Explain ventricular septal defect
Reading File
Finding Sources
Searching PubMed
"ventricular septal defect"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to deliver a thorough answer. Let me compile everything.
Ventricular Septal Defect (VSD)
Definition and Epidemiology
A ventricular septal defect (VSD) is an abnormal opening (hole) in the interventricular septum that allows communication between the left ventricle (LV) and right ventricle (RV). VSDs are the most common congenital cardiac anomaly diagnosed at birth, comprising 20-30% of all congenital heart disease (CHD). They range in size from 3-4 mm to over 3 cm and can occur as isolated lesions or as part of more complex malformations (e.g., tetralogy of Fallot).
- Robbins & Kumar Basic Pathology
- Schwartz's Principles of Surgery, 11th Edition
Embryology
The ventricular septum forms by two components:
- A muscular ridge growing upward from the cardiac apex
- A membranous partition growing downward from the endocardial cushions
The basal (membranous) region is the last part to close and is where ~90% of VSDs occur. Failure of these components to fuse properly results in a VSD.
Types / Anatomical Classification
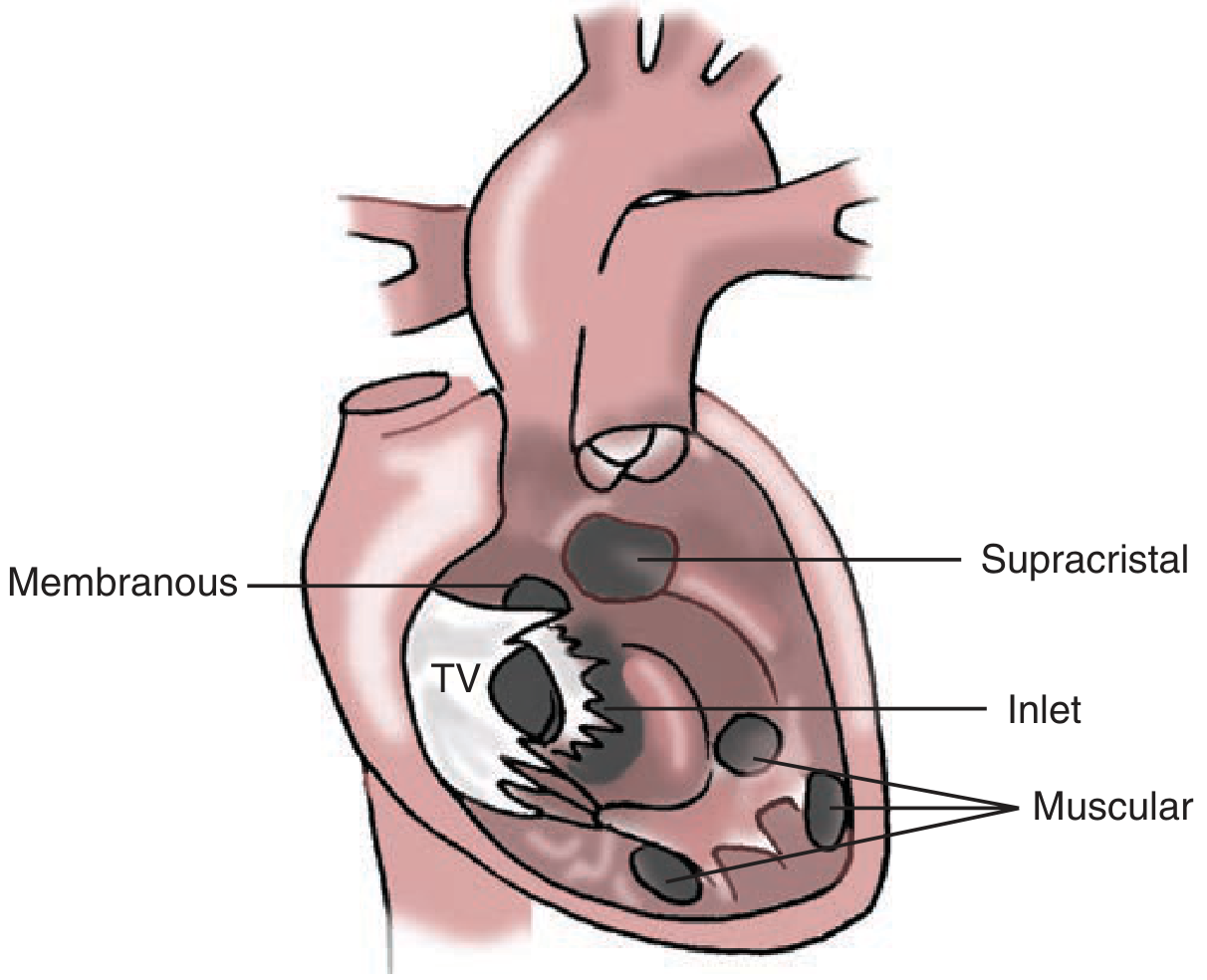
Figure: Types of VSD by location (Schwartz's Principles of Surgery)
The interventricular septum is divided into four regions, each giving rise to a distinct VSD type:
| Type | Location | Notes |
|---|---|---|
| Perimembranous (paramembranous, conoventricular) | Membranous septum, below aortic valve | Most common type requiring surgery (~80% of surgically treated VSDs); includes malalignment defects of tetralogy of Fallot |
| Supracristal / Outlet (infundibular) | Conal septum, above crista supraventricularis, below pulmonary valve | Risk of aortic valve prolapse through the defect |
| Inlet / AV canal | Crux of the heart, between tricuspid and mitral valves | Often associated with AV canal anomalies |
| Muscular (trabecular) | Trabecular septum, toward apex | Most common type overall; can be multiple ("Swiss cheese" defect) |
Gross Pathology
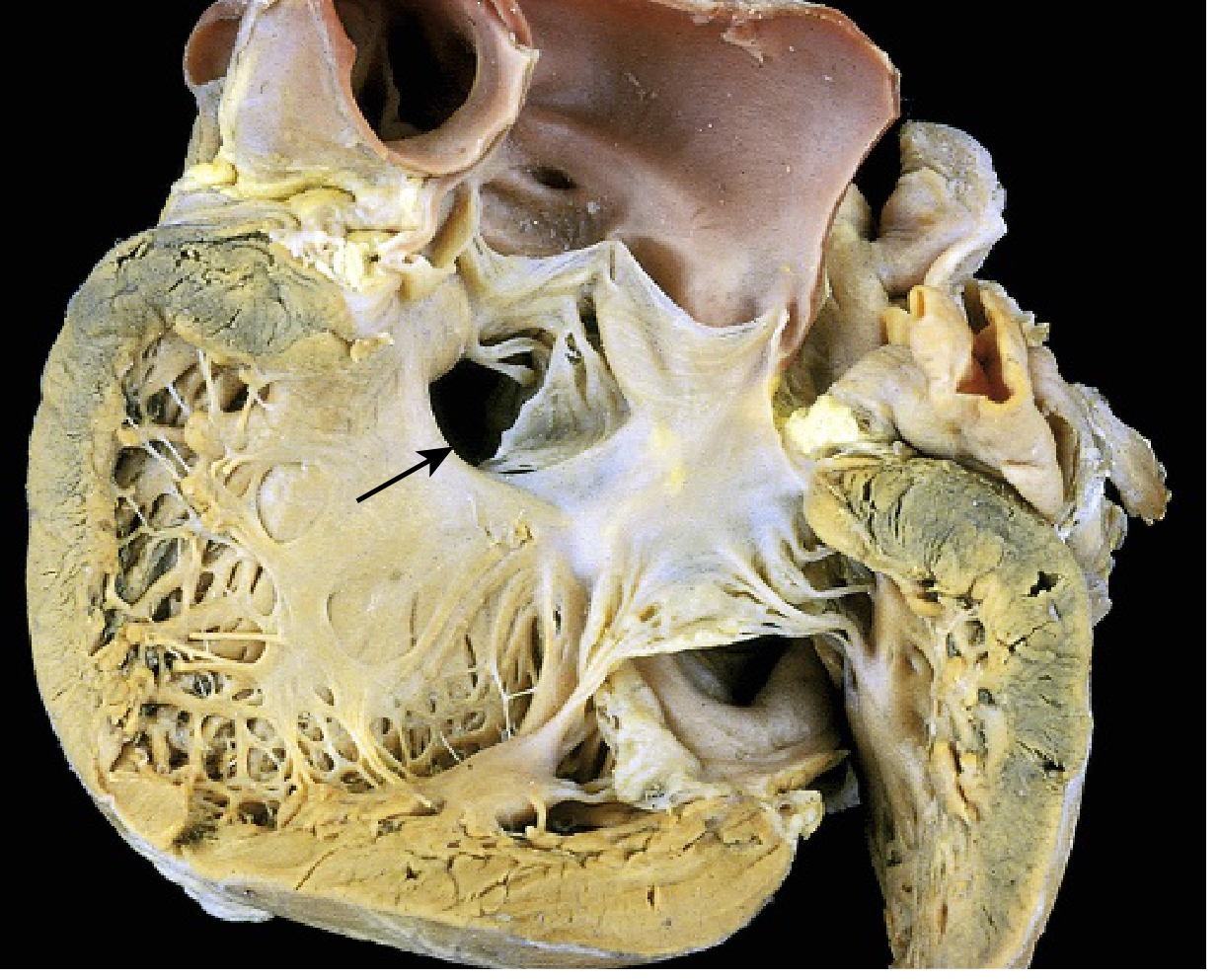
Figure: Membranous VSD (arrow) - Robbins & Kumar Basic Pathology (Courtesy of William D. Edwards, MD, Mayo Clinic)
With significant left-to-right shunting, there is:
- RV hypertrophy and dilation
- Enlargement of the pulmonary artery (from increased RV output and elevated pressures)
- Vascular changes of pulmonary hypertension in the lung parenchyma
Pathophysiology
The direction and magnitude of shunting depend on defect size and the ratio of pulmonary vascular resistance (PVR) to systemic vascular resistance (SVR).
Shunting occurs predominantly during systole because LV pressure exceeds RV pressure at that phase.
Small / Restrictive VSD
- High resistance to flow across defect
- RV pressure normal or minimally elevated
- Qp:Qs ratio rarely exceeds 1.5
- Usually asymptomatic
- Risk of infective endocarditis from jet lesion damaging the endocardium
Moderate VSD
- Qp:Qs > 1.2
- Elevated pulmonary artery pressure, but PVR not yet elevated
- LA and LV dilation proportional to shunt magnitude
Large / Non-restrictive VSD
- Qp:Qs ≥ 1.5, often much higher
- Elevated pulmonary artery pressure AND elevated PVR
- Massive left-to-right shunting causes congestive heart failure (CHF) in infancy
- If untreated, chronic volume and pressure overload causes progressive pulmonary vascular disease
Eisenmenger Syndrome
Prolonged, untreated large VSDs lead to irreversible pulmonary hypertension. When pulmonary pressure exceeds systemic pressure, shunt reversal occurs (now right-to-left), causing cyanosis. This affects ~10% of patients with VSDs - typically when the defect is as large as the aorta. Once Eisenmenger syndrome develops, surgical closure is contraindicated.
Clinical Features
Small VSD:
- Asymptomatic
- Harsh, high-pitched holosystolic murmur at the left lower sternal border (due to jet effect)
- Risk of infective endocarditis
Large VSD (infants):
- Congestive heart failure: tachypnea, poor feeding, failure to thrive
- Frequent respiratory tract infections
- Sweating during feeds
Eisenmenger syndrome:
- Progressive cyanosis
- Clubbing
- Polycythemia
- May appear deceptively asymptomatic until frank cyanosis develops
Spontaneous Closure
About half of all native VSDs close spontaneously. Most closures happen in the first decade of life:
- At 1 month of age: ~80% chance of spontaneous closure
- At 12 months of age: only ~25% chance
- Spontaneous closure in adult life is unusual
Perimembranous VSDs may close by tricuspid valve leaflet tissue adhering to the defect edges ("aneurysm of the membranous septum").
Diagnosis
- Chest X-ray: Cardiomegaly, pulmonary plethora (overcirculation)
- ECG: Left ventricular hypertrophy; biventricular hypertrophy in large defects; right ventricular hypertrophy if pulmonary hypertension develops
- Echocardiography (with color Doppler): Definitive modality - identifies defect location, estimates shunt size, and measures pulmonary arterial pressures
- Cardiac catheterization: Reserved for older patients where pulmonary resistance measurement is needed before closure; largely supplanted by echo
Treatment
Conservative
Small, restrictive VSDs with Qp:Qs < 1.5 and normal pulmonary pressures are observed, given the high rate of spontaneous closure.
Indications for Closure
- Qp:Qs ≥ 1.5 with volume overload
- Symptoms of heart failure
- Elevated pulmonary artery pressure
- Recurrent endocarditis
- Aortic valve prolapse (especially supracristal VSDs)
Surgical Repair
- Performed under cardiopulmonary bypass
- Patch closure with a Dacron or pericardial patch using interrupted sutures is the standard technique
- Mortality is low in experienced centers (<1-2% for isolated VSDs)
- Perimembranous VSDs require care to avoid injury to the AV node and bundle of His (the conduction system runs along the posteroinferior rim)
Transcatheter (Device) Closure
- Device closure via cardiac catheterization is now available for selected muscular and perimembranous VSDs
- Preferred for muscular VSDs (especially mid-ventricular and apical) where surgical access is difficult
Complications
| Complication | Mechanism |
|---|---|
| Congestive heart failure | Volume overload from large left-to-right shunt |
| Pulmonary hypertension | Increased pulmonary blood flow and pressure |
| Eisenmenger syndrome | Irreversible pulmonary vascular disease with shunt reversal |
| Infective endocarditis | Jet lesion damages endocardium → colonization nidus |
| Aortic regurgitation | Supracristal VSDs allow aortic cusp prolapse |
| Complete heart block | Surgical complication from AV node injury |
Key Points Summary
- VSDs are the most common congenital heart defect (~20-30% of all CHD)
- The membranous septum is the last to close embryologically and the site of ~90% of defects
- Perimembranous type is most common surgically; muscular type is most common overall
- Shunting is left-to-right (acyanotic) initially, becoming right-to-left (cyanotic - Eisenmenger) if untreated
- Half of small VSDs close spontaneously, mostly in the first year
- Echocardiography is the diagnostic gold standard
- Large symptomatic VSDs require repair to prevent irreversible pulmonary vascular disease
Sources: Schwartz's Principles of Surgery, 11th Edition | Goldman-Cecil Medicine | Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.