ethmoid sinuses and may cause mucus accumulation (mucocele).
Chronic sinusitis is typically polymicrobial, largely composed of normal oral microbes. Staphylococcus aureus, anaerobes, and fungi become more prominent. Fungi may cause severe chronic sinusitis especially in diabetic patients (e.g., mucormycosis). Sinusitis also occurs as a component of Kartagener syndrome (bronchiectasis + situs inversus + sinusitis) due to inherited ciliary defects.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p.803-805
- Harrison's 22E, p.299
Clinical Features
Symptoms:
- Purulent nasal discharge
- Facial congestion, fullness, or pressure/pain
- Postnasal drip, halitosis, cough, fatigue
- Fever, hyposmia or anosmia
- Ear pressure/fullness
- Maxillary toothache
Risk factors: Age 45-65, smoking, asthma, air travel, allergies.
Exam findings: Direct rhinoscopy shows excess mucus or purulence. Tenderness over maxillary sinuses; in severe cases, erythema and swelling. Sinus transillumination is not accurate for diagnosis.
- Harrison's 22E, p.299
Differential Diagnosis
- Common cold / allergic rhinitis
- Vasomotor rhinitis
- Rhinitis medicamentosa (from topical decongestants)
- Drug-induced rhinitis (aspirin, NSAIDs, beta-blockers)
- Granulomatosis with polyangiitis
- CSF leak
- Dental pathology / temporomandibular disorder
- Headache syndromes
- Invasive fungal infection (especially in immunocompromised)
- Foreign body (especially in children)
Antibiotic Prescribing Criteria
Antibiotics should only be prescribed when symptoms meet one of these criteria (Harrison's Table 37-2):
| Indication | Definition |
|---|---|
| Persistent | Symptoms lasting ≥ 10 days |
| Severe | Fever > 102°F AND purulent nasal discharge or facial pain for ≥ 3-4 consecutive days |
| Worsening | New fever, headache, or increased nasal discharge following an upper respiratory infection that lasted 5-6 days and was initially improving ("double sickening") |
- Harrison's 22E, p.299-300
Treatment
Symptomatic (all patients)
- Intranasal decongestants: oxymetazoline, 2 sprays each nostril BID, for no more than 5 days
- Oral decongestants: pseudoephedrine 120 mg extended-release during the day
- Analgesics/antipyretics: acetaminophen or ibuprofen
- Nasal saline spray or washes
- Intranasal glucocorticoids - particularly helpful with an allergic component
Antibiotic Therapy (when criteria met)
First line: Amoxicillin/clavulanate 875/125 mg PO BID x 7 days. Amoxicillin 875 mg PO BID x 7 days is an acceptable alternative.
Penicillin allergy (mild): Cefuroxime
Penicillin allergy (severe): Doxycycline
Not recommended: Macrolides (high rates of macrolide-resistant S. pneumoniae)
No improvement after 3-5 days on first-line antibiotic:
- Amoxicillin/clavulanate 2000/125 mg PO BID x 7 days, OR
- Levofloxacin (note: fluoroquinolones carry risks of dysglycemia, neuropathy, tendon and aortic rupture)
Still no improvement after second-line antibiotic: Refer to otorhinolaryngology and/or obtain non-contrast CT.
Chronic Sinusitis
-
Medical treatment with antibiotics for 4-6 weeks
-
Nasal saline irrigation (recent meta-analysis supports budesonide nasal irrigation for chronic rhinosinusitis)
-
Adenoidectomy may help in younger children
-
Endoscopic sinus surgery (FESS) for failed medical management, targeting involved sinuses
-
Harrison's 22E, p.299-300
-
K.J. Lee's Essential Otolaryngology, p.1015
Complicated Sinusitis
Frontal and ethmoidal sinusitis usually responds to decongestants and antibiotics. Failure to respond or evidence of spread beyond the sinus requires drainage. Failure to recognize extra-sinus spread can lead to orbital abscess and intracranial infection - this should be identified within 24 hours of the first signs.
If infection spreads beyond the frontal sinus (bony wall infection + venous thrombosis through bone), prolonged antibiotics are required - 8-12 weeks. A patient may show dramatic initial improvement with a 2-week course, creating a false sense of security - this is a pitfall; stopping short risks chronic osteomyelitis or secondary intracranial sepsis.
Complications include:
- Orbital cellulitis and abscess
- Osteomyelitis
- Meningitis
- Intracranial abscesses
- Cavernous sinus thrombosis
- Septic thrombophlebitis of dural venous sinuses
Red flags requiring urgent reassessment: confusion, unilateral weakness, proptosis, limited ocular movements, acute vision changes.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 1, p.495
- Harrison's 22E, p.299
Fungal Sinusitis
Classification
Invasive:
- Acute invasive fungal sinusitis (AIFS) - occurs in immunocompromised patients; rapidly progressive and potentially fatal. CT may show subtle bone erosion; early finding is severe unilateral nasal mucosal inflammatory changes. MRI is superior (sensitivity 85% vs CT 63%) - look for "black turbinate sign" (non-enhancing devitalized tissue on post-contrast MRI), obliteration of periorbital fat, leptomeningeal enhancement.
- Chronic invasive fungal sinusitis (CIFS) - immunocompetent or mildly immunocompromised (e.g., diabetics). Homogeneous opacification without focal hyperdensities; limited unilateral bony erosion.
- Chronic granulomatous invasive fungal sinusitis (CGIFS) - seen mainly in Africa/South Asia; usually Aspergillus spp; immunocompetent individuals.
Non-invasive:
- Allergic fungal sinusitis (AFS) - immunocompetent atopic patients; "allergic mucin" visible on endoscopy. CT: bilateral multisinusal opacification with sinus expansion, bony erosion, and intra-sinus high attenuation (calcium, heavy metals, inspissated secretions).
Causative Organisms
- Mucorales fungi (mucormycosis) - especially in uncontrolled diabetes
- Aspergillus spp. (A. flavus has high propensity for acute sinus infection; cavernous sinus thrombosis involving CN III, IV, V, VI)
Management of AIFS
- This is a diagnostic and therapeutic emergency
- Nasal endoscopy + biopsy (frozen section to accelerate treatment)
- Gadolinium-enhanced MRI is the preferred imaging modality
- Wide debridement to viable tissue
- IV antifungal agents
- Surgical debridement often required
- Treat even without histologic confirmation of invasion if clinical scenario + fungal elements on silver stain or culture are consistent
CT and MRI of Aspergillus sinusitis (Cummings Otolaryngology):
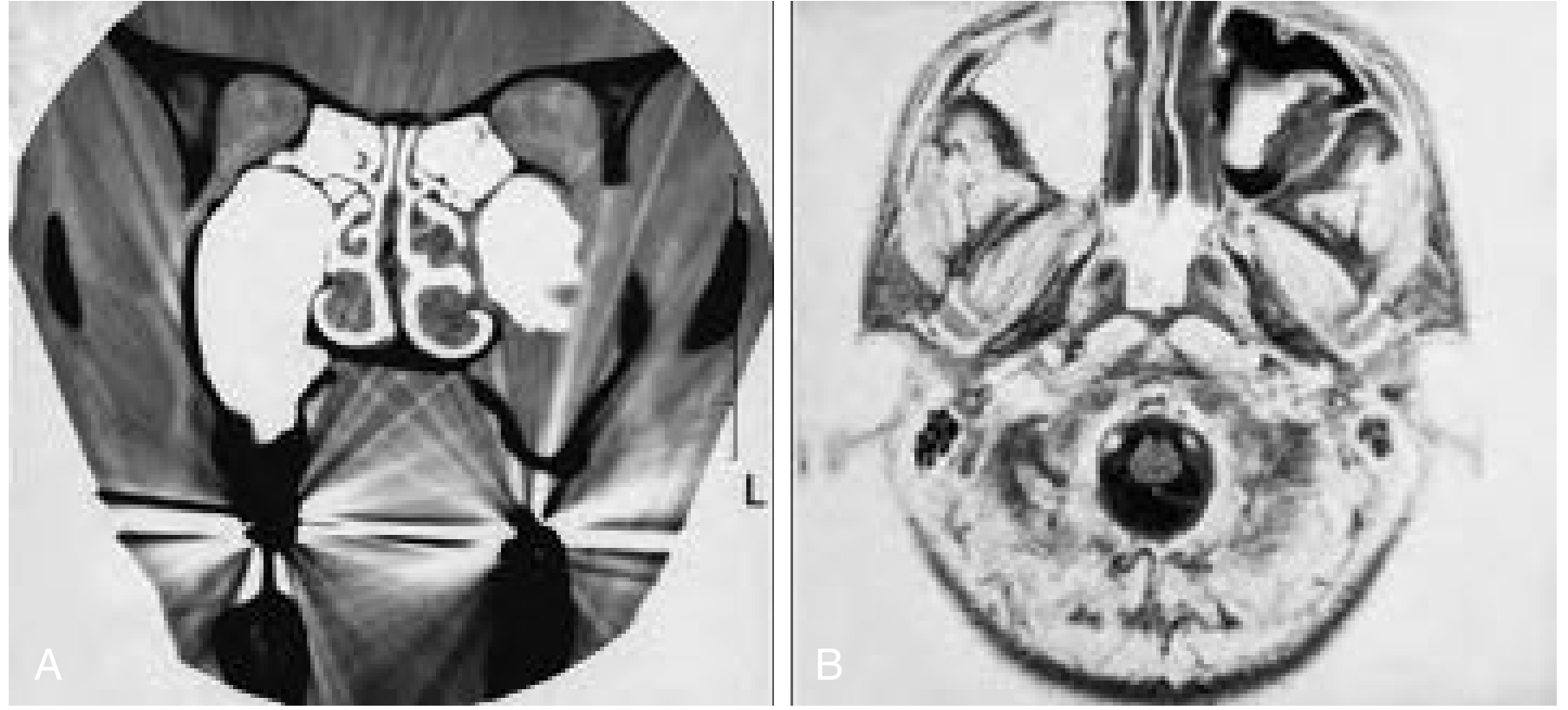
Fig: (A) Coronal CT - left maxillary sinusitis with erosion of the superior lateral bony wall. (B) T2 axial MRI - thickened left maxillary sinus mucosa with hyperintense inflammation and a hypointense signal corresponding to bone destruction. Differential includes invasive fungal disease, lymphoma, and SCC.
- Cummings Otolaryngology Head and Neck Surgery, p.231-233
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 1
Nosocomial Sinusitis
Occurs in critically ill patients, particularly those with nasotracheal intubation. Management: address precipitating factors (e.g., remove nasal tube) and treat empirically with broad-spectrum antibiotics until culture/sensitivity results are available.
Special Populations
Immunocompromised Patients
Initial evaluation includes thorough head and neck exam, nasal endoscopy, and endoscopy-guided cultures from the middle meatus or sphenoethmoid recess. A low threshold for imaging in patients with low neutrophil or CD4 counts is advised. Goals include swift treatment of bacterial sinusitis and early identification of fungal sinusitis or neoplasm.
Recurrent Acute Sinusitis
Consider: nasal culture during episodes, CT imaging between episodes to identify anatomic abnormalities (e.g., septal deviation, concha bullosa), and allergic/immunologic evaluation.
Kartagener Syndrome
Sinusitis + bronchiectasis + situs inversus - due to inherited genetic defects in ciliary action.
Recent Evidence (2025)
A meta-analysis (Magboul et al., Rhinology 2025) supports budesonide nasal irrigation as an effective and safe treatment for chronic rhinosinusitis (PMID 39729039). An Italian intersociety consensus (2025) addressed sinusitis treatment in children, reinforcing antibiotic stewardship principles in the pediatric setting (PMID 40140854).
This is a shared conversation. Sign in to Orris to start your own chat.