32 year old women feeling giddiness . Stirring of head around 45 to 90 degree rotating head. Couldn’t lay down, and stand , nausea , 1 episode of vomiting , since 3 hours
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
I now have comprehensive information to give a thorough clinical response. Let me compile the full answer.
Clinical Assessment: 32-Year-Old Female with Positional Giddiness
Most Likely Diagnosis: Benign Paroxysmal Positional Vertigo (BPPV)
The presentation is classic:
- Vertigo triggered by head rotation (45-90 degree head movement)
- Difficulty lying down and standing (positional provocation)
- Nausea and vomiting (autonomic accompaniment)
- Acute onset, 3-hour duration
- Young woman (BPPV affects all ages, more common in women)
Pathophysiology
BPPV occurs due to canalolithiasis - free-floating otoconia (calcium carbonate crystals) that detach from the utricle and migrate into a semicircular canal (most commonly the posterior semicircular canal). Head movement sets these canaliths in motion, causing endolymph turbulence and abnormal deflection of the cupula, generating the sensation of vertigo.
- K.J. Lee's Essential Otolaryngology, p. 355
Diagnostic Criteria (Evidence-Based)
The following 4 criteria together have 88% sensitivity, 92% specificity (LR+ 11, LR- 0.13) for BPPV:
- Recurrent vertigo
- Duration of each attack < 1 minute
- Symptoms invariably provoked by changing head position (lying down, turning in bed, reclining, bending forward)
- Not attributable to another disorder
- Symptom to Diagnosis: An Evidence Based Guide, 4th Ed., p. 268
Confirm Diagnosis at Bedside: Dix-Hallpike Maneuver
Perform the Dix-Hallpike test: Move the patient from sitting to recumbent with the head tilted 30-45 degrees over the end of the table and 30-45 degrees to one side (test each ear separately).
Positive findings for BPPV (peripheral):
| Feature | BPPV (Peripheral) |
|---|---|
| Latency | 2-5 seconds |
| Duration of nystagmus | < 30 seconds (usually < 15 s) |
| Character | Mixed rotational-upward beating |
| Fatigue on repetition | Yes - fades after 3-4 repetitions |
| Direction on sitting up | Reverses |
- Adams and Victor's Principles of Neurology, 12th Ed., p. 353-354
- Symptom to Diagnosis, p. 268
Red Flags - Rule Out Central Cause
This patient MUST be evaluated for central vertigo (posterior circulation stroke/TIA) if any of the following are present:
- Nystagmus starts immediately (no latency), lasts > 1 minute, or does not fatigue
- Pure vertical nystagmus (not suppressed by fixation)
- Focal neurological signs (diplopia, dysphagia, dysarthria, limb ataxia, facial numbness)
- Severe unsteadiness - unable to sit or walk at all
- New severe headache ("thunderclap")
- Negative head impulse test (HINTS exam)
If red flags are present: Neurology consult + urgent MRI brain (MRI > CT for posterior fossa).
Management Algorithm
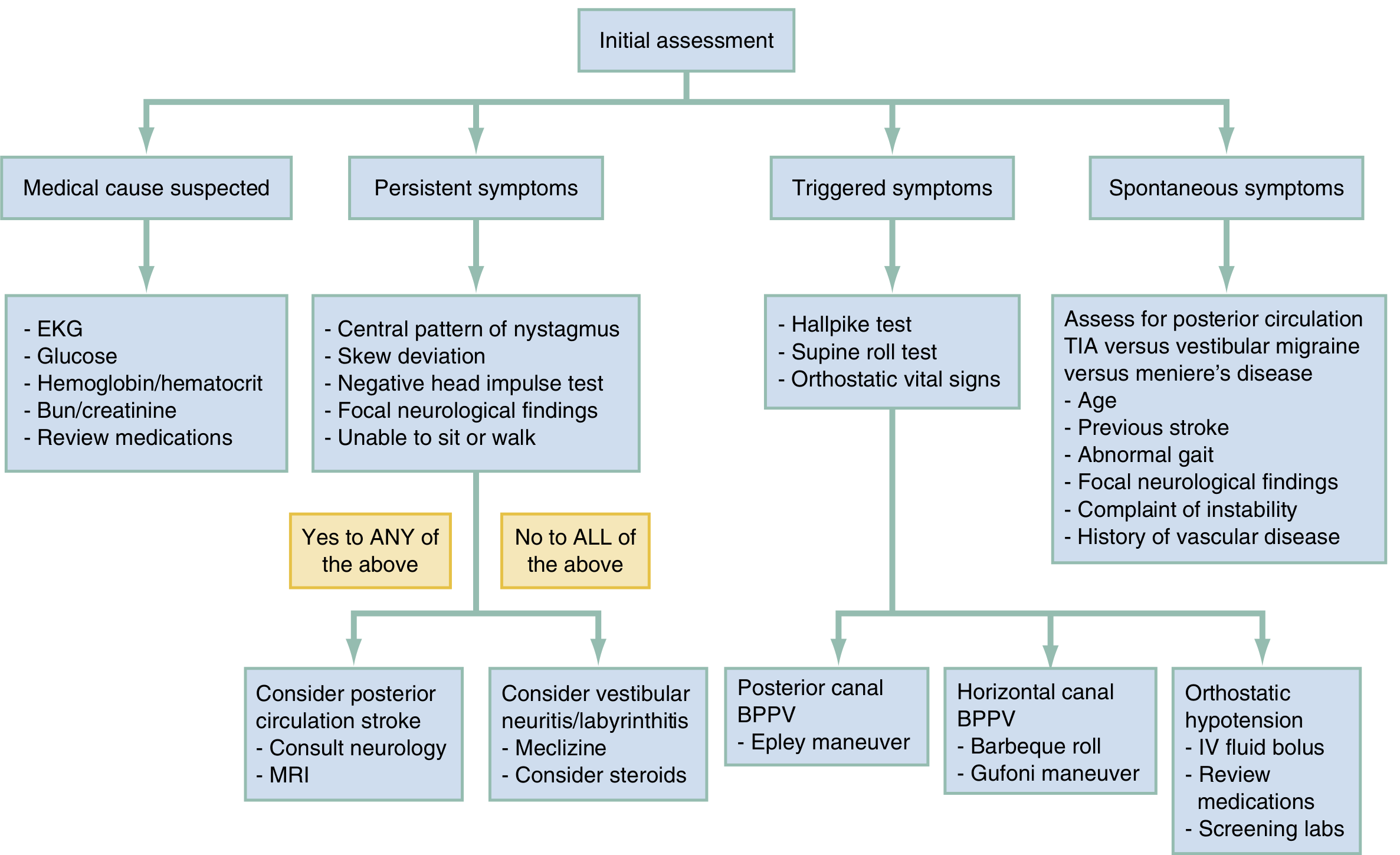
For this patient (triggered symptoms, no red flags):
1. Canalith Repositioning - Epley Maneuver (First-line)
- Involves 4-5 sequential head rotations, each held ~30 seconds (or until nystagmus/vertigo resolves)
- Effective in ~56-80% of patients with posterior canal BPPV
- Modified Epley reported up to 96.7% efficacy in some series
- The affected (dysfunctional) ear is the one that is downward when vertigo is elicited on Dix-Hallpike
A demonstration of both the Dix-Hallpike and Epley maneuvers:
2. Vestibular Suppressants (Symptomatic Relief)
- Since this patient is actively vomiting and cannot tolerate repositioning maneuvers, short-term vestibular suppressants are appropriate:
- Prochlorperazine (antiemetic/vestibular suppressant) - IV/IM for acute vomiting
- Meclizine (Antivert) - oral antihistamine
- Benzodiazepines (e.g., diazepam) - short-term only
- Caution: These drugs delay central CNS adaptation and should not be used long-term. They also worsen imbalance.
- Rosen's Emergency Medicine, p. 192
3. After Acute Episode
- Brandt-Daroff exercises - habituation exercises the patient can perform at home
- Semont liberatory maneuver - alternative to Epley
- Horizontal canal BPPV (if Dix-Hallpike negative): "Barbecue roll" or Gufoni maneuver
Differential Diagnosis to Consider
| Disorder | Duration of Vertigo | Key Distinguishing Feature |
|---|---|---|
| BPPV (most likely) | Seconds (< 1 min) | Purely positional, no hearing loss, fatigable nystagmus |
| Vestibular neuritis | Days to weeks | Spontaneous, continuous vertigo; no hearing loss |
| Meniere's disease | Minutes to hours | Fluctuant sensorineural hearing loss, tinnitus, aural fullness |
| Cerebellar/brainstem stroke | Constant/progressive | Neurological signs, cannot walk, no fatigue of nystagmus |
| Vestibular migraine | Variable | Headache history, migrainous features |
- K.J. Lee's Essential Otolaryngology, p. 356
Natural History
Most cases of BPPV resolve spontaneously within 2-6 weeks (sometimes months). About half of patients have recurrent clusters. Surgical options (posterior canal occlusion, singular neurectomy) exist for refractory cases but are rarely needed.
Summary of Immediate Action Plan
- Neurological exam - rule out focal deficits (HINTS exam if continuous vertigo)
- Dix-Hallpike maneuver - confirm BPPV, identify affected ear
- IV/IM antiemetic (prochlorperazine or ondansetron) for active vomiting
- Epley maneuver once patient can tolerate it
- If atypical features or unable to walk - MRI brain to exclude posterior fossa lesion
- Reassure and follow up; prescribe home Brandt-Daroff exercises on discharge
This is a shared conversation. Sign in to Orris to start your own chat.