Glomerular Filtration and GFR
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have thorough, multi-source content to deliver a comprehensive answer. Let me compile everything.
Glomerular Filtration and GFR
Overview
Glomerular filtration is the first step in urine formation. As renal blood flow enters the glomerular capillaries, a portion of the plasma is forced across the capillary wall into Bowman's space, producing an ultrafiltrate - a fluid containing water and small solutes, but essentially free of plasma proteins and blood cells. Under normal conditions, the two kidneys together produce a GFR of 125 mL/min (180 L/day).
This enormous filtration rate is essential because it exposes the entire extracellular fluid volume to tubular scrutiny more than 10 times per day, allowing rapid elimination of toxins and waste. If GFR falls to 10% of normal (as in end-stage renal disease), the plasma blood urea nitrogen must rise ~10-fold just to maintain the same rate of urea excretion.
- Medical Physiology, p. 1100
- Costanzo Physiology 7th Ed., p. 267
The Glomerular Filtration Barrier
The glomerular capillary wall has three layers that together constitute the filtration barrier:
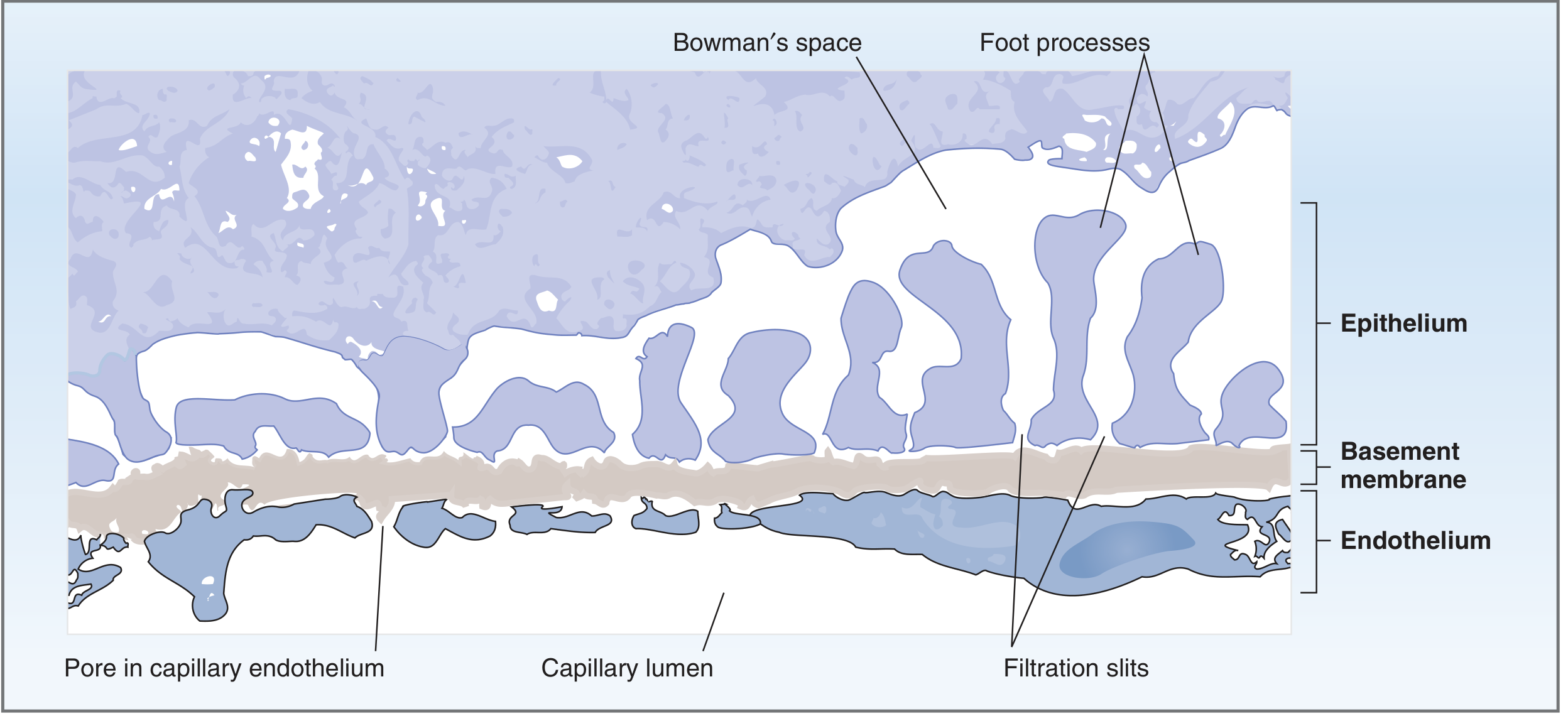
1. Fenestrated Endothelium
Pores of 70-100 nm in diameter. Large enough for fluid and plasma proteins, but not blood cells. The endothelial surface is coated with a negatively charged glycocalyx that repels plasma proteins.
2. Glomerular Basement Membrane (GBM)
Three sub-layers:
- Lamina rara interna - fused to endothelium
- Lamina densa - middle, most restrictive layer; a meshwork of collagen and negatively charged proteoglycans
- Lamina rara externa - fused to the podocytes
The GBM is the most significant barrier to plasma protein filtration.
3. Visceral Epithelium (Podocytes)
Podocytes have long foot processes (pedicels) that encircle the capillaries. Between adjacent foot processes are filtration slits (25-60 nm) bridged by thin slit diaphragms composed of proteins including nephrin and podocin. Mutations in nephrin alone cause proteinuria. This layer adds an additional size barrier.
- Costanzo Physiology 7th Ed., pp. 267-268
- Guyton & Hall Textbook of Medical Physiology, p. 335
Charge Selectivity of the Barrier
Beyond size, the barrier carries fixed negative charges on the endothelium, all layers of the GBM, and the podocytes. This has critical consequences:
- Small solutes (Na+, K+, Cl-): freely filtered regardless of charge
- Large solutes (plasma proteins): repelled by negative charges + excluded by pore size - doubly restricted from filtration
- Cationic macromolecules: more filterable (attracted to negative barrier)
- Anionic macromolecules: least filterable (repelled)
In diseases that strip the negative charges from the barrier (e.g., minimal change disease), proteinuria results even without overt structural disruption.
- Costanzo Physiology 7th Ed., pp. 268-269
Starling Forces Governing GFR
GFR is governed by the Starling equation applied to the glomerular capillary:
GFR = K_f × [(P_GC - P_BS) - π_GC]
| Parameter | Description | Value (approx.) |
|---|---|---|
| K_f | Filtration coefficient (permeability × surface area) | Very high - >100× systemic capillaries |
| P_GC | Hydrostatic pressure in glomerular capillary - favors filtration | ~45 mm Hg |
| P_BS | Hydrostatic pressure in Bowman's space - opposes filtration | ~10 mm Hg |
| π_GC | Oncotic pressure of capillary blood - opposes filtration | ~27 mm Hg (rising along capillary) |
Net ultrafiltration pressure at the start of the capillary: 45 - 10 - 27 = +8 mm Hg (favoring filtration)
As blood flows along the capillary and protein-free fluid is filtered out, π_GC rises progressively until the net pressure reaches zero - a state called filtration equilibrium, which normally occurs at the end of the glomerular capillary.
- Costanzo Physiology 7th Ed., pp. 268-270
Filtration Fraction
The filtration fraction (FF) is the fraction of renal plasma flow (RPF) that is actually filtered:
FF = GFR / RPF ≈ 125 / 625 = 0.20 (20%)
About 20% of all plasma entering the glomerular capillaries is filtered into Bowman's space under normal conditions.
- Guyton & Hall, p. 335; Harrison's Principles, p. XX
Effect of Arteriolar Changes on GFR
| Condition | RPF | GFR | Filtration Fraction |
|---|---|---|---|
| Afferent arteriole constriction | ↓ | ↓ | No change |
| Efferent arteriole constriction | ↓ | ↑ | ↑ |
| ↑ plasma protein concentration | No change | ↓ | ↓ |
| ↓ plasma protein concentration | No change | ↑ | ↑ |
| Ureteral obstruction | No change | ↓ | ↓ |
Key distinction: Afferent constriction reduces P_GC and thus GFR. Efferent constriction raises P_GC (blood trapped in the glomerulus) and raises GFR, while reducing overall RPF.
Angiotensin II preferentially constricts efferent arterioles, which at low concentrations maintains or raises GFR even while reducing RPF - a protective mechanism in volume depletion. ACE inhibitors block this protection, which is why they can precipitate acute kidney injury in bilateral renal artery stenosis.
- Costanzo Physiology 7th Ed., pp. 270-271
Measurement of GFR
The Clearance Concept
GFR is calculated using the clearance formula for an ideal marker (substance X):
GFR = (U_x × V̇) / P_x
Where U_x = urine concentration, V̇ = urine flow rate, P_x = plasma concentration.
Criteria for an Ideal GFR Marker
- Freely filterable at the glomerulus
- Not reabsorbed or secreted by the tubules
- Not synthesized, broken down, or stored in the kidney
- Physiologically inert
Inulin - The Gold Standard
Inulin (a fructose polymer, MW ~5000 Da) meets all criteria. Inulin clearance = true GFR. Importantly, GFR measured by inulin clearance is independent of both plasma inulin concentration and urine flow rate (when one rises, the other falls proportionately, so the product stays constant).
Clinical Surrogates for GFR
Inulin requires IV infusion and is impractical clinically. Instead:
Creatinine clearance is routinely used but overestimates GFR slightly because creatinine is also secreted by proximal tubules (but close enough for clinical purposes).
Estimated GFR (eGFR) equations:
- MDRD equation: eGFR = 175 × (P_Cr)^-1.154 × (Age)^-0.203 × (0.742 if female) × (1.212 if African American)
- CKD-EPI equation (more accurate): Improves on MDRD, especially at higher GFR values
- Cockcroft-Gault formula: eGFR = [140 × Age × Weight × (0.85 if female)] / [72 × P_Cr] - includes body weight, useful for drug dosing
Cystatin C is an alternative endogenous marker that is less affected by muscle mass.
- Medical Physiology, p. 1101; Costanzo Physiology, p. 272
Autoregulation of GFR
Despite wide swings in systemic arterial pressure (80-180 mm Hg), the kidneys maintain a remarkably stable RBF and GFR through autoregulation - a process independent of renal nerves and circulating hormones (persists even in denervated, isolated kidneys).
Two Mechanisms (equally important):
1. Myogenic Response
When arterial pressure rises, afferent arteriolar smooth muscle is stretched, triggering opening of stretch-activated nonselective cation channels → depolarization → Ca²+ influx → vasoconstriction. This directly resists the pressure rise and maintains constant capillary pressure.
2. Tubuloglomerular Feedback (TGF)
The juxtaglomerular apparatus (JGA) mediates this reflex:
- ↑ GFR → ↑ NaCl delivery to the macula densa (thick ascending limb)
- Macula densa cells release ATP into the extracellular space
- ATP is metabolized to adenosine - a potent vasoconstrictor of the afferent arteriole
- Afferent arteriole constricts → ↓ P_GC → GFR returns to normal
- Angiotensin II and reactive oxygen species enhance TGF; nitric oxide blunts it
3. Angiotensin II (third component - Harrison's)
During reduced renal perfusion, granular cells of the JGA release renin → angiotensin I → angiotensin II → efferent arteriole vasoconstriction → maintains glomerular pressure and GFR despite systemic hypoperfusion.
At very low perfusion pressures (e.g., congestive heart failure), efferent arteriolar resistance increases via angiotensin II to partially preserve GFR.
- Medical Physiology, pp. 1102-1103
- Harrison's Principles of Internal Medicine 22E, p. XX
Normal GFR Values and Age-Related Decline
| Group | Normal GFR |
|---|---|
| Young adult male | ~130 mL/min/1.73 m² |
| Young adult female | ~120 mL/min/1.73 m² |
| Standard value used in physiology | 125 mL/min (180 L/day) |
GFR declines substantially with normal aging - from young adulthood to age 70-75, healthy adults lose nearly half their nephrons. This decline is accelerated by diabetes, hypertension, and glomerulonephritis.
- Guyton & Hall, p. 334
Clinical Significance
| Condition | GFR Impact | Mechanism |
|---|---|---|
| Diabetes mellitus | Initially ↑ (hyperfiltration), then ↓ | Mesangial expansion, podocyte loss |
| Bilateral renal artery stenosis + ACE inhibitor | ↓↓ GFR | Removal of angiotensin II-mediated efferent tone |
| Volume depletion / hemorrhage | ↓ | ↓ P_GC via reduced RPF; angiotensin II compensates |
| Ureteral obstruction | ↓ | ↑ P_BS opposing filtration |
| Nephrotic syndrome | ↓ filtration of albumin loses → ↓ oncotic pressure | Loss of negative charge barrier / structural damage |
| CKD | Progressive ↓ | Nephron loss |
Sources:
- Costanzo Physiology, 7th Edition
- Medical Physiology (Boron & Boulpaep)
- Guyton & Hall Textbook of Medical Physiology
- Harrison's Principles of Internal Medicine, 22nd Edition
- Brenner and Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.