patent ductus defect of CHD tell me every single information of this topic like definition , etiology, symptoms , pathophsiology, digonosis and treatment and also other information
Reading File
Finding Sources
Finding Sources
Searching PubMed
"patent ductus arteriosus"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the comprehensive information needed. Let me compile the complete, detailed answer:
Patent Ductus Arteriosus (PDA) - Complete Guide
1. Definition
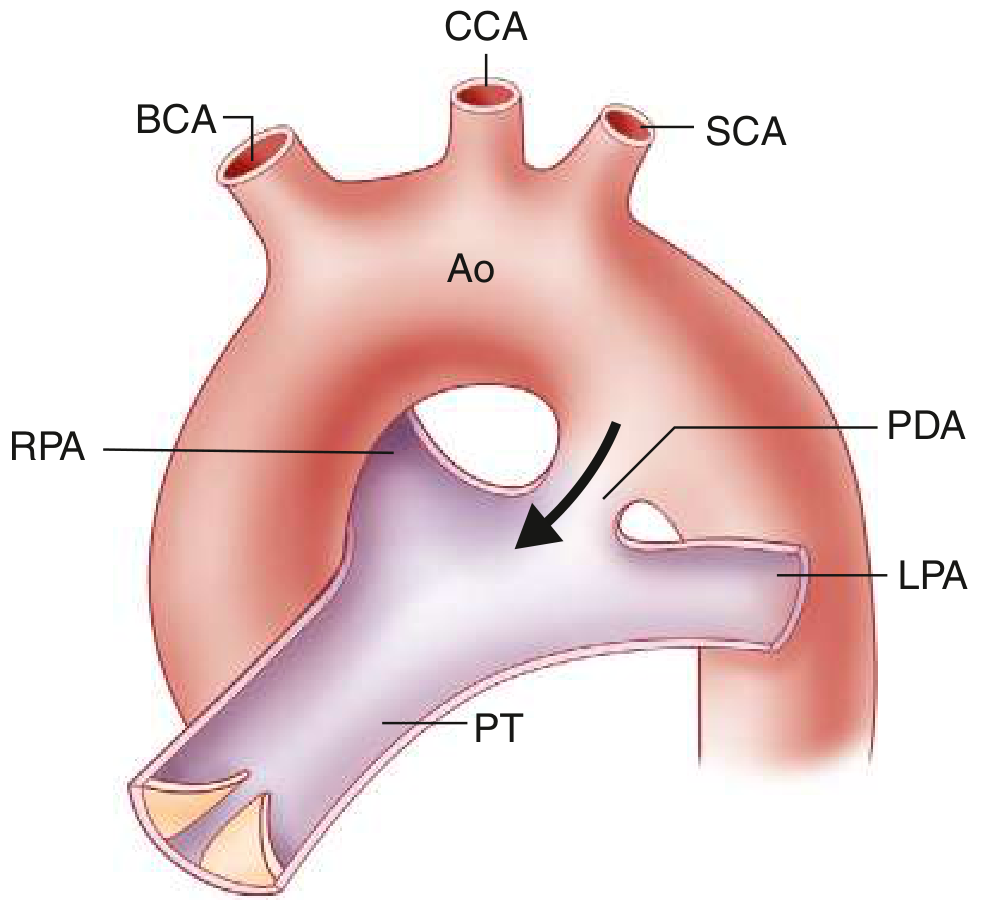
Patent Ductus Arteriosus (PDA) is a congenital heart defect in which the ductus arteriosus - a normal fetal vascular channel connecting the main pulmonary artery (or left pulmonary artery) to the upper descending thoracic aorta, just distal to the origin of the left subclavian artery - fails to close after birth.
- In fetal life, the ductus is functionally essential, carrying approximately 60% of combined ventricular output from the pulmonary artery to the aorta (bypassing the fluid-filled, non-functional lungs).
- After birth, it should close functionally within 10-15 hours and anatomically (forming the ligamentum arteriosum) within the first few months.
- When it fails to close, blood shunts from the high-pressure aorta into the lower-pressure pulmonary artery (left-to-right shunt), causing pulmonary overcirculation and left heart volume overload.
PDA accounts for approximately 7% of all congenital heart lesions, with about 90% of these being isolated defects.
- Robbins & Kumar Basic Pathology, Schwartz's Principles of Surgery 11th Ed.
2. Anatomy
- The ductus is derived from the 6th aortic arch (left side).
- In the neonate, its length ranges from 2 to 8 mm and diameter from 4 to 12 mm.
- Normal closure leaves a fibrous remnant called the ligamentum arteriosum.
3. Etiology & Risk Factors
Incidence
- Approximately 1 in every 2000 births in term infants.
- Dramatically increases with prematurity - present in up to 75% of infants born at 28-30 weeks gestation.
- Female predominance: 2:1 female-to-male ratio.
Causes & Risk Factors
| Category | Details |
|---|---|
| Prematurity | Most important risk factor. Virtually ALL preterm neonates ≤28 weeks with birth weight <1750 g have a PDA in the first 24 hours |
| Hypoxia | Respiratory distress syndrome (RDS), surfactant deficiency, high-altitude residence - all reduce oxygen tension, which is the main stimulus for ductal closure |
| Maternal Rubella | One of the classic teratogenic associations; rubella in early pregnancy strongly associated with PDA |
| Failure of TGF-β induction | TGF-β normally triggers post-natal ductal involution; its absence may cause persistent patency |
| Chromosomal anomalies | Trisomy 21 (Down syndrome), trisomy 18, etc. |
| Associated CHDs | Coarctation of the aorta, Transposition of the Great Arteries (TGA), pulmonary stenosis/atresia - large pressure differences between aorta and pulmonary artery prevent normal constriction |
| Pharmacologic | Prostaglandin infusion (used therapeutically to keep ductus open in duct-dependent lesions) |
- The Developing Human (Clinically Oriented Embryology), Schwartz's Principles of Surgery
4. Normal Physiology of Ductal Closure
Understanding normal closure explains why PDA occurs:
-
Fetal state: Locally produced prostaglandin E2 (PGE2) and prostaglandin I2 (PGI2) maintain active muscular relaxation of the ductal wall, keeping it widely patent. Placenta is also a key source of these prostaglandins.
-
At birth:
- Increased pulmonary blood flow metabolizes PGE2 and PGI2.
- Removal of the placenta eliminates a major prostaglandin source.
- Release of histamines, catecholamines, bradykinin, and acetylcholine promote ductal contraction.
- Rising arterial oxygen tension is the primary stimulus for smooth muscle contraction - ductal closure begins within 10-15 hours.
-
Anatomic closure by fibrosis occurs over subsequent weeks to months, producing the ligamentum arteriosum.
- Schwartz's Principles of Surgery 11th Ed.
5. Pathophysiology
The hemodynamic consequences depend entirely on the size of the ductus and the pressure/resistance ratio between the pulmonary and systemic circulations.
Left-to-Right Shunt (the usual pattern)
Since aortic pressure exceeds pulmonary artery pressure throughout the cardiac cycle (both systole AND diastole), blood flows continuously from the aorta into the pulmonary artery. This results in:
- Pulmonary overcirculation: increased pulmonary blood flow returning to the left atrium.
- Left atrial and left ventricular volume overload with dilation.
- Elevated pulmonary artery pressure - if large/unrestrictive shunt.
- Right ventricular strain from augmented afterload.
- Increased sympathetic discharge → tachycardia, tachypnea, ventricular hypertrophy.
- Lowered aortic diastolic pressure (blood escaping into the pulmonary artery in diastole) → bounding/waterhammer pulse and widened pulse pressure.
- Coronary and splanchnic steal - reduced diastolic aortic pressure compromises coronary perfusion and gut perfusion, particularly dangerous in premature infants.
Small PDA
- Continuous flow throughout the cardiac cycle.
- No significant left heart dilation, no pulmonary hypertension, no symptoms.
- BUT - carries a risk of infectious endarteritis of ~0.45% per year after the second decade (turbulent flow damages the endothelium of the pulmonary artery opposite the ductus).
Moderate/Large PDA
- Left atrial and ventricular dilation develops.
- Pulmonary hypertension of variable degree.
- Symptoms appear progressively in the 2nd-3rd decades (dyspnea, palpitations, exercise intolerance).
- Mortality rises to 3-4% per year by the 4th decade; two-thirds of patients die by age 60 if untreated.
Eisenmenger Syndrome (~5% of isolated PDA cases)
- Sustained pulmonary hypertension causes progressive pulmonary vascular disease.
- When pulmonary vascular resistance equals or exceeds systemic resistance, the shunt reverses to right-to-left.
- Deoxygenated blood enters the descending aorta (DISTAL to the left subclavian artery) → differential cyanosis (lower extremities more cyanosed and clubbed than upper extremities and right hand).
- Goldman-Cecil Medicine, Schwartz's Principles of Surgery
6. Clinical Manifestations & Symptoms
Neonates & Infants (premature)
- Respiratory distress / failure to wean from ventilator
- Tachycardia, tachypnea
- Bounding pulses, hyperdynamic precordium
- Widened pulse pressure
- Apnea spells
- Feeding difficulties, poor weight gain
- Increased ventilator requirements
Children & Adults (uncorrected)
- Small PDA: usually asymptomatic; detected as murmur
- Moderate/Large PDA:
- Dyspnea on exertion
- Palpitations
- Exercise intolerance
- Recurrent respiratory infections
- Features of congestive heart failure (pulmonary edema, hepatomegaly)
Differential Cyanosis (Eisenmenger)
- Cyanosis and clubbing of the toes (lower extremities), while upper extremities and right hand remain normal - this is pathognomonic of Eisenmenger physiology with PDA.
7. Physical Examination Findings
| Finding | Details |
|---|---|
| Continuous "machinery" murmur | Heard at the 1st-2nd left intercostal space below the left clavicle (infraclavicular region). Peaks at S2, continues through diastole. It is the hallmark of PDA. |
| Bounding/waterhammer pulse | Due to increased stroke volume and low diastolic BP |
| Widened pulse pressure | From aortic diastolic runoff into pulmonary artery |
| Hyperdynamic precordium | Hyperactive apical impulse from LV volume overload |
| Thrill | May be palpable at the 2nd left intercostal space |
| Differential cyanosis/clubbing | Toes > fingers (Eisenmenger physiology) |
Note on murmur changes with pulmonary hypertension: As pulmonary pressure rises, the diastolic component of the murmur shortens progressively. With full Eisenmenger physiology, the entire murmur may disappear, replaced by signs of pulmonary hypertension (loud P2, etc.).
8. Investigations & Diagnosis
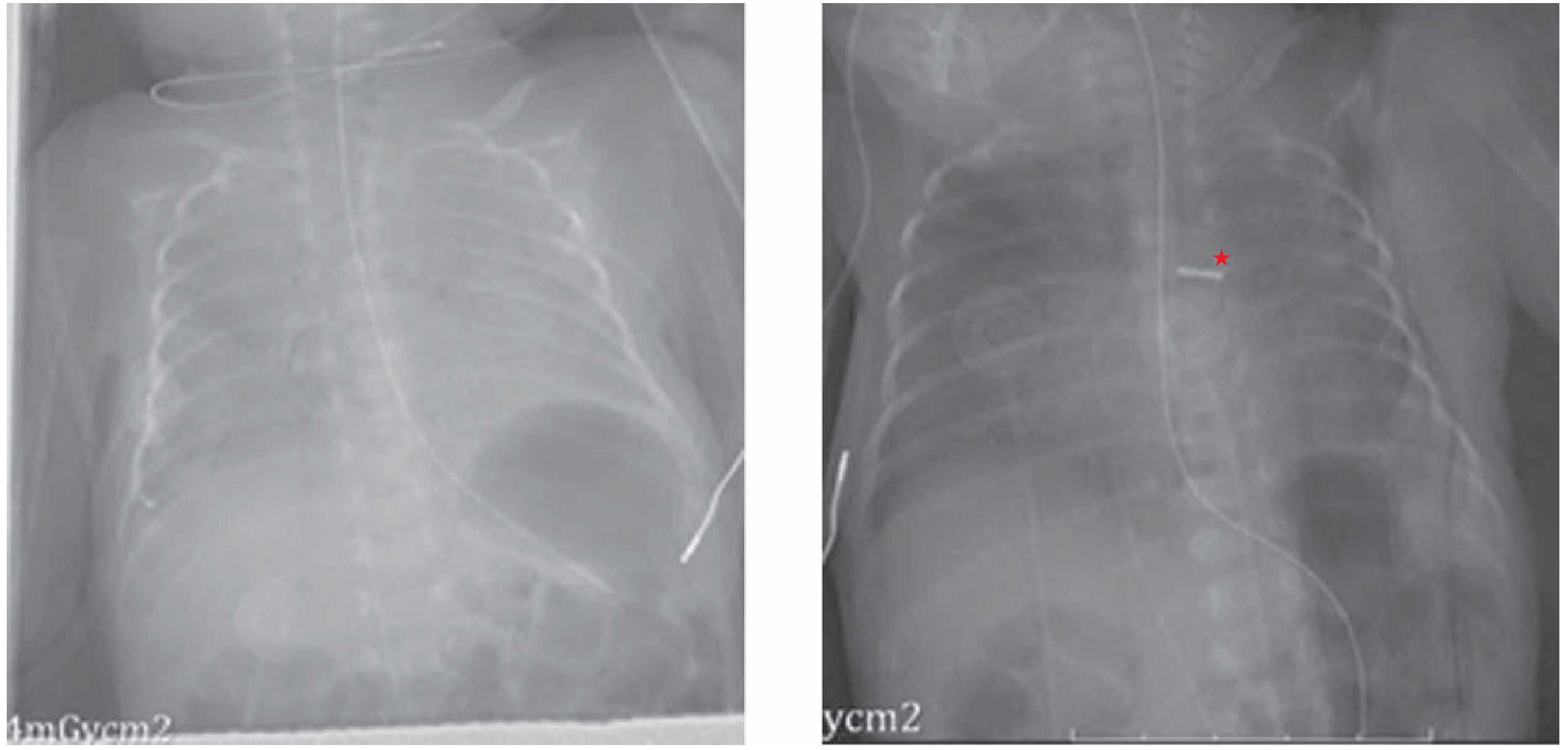
Chest X-Ray (CXR)
- Increased pulmonary vascular markings (pulmonary plethora)
- Cardiomegaly (left-sided enlargement)
- Dilated ascending aorta and pulmonary artery trunk
- In older patients: calcification at the site of the PDA
Electrocardiogram (ECG)
- Left ventricular strain pattern
- Left atrial enlargement (broad, notched P waves)
- Right ventricular hypertrophy if pulmonary hypertension has developed
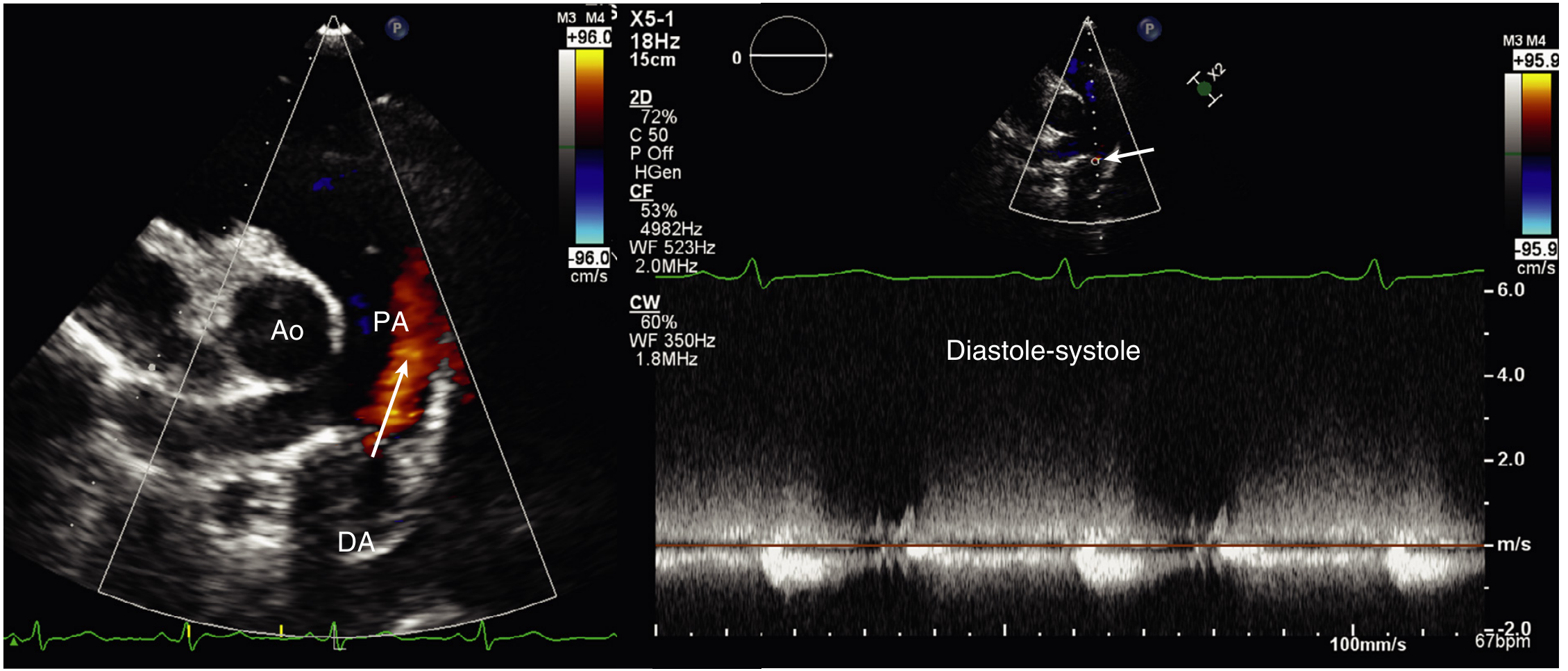
Echocardiography (Primary Diagnostic Tool)
- 2D echo: may directly visualize the ductus (easier in neonates; harder in adults due to limited acoustic window).
- Color Doppler: detects the characteristic continuous, turbulent flow jet entering the pulmonary artery from the aorta. Sensitivity 96%, specificity 100% for PDA diagnosis.
- Left atrial and left ventricular dilation (volume overload markers).
- Suprasternal notch Doppler: holodiastolic flow reversal in the descending aorta (blood flowing antegrade into ductus in diastole).
- LA:Ao ratio >1.4 suggests significant left-to-right shunt.
Cardiac Catheterization
- Not routinely needed for diagnosis.
- Indicated when pulmonary hypertension is suspected - to measure pulmonary vascular resistance and assess reversibility (determines if closure is safe).
- Step-up in oxygen saturation at the pulmonary artery level (compared to RV) confirms left-to-right shunting.
- Contraindicated in established Eisenmenger syndrome.
CT Angiography / MRI
- Used when echocardiographic windows are poor.
- CT angiography can directly visualize the ductus and assess pulmonary vasculature.
- Goldman-Cecil Medicine, Textbook of Clinical Echocardiography, Schwartz's Principles of Surgery
9. Treatment
General Principles
- The presence of a persistent PDA is itself a sufficient indication for closure (risk of endocarditis, CHF, pulmonary hypertension).
- Exception: Eisenmenger syndrome - closure is CONTRAINDICATED (would remove the "pop-off valve" for the right ventricle).
- In duct-dependent congenital lesions (e.g., pulmonary atresia, critical coarctation), the ductus must be kept open with prostaglandin E1 (PGE1) infusion until corrective surgery.
A. Pharmacologic Closure (Premature Infants Only)
Cyclo-oxygenase (COX) inhibitors block prostaglandin synthesis, removing the main vasodilatory stimulus on the ductal smooth muscle.
| Drug | Notes |
|---|---|
| Indomethacin (IV) | First-line in premature infants. Multiple dosing regimens. Effective but has side effects (renal insufficiency, necrotizing enterocolitis, platelet dysfunction). |
| Ibuprofen (IV or oral) | Comparable efficacy to indomethacin with fewer renal side effects. Ibuprofen may accelerate closure but may not reduce the need for procedural intervention in all cases. |
| Acetaminophen (paracetamol) | Increasingly used as an alternative with fewer GI and renal side effects. Acts via a different mechanism (inhibits prostaglandin peroxidase). |
Term infants are generally unresponsive to pharmacologic therapy and require mechanical/procedural closure.
Contraindications to pharmacologic therapy:
- Necrotizing enterocolitis
- Renal insufficiency / oliguria
- Active bleeding (especially intraventricular hemorrhage)
- Thrombocytopenia
- Hyperbilirubinemia (indomethacin displaces bilirubin)
B. Transcatheter (Percutaneous) Device Closure
Now the preferred treatment for most children and adults (symptomatic or after infancy).
Devices used:
- Gianturco coils - for small PDAs (<3 mm). Coil occlusion.
- Rashkind double-umbrella device - older technique, still used.
- Amplatzer Duct Occluder (ADO) - most widely used today; delivered via a femoral vein or artery catheter.
- Piccolo Occluder - for very small/premature infants.
Advantages: Avoids surgery, shorter recovery, excellent results in experienced centers.
Complications: Thromboembolism, incomplete occlusion (residual shunt 0.5-8% depending on device), device embolization, vascular injury, endocarditis, hemorrhage from perforation.
Limitations: Not applicable in very premature/small infants due to vessel access size constraints.
C. Surgical Closure
Indicated when:
- Transcatheter approach is not feasible (very premature, large ductus with complex anatomy)
- Failed device closure
- Associated cardiac defects requiring open surgery
Techniques:
- Ligation - single ligature with surgical clip or permanent suture. Approach via left posterior-lateral thoracotomy (3rd or 4th intercostal space), with lung retracted anteriorly.
- Division with oversewing - used when the ductus is short and broad (width approaches length). Both ends oversewn between vascular clamps.
- Video-Assisted Thoracoscopic Surgery (VATS) - metal clip ligation via thoracoscope. Few advantages over open in most centers.
- Median sternotomy - reserved for patients needing simultaneous repair of additional cardiac lesions.
Key anatomic hazard: The recurrent laryngeal nerve loops around the PDA and must be identified and protected to avoid left vocal cord paralysis.
Outcomes:
- Operative mortality: <1% in uncomplicated cases; up to 8% with severe pulmonary hypertension or calcification.
- After ligation in infancy/early childhood, cardiac function is typically normal and no special follow-up is required.
- Schwartz's Principles of Surgery, Goldman-Cecil Medicine
10. Complications of Untreated PDA
| Complication | Details |
|---|---|
| Congestive Heart Failure | Leading cause of death in untreated PDA (30% estimated mortality in isolated untreated PDA) |
| Pulmonary Hypertension | Progressive pulmonary vascular disease |
| Eisenmenger Syndrome | Occurs in ~5% of isolated PDA; shunt reversal, irreversible |
| Infective Endarteritis | ~0.45% per year; turbulent jet damages pulmonary artery endothelium; more common with small PDAs |
| Recurrent Respiratory Infections | From pulmonary congestion |
| Failure to thrive | Particularly in infants |
| Aneurysm of ductus | Rare; can occur in older unrepaired patients or as a complication of closure |
11. Special Situations
PDA in Premature Infants
- Near-universal in very premature neonates (≤28 weeks, <1750 g).
- Manifests as respiratory failure, inability to wean from ventilator, hypotension, metabolic acidosis.
- Conservative management (fluid restriction, diuretics) may be tried first.
- Pharmacologic closure with indomethacin or ibuprofen is first-line if no contraindications.
- Surgical ligation if pharmacologic therapy fails or is contraindicated.
PDA as a Lifesaving Channel (Duct-Dependent Lesions)
In certain complex CHDs, either pulmonary or systemic circulation depends entirely on the ductus:
- Pulmonary atresia, critical pulmonary stenosis - ductus is the only source of pulmonary blood flow.
- Hypoplastic left heart syndrome, critical aortic stenosis, critical coarctation - ductus maintains systemic perfusion.
- These patients require IV prostaglandin E1 (PGE1/alprostadil) infusion to keep the ductus open until surgical/interventional palliation.
PDA in Adults
- Often discovered incidentally or presents with exertional dyspnea, palpitations.
- Continuous machinery murmur is the hallmark.
- Older patients may show calcification of the ductus on chest X-ray.
- Transcatheter closure is well-established and effective in adults.
- Eisenmenger physiology must be excluded before proceeding with closure.
12. Classification / Types of PDA
Krichenko classification (by angiographic morphology):
- Type A (conical) - most common; funnel-shaped, narrow at pulmonary end.
- Type B (window) - short, broad ductus.
- Type C (tubular) - uniform caliber, no constriction.
- Type D (complex) - multiple constrictions.
- Type E (elongated) - long, tortuous ductus, usually in older patients.
13. Prognosis
- Small PDA that is closed early: excellent prognosis, normal life expectancy.
- Untreated moderate/large PDA: 3-4% annual mortality by the 4th decade; two-thirds of patients die by age 60.
- Estimated overall death rate for untreated isolated PDA: ~30% (primarily CHF and respiratory infections).
- Eisenmenger physiology: poor prognosis, median survival into 30s-40s; closure contraindicated.
- Post-closure in Eisenmenger: mortality may worsen acutely (right ventricular decompensation without the pulmonary "pop-off").
14. Key Summary Table
| Feature | Detail |
|---|---|
| Embryologic origin | 6th aortic arch |
| Normal closure | Functional: 10-15 hrs; Anatomic: weeks-months |
| Trigger for closure | Rising O2 tension (primary), fall in prostaglandins |
| Incidence | 1:2000 births (term); up to 75% at 28-30 weeks |
| Sex ratio | F:M = 2:1 |
| Classic murmur | Continuous "machinery" murmur, left infraclavicular |
| Shunt direction | L→R (aorta to pulmonary artery) initially |
| Best diagnostic test | Color Doppler echocardiography (96% sensitivity, 100% specificity) |
| Pharmacologic closure | Indomethacin / Ibuprofen / Paracetamol (premature infants only) |
| Preferred closure | Transcatheter device (Amplatzer, coil) |
| Surgery | Ligation or division; left thoracotomy |
| Key complication | CHF, pulmonary HTN, Eisenmenger, endarteritis |
| Differential cyanosis | Toes > fingers = pathognomonic of Eisenmenger + PDA |
| Eisenmenger closure | CONTRAINDICATED |
Sources:
- Schwartz's Principles of Surgery, 11th Edition, pp. 787-788
- Goldman-Cecil Medicine International Edition, pp. 611-612
- Robbins & Kumar Basic Pathology, p. 259
- The Developing Human - Clinically Oriented Embryology, pp. 881-882
- Textbook of Clinical Echocardiography, p. 548
This is a shared conversation. Sign in to Orris to start your own chat.