Anal fistulae
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
anal fistula management treatment
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information from multiple textbooks plus imaging. Let me compile the full answer.
Anal Fistulae (Fistula-in-Ano)
Definition
Fistula derives from the Latin for "pipe." An anal fistula is an abnormal communication between the anal canal (or rectum) and the perianal skin - or occasionally to adjacent organs. It always has an internal opening (usually at the dentate line) and an external opening (usually on the perianal skin within ~3 cm of the anal verge).
- Pfenninger and Fowler's Procedures for Primary Care, p. 693
Aetiology and Pathophysiology
The vast majority (~90%) arise from cryptoglandular infection: bacteria infect one of the anal glands that open at the base of the anal crypts at the dentate line. Instead of spontaneously draining back into the anal canal, the infection spreads laterally through the sphincter complex into perianal tissues, forming an abscess. When that abscess discharges to the skin, the tract persists as a fistula.
About 30-40% of anorectal abscesses eventually result in a fistula. Fewer than 20% of first-time abscesses do, but if a patient presents with a recurrent abscess at the same site, the probability rises to >50%.
Risk factors for fistula development:
- Crohn's disease (fistulas occur in 13-54% of Crohn's patients)
- Immunocompromise (steroids, HIV)
- Diabetes mellitus
- Prior perianal radiation
- Tuberculosis, malignancy, actinomycosis (less common)
Non-cryptoglandular causes (~10%): IBD, tuberculosis, malignancy, radiation.
- Harrison's Principles of Internal Medicine 22E, p. 2629
Classification: Parks Classification
Fistulae are classified by their relationship to the anal sphincter complex. This is the most widely used system.
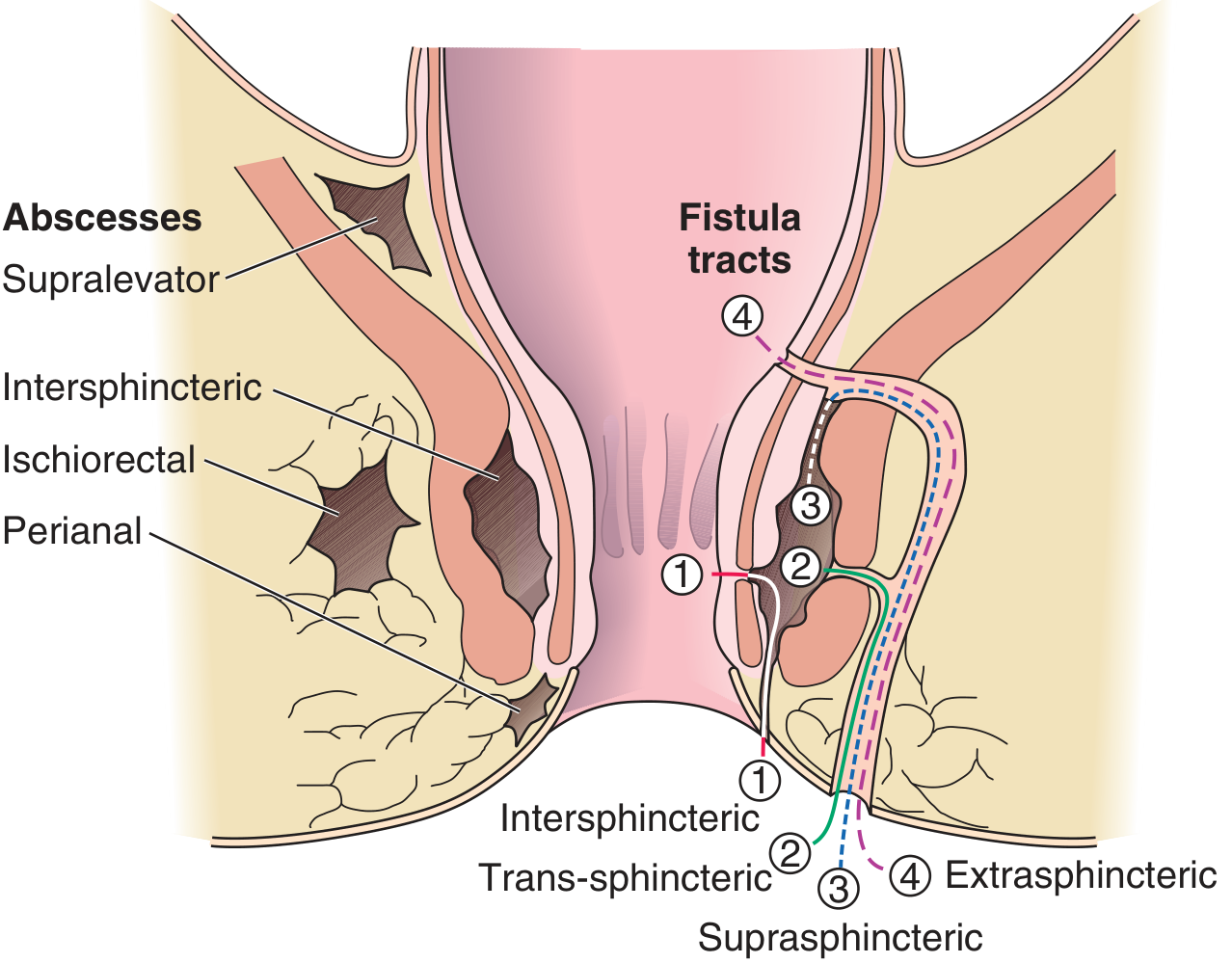
Harrison's Fig. 339-5: Anorectal abscess locations (left) and fistula tract types (right).
| Type | Frequency | Course |
|---|---|---|
| Intersphincteric | ~70% | Tract passes between internal and external sphincter, exits at perianal skin |
| Transsphincteric | ~23% | Passes through both sphincters into the ischiorectal fossa |
| Suprasphincteric | ~5% | Passes up over the puborectalis, then down through the ischiorectal fossa |
| Extrasphincteric | ~2% | Passes entirely outside both sphincters; often iatrogenic or Crohn-related |
A fistula is also classified as simple (single tract, low risk to sphincter) or complex (multiple tracts, involves significant sphincter, anterior in women, associated with IBD, radiation, or malignancy).
Clinical Features
- Constant or intermittent purulent discharge from the perianal area - this is the hallmark symptom
- Perianal pain and tenderness
- History of prior perianal abscess (often recurrent)
- A visible external opening on the perianal skin, often with granulation tissue; may be inflamed or may close over superficially
The external opening rarely closes spontaneously and permanently; as long as it remains open, a new abscess does not form.
Evaluation
History
Duration, prior anorectal surgery, sphincter function, bowel habit changes (to exclude IBD), urogenital symptoms.
Physical Examination
Inspection and gentle digital rectal exam. The external opening is usually visible. The internal opening may be palpable as a nodule at the dentate line.
Goodsell's Rule
A useful anatomical guide to predict the internal opening location:
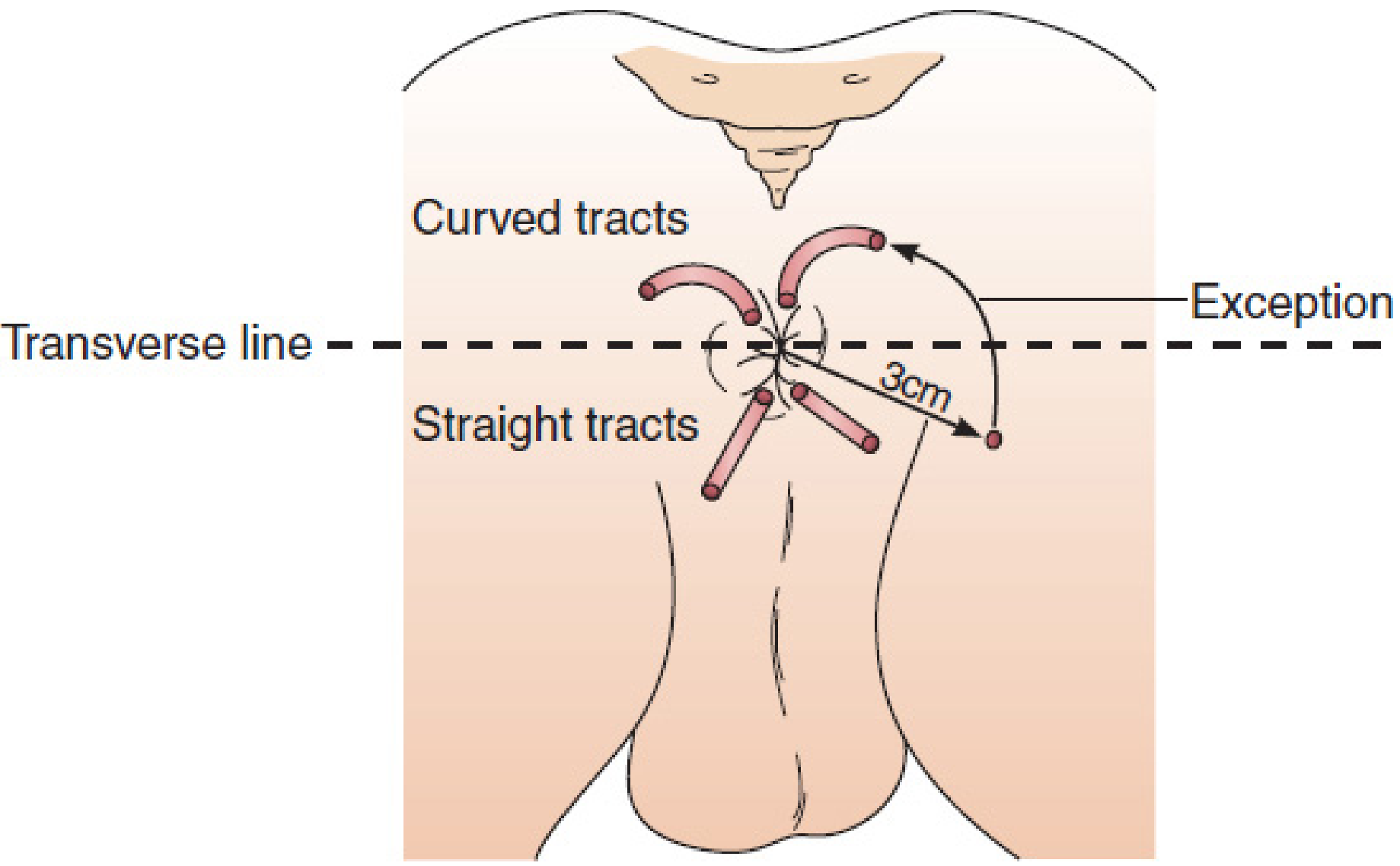
- External openings posterior to a transverse line through the anus → internal opening in the posterior midline
- External openings anterior to the transverse line → internal opening at the nearest crypt
- Exception: an opening >3 cm from the anal verge may have upward extension and not follow the rule
Investigations
- Examination under anaesthesia (EUA) - the gold standard; allows probing the tract, injection of hydrogen peroxide through the external opening to identify the internal opening
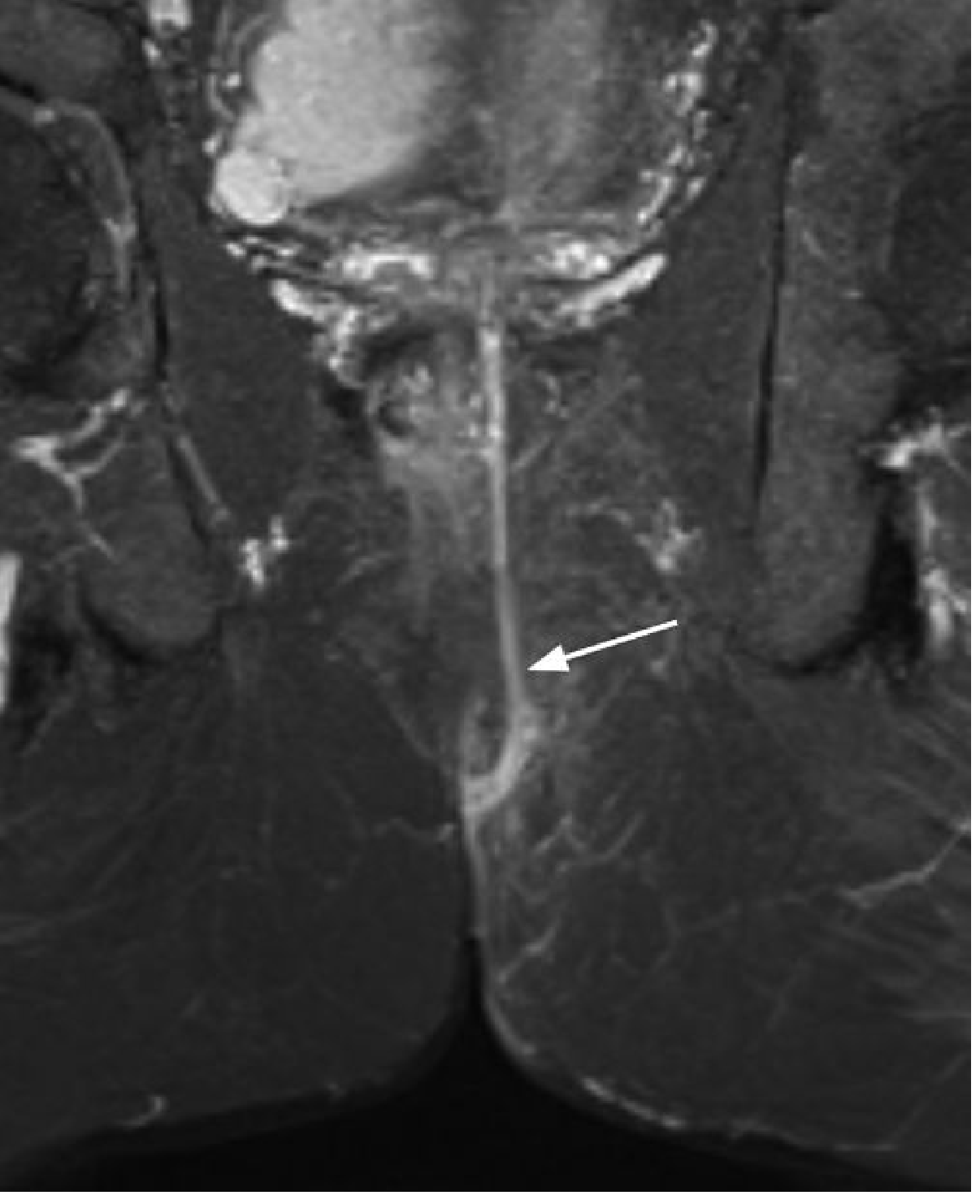
- MRI - the imaging modality of choice for complex fistulae; achieves ~80% accuracy in delineating tracts. Fat-suppressed T2W (STIR) sequences show the fistula tract as high signal against the lower-signal sphincter and adjacent fat. Also detects associated abscesses and supralevator collections that are clinically occult. Preoperative MRI reduces recurrence rates in complex disease.
-
Endoanal ultrasound (EUS) - useful for identifying the tract and internal opening, particularly within the sphincter complex
-
Fistulography (water-soluble contrast with fluoroscopy) - for complex or multi-tract disease
-
Grainger & Allison's Diagnostic Radiology, p. 593
-
Mulholland and Greenfield's Surgery 7e, p. 3561
Differential Diagnosis
- Hidradenitis suppurativa - inflammation of apocrine sweat glands; tracts are superficial and do not connect to the anal canal
- Pilonidal disease - origin in the gluteal cleft, foreign body reaction to hair; does not have an internal opening at the dentate line
- Crohn's disease (may coexist)
- Rectovaginal or rectourethral fistula
Management
The goal is to eradicate the fistula tract while preserving sphincter function. The choice of technique depends on how much sphincter muscle the tract involves.
1. Fistulotomy (unroofing)
- The tract is laid open by incising the overlying tissue.
- Suitable for simple, low fistulas where less than ~30% of the sphincter is involved.
- Healing rates up to 90%.
- Risk: incontinence if too much sphincter is divided; women are particularly at risk for anterior fistulotomy.
- Post-op: wound heals by secondary intention over 4-6 weeks; must be kept open from inside out.
- A 2025 meta-analysis (Quinn et al., ANZ J Surg, PMID 40125894) directly compared fistulotomy vs. fistulectomy in RCTs.
2. Seton Placement
- A vessel loop or silk tie is passed through the tract.
- Two uses:
- Draining seton: maintains patency, reduces inflammation; used as a bridge before definitive repair.
- Cutting seton: progressively tightened every 2-4 weeks to slowly erode through the sphincter, inducing fibrosis. Success rates up to 94%, but incontinence rates of 23% or more are reported.
- Required before most sphincter-preserving procedures (LIFT, advancement flap) to allow fibrosis and reduce inflammation.
3. Endoanal Advancement Flap
- A flap of mucosa with underlying internal sphincter is raised, the tract is curetted, the internal opening sutured, and the flap is advanced to cover it.
- Used for complex fistulas. Success rate: 66-87%.
- Can be repeated after an interval if it fails.
4. LIFT Procedure (Ligation of Intersphincteric Fistula Tract)
- After seton-induced fibrosis, an incision is made in the intersphincteric groove; both ends of the tract are ligated and the tract is divided.
- Reported success: 40-95% (wide range across studies).
- Sphincter-preserving.
5. Fibrin Glue and Fistula Plug
- Associated with high recurrence rates and are not recommended as primary treatment.
6. Medical Management (Crohn's-related fistulae)
- Anti-TNF agents (infliximab, adalimumab) are the cornerstone.
- Asymptomatic Crohn's fistulae do not need treatment.
- Long-term seton placement + medical therapy for complex Crohn's fistulae.
- Allogeneic adipose-derived mesenchymal stem cell therapy (darvadstrocel / ADMIRE study): 59% remission at 52 weeks vs. 42% placebo - statistically significant but cost is prohibitive.
- Temporary fecal diversion may facilitate healing; proctectomy is reserved for severe refractory perianal Crohn's disease.
7. Emerging: Laser-based therapies
- A 2025 systematic review (Duda et al., Int J Colorectal Dis, PMID 40936062) evaluated laser-based techniques with and without adjunctive measures.
Complications of Surgery
- Anal incontinence - the major concern; risk increases with amount of sphincter divided
- Fistula recurrence - especially if the wound closes prematurely before the deep tract has healed, or if complex tracts are missed
- Creating a false tract with aggressive probing
- Missing a concurrent occult perianal abscess
- Missing underlying Crohn's disease (requires specific medical approach)
Key Points Summary
| Feature | Detail |
|---|---|
| Most common cause | Cryptoglandular infection / perianal abscess |
| Internal opening | Usually at dentate line |
| Most common type | Intersphincteric (70%) |
| Best imaging | MRI (STIR T2W) |
| Gold standard evaluation | Examination under anaesthesia |
| Treatment for simple fistula | Fistulotomy |
| Treatment for complex/high fistula | Seton + staged repair (LIFT, advancement flap) |
| Crohn's first-line | Anti-TNF + long-term seton |
Sources: Harrison's Principles of Internal Medicine 22E, p. 2629 | Mulholland and Greenfield's Surgery 7e, pp. 3560-3563 | Pfenninger and Fowler's Procedures for Primary Care, pp. 693-695 | Grainger & Allison's Diagnostic Radiology, p. 593
This is a shared conversation. Sign in to Orris to start your own chat.