
IMG_20260523_105923.jpg
Explain me this
Reading File
Finding Sources
Searching the Web
PImax PEmax respiratory muscle strength test interpretation reduced values
Reading File
Reading File
This is a respiratory muscle strength test report. Here is a full breakdown:
What This Test Measures
The test measures two pressures:
- PImax (Maximal Inspiratory Pressure) - the maximum pressure the breathing-in muscles (mainly the diaphragm and external intercostals) can generate. The patient exhales fully to residual volume, then inhales against a blocked airway as hard as possible.
- PEmax (Maximal Expiratory Pressure) - the maximum pressure the breathing-out muscles (abdominal muscles, internal intercostals) can generate. The patient inhales fully to total lung capacity, then exhales as forcefully as possible.
Together, these values directly reflect respiratory muscle strength - independent of lung mechanics. They are particularly important for detecting weakness from neuromuscular disease, as spirometry can be normal even when muscles are weak.
Reading Your Results
| Measurement | Predicted (normal) | Actual (Pre) | % of Predicted |
|---|---|---|---|
| PImax | 11.44 kPa | 4.57 kPa | 40% |
| PEmax | 9.21 kPa | 3.94 kPa | 42.8% |
- Both values are severely reduced - only about 40-43% of what is expected for this patient's age/sex/height.
- Normal PImax is typically more negative than -75 cmH2O (~7.5 kPa); this patient's value is only ~4.57 kPa.
- Normal PEmax is typically >125 cmH2O (~12.5 kPa); this patient's value is only ~3.94 kPa.
The Graphs
Both graphs (PI max and PE max) show pressure on the Y-axis (kPa) over time (seconds). The tracings rise only briefly and very low before dropping - confirming the patient could not sustain the effort, consistent with true muscle weakness.
Technical Notes from the Report
- Armspan was used to measure height - this is standard when a patient cannot stand straight (e.g., scoliosis, elderly, wheelchair users).
- Patient effort was just satisfactory; poor acceptability in PImax - the patient could only sustain the inspiratory effort for less than 2 seconds. A valid PImax requires sustaining pressure for at least 1-2 seconds. This means the PImax value may actually underestimate the true weakness (or it could reflect genuine inability to sustain effort due to weakness itself).
- No post-bronchodilator values were recorded (Post column is blank), so this was not a reversibility study.
Conclusion (as printed on the report)
"BOTH PI MAX AND PE MAX ARE REDUCED"
This means the patient has global respiratory muscle weakness - both inspiratory and expiratory muscles are affected. This pattern is typical of:
- Neuromuscular diseases (e.g., motor neuron disease/ALS, myasthenia gravis, muscular dystrophy, Guillain-Barre syndrome)
- Severe malnutrition/cachexia
- Bilateral diaphragm paralysis
- Systemic myopathy (steroid myopathy, inflammatory myopathy)
- Critical illness/prolonged ICU stay
Clinically, severely reduced PEmax (<60 cmH2O / ~6 kPa) indicates impaired cough, putting the patient at risk for secretion retention and chest infections. Severely reduced PImax suggests risk of ventilatory failure.
In short: This report shows that both the muscles responsible for breathing in and breathing out are very weak (about 40% of expected), and this should be investigated further to find an underlying cause - most importantly to rule out neuromuscular disease.
(Sources: Fishman's Pulmonary Diseases and Disorders; Goldman-Cecil Medicine, Chapter 89)
Why does it happened? What's the causes
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
This is a detailed, evidence-based answer from the textbooks. Here are all the causes of reduced PImax and PEmax, organized by category:
Why Do PImax and PEmax Become Reduced?
The respiratory muscles - like any other muscle in the body - can become weak from problems anywhere along the chain: brain → spinal cord → peripheral nerve → neuromuscular junction → the muscle itself.
1. Diseases of the Motor Neuron (Upper & Lower)
These destroy the nerve cells that send signals to breathe.
- Amyotrophic Lateral Sclerosis (ALS / Motor Neuron Disease) - the most common cause of bilateral diaphragm weakness from motor neuron disease
- Poliomyelitis - viral destruction of anterior horn cells
- Cervical spinal cord injury - cuts off nerve signals to the diaphragm (phrenic nerve originates at C3-C5)
- Cervical spondylosis - compression of the spinal cord in the neck
2. Peripheral Nerve / Phrenic Nerve Damage (Neuropathic)
The phrenic nerve directly drives the diaphragm. If it is damaged, the diaphragm goes weak or paralyzed.
- Cardiac surgery (cold cardioplegia - ice used to protect the heart can freeze and damage the phrenic nerve)
- Blunt chest/neck trauma
- Radiation injury to the chest or neck
- Lung cancer or metastatic mediastinal tumor compressing the phrenic nerve
- Guillain-Barre syndrome - autoimmune attack on peripheral nerves; tends to cause less severe weakness than motor neuron disease
- Neuralgic amyotrophy (Parsonage-Turner syndrome) - inflammatory neuritis
- Vasculitis / Mononeuritis multiplex
- Paraneoplastic syndrome (cancer releasing substances that attack nerves)
- Diabetes mellitus - causes peripheral neuropathy that can involve the phrenic nerve
3. Neuromuscular Junction Disorders
The signal from nerve to muscle fails at the connection point.
- Myasthenia gravis - autoimmune destruction of acetylcholine receptors; the muscle cannot respond even when the nerve fires
- Lambert-Eaton myasthenic syndrome (paraneoplastic)
- Organophosphate poisoning - cholinesterase inhibition causing paradoxical weakness after initial overstimulation
4. Muscle Diseases (Myopathic)
The muscle fibers themselves are diseased or destroyed.
Muscular dystrophies:
- Duchenne & Becker muscular dystrophy
- Limb-girdle muscular dystrophy
Metabolic myopathies:
- Acid maltase deficiency (Pompe disease) - often first presents as respiratory failure
- Hyperthyroidism or hypothyroidism - both can cause proximal muscle weakness
- Vitamin deficiencies (B6, B12, folate)
Inflammatory / Rheumatologic:
- Dermatomyositis / Polymyositis
- Systemic Lupus Erythematosus (SLE)
- Mixed connective tissue disease
Miscellaneous muscle causes:
- Malnutrition / cachexia - loss of muscle mass affects respiratory muscles just like limb muscles
- Amyloidosis infiltrating the muscle
5. Other Contributing Factors
- Hyperinflation (severe COPD/emphysema) - the diaphragm gets flattened by overinflated lungs and loses its mechanical advantage, reducing PImax even without true muscle disease
- Severe obesity - extra load on chest wall increases the work demand
- ICU-acquired weakness - prolonged bed rest, mechanical ventilation, and critical illness rapidly waste respiratory muscles
- Steroid myopathy - long-term corticosteroid use weakens proximal muscles including the diaphragm
Key Point: Both PImax AND PEmax Reduced Together
When both are reduced (as in your report), it strongly points to a systemic or generalized cause - affecting all respiratory muscles - rather than an isolated phrenic nerve injury (which would reduce PImax more than PEmax). The most likely categories are:
- Neuromuscular disease (ALS, myasthenia gravis, muscular dystrophy)
- Systemic myopathy (inflammatory, metabolic, rheumatologic)
- Malnutrition / severe cachexia
- Critical illness weakness
The next step after this test would typically be nerve conduction studies, EMG, blood tests (CK, thyroid, autoantibodies), and neurology referral to find the exact cause.
(Sources: Murray & Nadel's Textbook of Respiratory Medicine, Table 130.4; Fishman's Pulmonary Diseases and Disorders)
If Patient has spinal surgery
Finding Sources
Finding Sources
Searching the Web
spinal surgery reduced PImax PEmax respiratory muscle weakness mechanism
Reading File
Reading File
This is very relevant. Spinal surgery is a completely plausible explanation for this patient's low PImax and PEmax. Here is a full breakdown:
How Spinal Surgery Causes Reduced PImax & PEmax
The key is where in the spine the surgery was done. Different spinal levels affect different respiratory muscles:
The Anatomy - Which Level Controls Which Muscles
| Spinal Level | Muscles Controlled | Effect if Damaged |
|---|---|---|
| C1 - C3 | Diaphragm + ALL respiratory muscles | Complete respiratory paralysis - needs ventilator |
| C3 - C5 (phrenic nerve origin) | Diaphragm | Severely reduced PImax - may need ventilation |
| C6 - C8 / T1 - T6 | Intercostal muscles (chest expansion) | Reduced PImax + markedly reduced PEmax |
| T7 - T12 | Abdominal muscles (expiratory force) | Mainly reduced PEmax, cough impaired |
Why This Patient Fits
The report shows both PImax (40% of predicted) and PEmax (43% of predicted) severely reduced. The textbook data for spinal cord injury patients shows:
- At low cervical level: PImax ~61% predicted, PEmax ~30% predicted
- At mid-thoracic level: PImax ~69% predicted, PEmax ~32% predicted
This pattern - with PEmax often worse than PImax - is characteristic of spinal cord/spine problems because:
- PImax is reduced because the diaphragm and inspiratory muscles (scalenes, intercostals) lose some nerve supply
- PEmax is reduced even more because the abdominal muscles and internal intercostals - which drive forceful expiration and coughing - are paralyzed when the thoracic spinal cord is affected
Specific Ways Spinal Surgery Can Cause This
1. Direct nerve damage during surgery
- The phrenic nerve roots (C3-C5) can be injured during cervical spine surgery
- This directly weakens or paralyzes the diaphragm
2. Spinal cord injury / swelling post-op
- Surgical manipulation, retraction, or post-operative swelling/hematoma near the cord can functionally injure it
- Even without complete cord injury, temporary or partial dysfunction reduces muscle signals
3. Post-operative pain and splinting
- After spinal surgery, pain prevents the patient from taking deep breaths or coughing forcefully
- This contributes to poor effort - consistent with the report's note: "patient effort was just satisfactory"
4. Pre-existing cord compression (reason for surgery)
- If the patient had surgery because of cord compression (e.g. cervical myelopathy, disc prolapse, stenosis), the nerve damage may have been present before surgery
- The test may be reflecting the underlying disease, not the surgery itself
5. Intercostal and abdominal muscle denervation
- Thoracic spine surgery (T1-T12) can damage the nerve roots supplying intercostal muscles (inspiration) and abdominal muscles (expiration/cough)
- Loss of abdominal muscle function directly explains the drastically low PEmax
6. Prolonged immobility / disuse atrophy
- Post-spinal surgery patients are often immobile for weeks
- The diaphragm is sensitive to inactivity - disuse atrophy sets in rapidly, especially if the patient was also on a ventilator
The Technical Note Explains It Too
The report says "armspan was used to measure height" - this is commonly done in patients who:
- Cannot stand due to spinal pathology
- Have significant spinal deformity (scoliosis, kyphosis)
- Are wheelchair-bound from spinal cord disease
This strongly supports that this patient has significant spinal pathology or is post-spinal surgery and cannot stand upright.
Bottom Line
If this patient had spinal surgery - especially cervical or upper thoracic - reduced PImax and PEmax are a direct and expected consequence. The spine is the highway carrying all nerve signals to the breathing muscles. Damage to it, whether from the original disease or the surgery itself, cuts off those signals and the muscles weaken.
The lower the surgery level (e.g. lumbar), the less the effect on breathing. The higher the level (cervical), the more severe and life-threatening the respiratory impact.
(Sources: Fishman's Pulmonary Diseases and Disorders - Spinal Cord Injury chapter; Murray & Nadel's Respiratory Medicine)
C4 sugery level
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
C4 is the most critical level for breathing. Here is exactly why:
C4 Surgery - Direct Hit on the Breathing Nerve
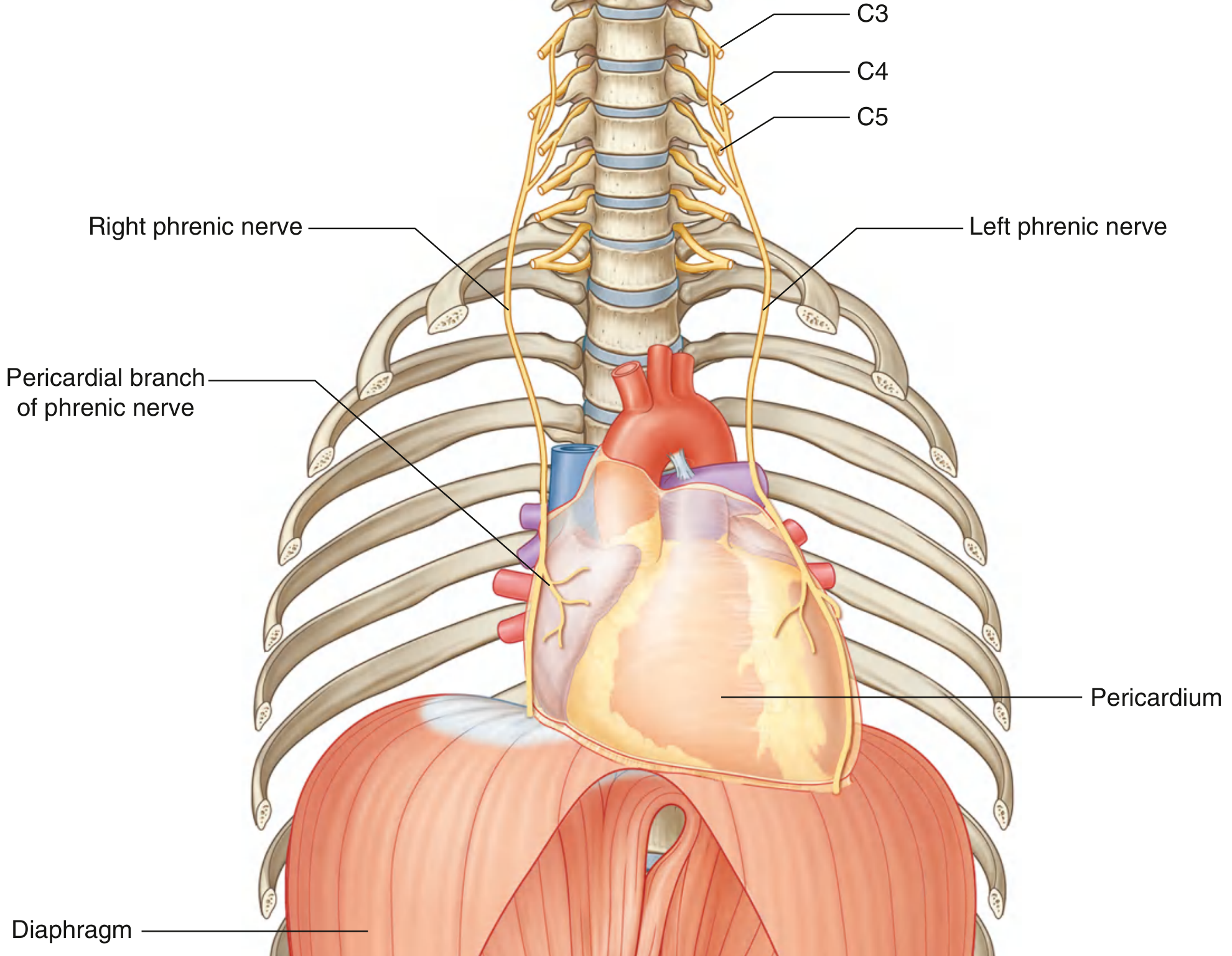
As you can see in this anatomy diagram, the phrenic nerve - the single most important nerve for breathing - is formed from C3, C4, and C5, with C4 being the dominant contribution. It travels all the way down through the chest to drive the diaphragm.
What C4 Surgery Damages
1. The Phrenic Nerve - Direct Diaphragm Weakness (PImax reduced)
Surgery at C4 is operating right at the origin of the phrenic nerve. Damage here can:
- Partially or completely interrupt the nerve signal to the diaphragm
- The diaphragm is the primary breathing muscle - responsible for 70-80% of inspiratory effort
- This directly explains why PImax is only 40% of predicted - the diaphragm simply cannot contract with full force
2. Intercostal Muscles Lost (both PImax and PEmax reduced)
At C4 level, the cord injury also means signals cannot get down to the thoracic segments (T1-T12) which supply the intercostal muscles. These muscles:
- Help expand the ribcage during inspiration (contributes to PImax)
- Help compress the chest during forced expiration (contributes to PEmax)
3. Abdominal Muscles Paralyzed (PEmax severely reduced)
Abdominal muscles (supplied by T6-T12) are completely denervated. These are the main muscles for:
- Forced expiration
- Coughing
- Generating high expiratory pressures
This is why PEmax is so low - the patient has no abdominal muscle backup for expiration.
The C4 Clinical Picture - What Happens
| Muscle Group | Level | Status After C4 Injury |
|---|---|---|
| Diaphragm | C3-C4-C5 | Partially denervated - weakened but may still work |
| Scalene/neck muscles | C3-C5 | Partially preserved - patient uses these to breathe |
| Intercostals | T1-T12 | Paralyzed |
| Abdominal muscles | T6-T12 | Paralyzed |
| Sternocleidomastoid | Cranial nerve XI | Preserved - accessory breathing muscle |
Why C4 is the "Danger Zone"
The textbook states clearly:
"Patients with C3-C4 injuries may eventually achieve at least partial ventilator independence. Lesions below C4 are usually compatible with unassisted ventilation - unless there are complicating processes."
- Above C4 (C1-C3): Complete respiratory paralysis, permanent ventilator
- At C4: Partial diaphragm function - may breathe independently but with significant weakness (exactly what this patient's test shows)
- Below C4 (C5-C8): Diaphragm largely intact, intercostals lost, PEmax affected more than PImax
This patient's result - PImax 40%, PEmax 43% - is consistent with C4 level injury, where the diaphragm is partially functioning but all the accessory inspiratory and expiratory muscles below that level are denervated.
What This Means Practically for the Patient
- Weak cough - cannot clear secretions properly, high risk of chest infections and pneumonia
- Breathless on exertion - respiratory reserve is used up just by the effort of normal breathing
- Worse when lying flat - without abdominal muscle tone, the abdominal contents push up into the chest in the supine position, compressing the lungs further
- Sleep risk - hypoventilation during sleep is common, may need nocturnal ventilation
- Any chest infection is dangerous - already at 40% capacity, any further reduction (from mucus, pneumonia) can push into respiratory failure
(Sources: Murray & Nadel's Respiratory Medicine - Cervical Spinal Cord Injury; Gray's Anatomy for Students - Innervation of the Diaphragm; Fishman's Pulmonary Diseases)
Clinical Data: T11 INCOMPLETE PARAPLEGIA (IMPROVED FROM C8 COMPLETE TETRAPLEGIA) SECONDARY TO NF THORACIC SCOLIOSIS S/P DECOMPRESSION AND POSTERIOR SPINAL FUSION C5-D8 (DOS:19/02/2020) SACRAL ULCERS
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Now I have the full picture. This is a very well-defined clinical case. Here is the complete analysis:
Full Clinical Picture - Explained
What This Patient Had
| Finding | Meaning |
|---|---|
| NF | Neurofibromatosis (Type 1) - a genetic condition causing nerve sheath tumors and skeletal deformities |
| Thoracic Scoliosis | Caused by the NF - abnormal sideways spinal curvature in the chest region |
| C8 Complete Tetraplegia | Original state - complete loss of movement and sensation from C8 level downward; all 4 limbs affected |
| Surgery: Decompression + Posterior Spinal Fusion C5-D8 | Surgically removed pressure off the cord AND fused the spine from C5 down to T8 (D8 = thoracic 8) |
| Improved to T11 Incomplete Paraplegia | After surgery, significant neurological recovery - now only legs affected, some sensation/movement preserved |
| Sacral Ulcers | Pressure sores from prolonged immobility/wheelchair use |
Why PImax and PEmax Are Reduced - Now Fully Explained
This patient has multiple simultaneous reasons for respiratory muscle weakness:
Reason 1 - Surgical Fusion Level C5 to T8
The fusion spans C5 down to T8. Looking at the muscle-level table from Murray & Nadel's:
| Respiratory Muscle | Spinal Level | Status in this Patient |
|---|---|---|
| Diaphragm | C3-C5 | Partially affected - C5 is at the edge of the fusion |
| Parasternal intercostals | T1-T7 | Denervated - fusion covers this entire range |
| Lateral external intercostals | T1-T12 | Partially denervated - T1 to T8 affected |
| Scalenes | C4-C8 | Affected - within fusion zone |
| Lateral internal intercostals (expiratory) | T1-T12 | Partially denervated - T1-T8 affected |
| Abdominal muscles (expiratory) | T7-L1 | Partially affected - T7-T8 at border of fusion |
This explains why both PImax AND PEmax are reduced - the entire zone from C5 to T8 is affected, covering nearly all the important respiratory muscles except the diaphragm (which is partially spared because C3-C4 are above the fusion).
Reason 2 - Thoracic Scoliosis from Neurofibromatosis
NF-related scoliosis (especially dystrophic NF scoliosis) is often severe and rapid. The deformed ribcage:
- Restricts chest wall expansion physically
- Creates a mechanical disadvantage for the respiratory muscles
- Reduces lung volumes (restrictive pattern)
- Even if muscles were strong, the bent cage limits how much pressure they can generate
This adds an extra mechanical handicap on top of the nerve damage.
Reason 3 - Original C8 Complete Tetraplegia (Pre-improvement)
Before improving to T11 incomplete, this patient had complete tetraplegia at C8 - meaning all intercostal and abdominal muscles were fully denervated for a period. Prolonged complete denervation causes:
- Muscle atrophy - the muscle fibers waste away
- Even after partial neurological recovery, the muscles may not have regained full strength
- Recovery of motor function after spinal cord injury is partial and incomplete in most cases
Reason 4 - Sacral Ulcers + Prolonged Immobility
Sacral pressure ulcers indicate this patient has been immobile and likely wheelchair-dependent for a significant time. This causes:
- Disuse atrophy of all muscles including respiratory muscles
- The diaphragm is especially sensitive - it weakens rapidly with inactivity
- General deconditioning reduces exercise tolerance and respiratory reserve
Why the Test Results Make Perfect Sense
PImax = 40% of predicted → Diaphragm partially preserved (C3-C4 above fusion)
but scalenes (C4-C8) and intercostals (T1-T8) lost
PEmax = 43% of predicted → Intercostal expiratory muscles (T1-T8) denervated
Abdominal muscles (T7-L1) at least partially denervated
Only pectoralis major (C5-T1) partly available for forced expiration
The fact that PImax and PEmax are roughly equal (both ~40%) actually fits a mid-cervical to upper thoracic cord lesion where both inspiratory and expiratory muscles are proportionally affected - exactly this patient's C5-T8 surgical zone.
Clinical Implications for This Patient
-
Cough is severely impaired - PEmax at 43% means mucus clearance is very poor → high risk of recurrent chest infections and pneumonia (leading cause of death in SCI patients)
-
No respiratory reserve - at 40% capacity, any additional load (infection, obesity, lying flat) can precipitate respiratory failure
-
Scoliosis compounds everything - the bent spine and ribcage mean even the remaining muscle strength is mechanically inefficient
-
Nighttime hypoventilation likely - may need to be assessed for sleep-disordered breathing or nocturnal non-invasive ventilation (NIV/BiPAP)
-
The "just satisfactory" effort noted in the test is actually typical in SCI patients - they struggle to sustain the maneuver because of genuine weakness, not just poor cooperation
-
Armspan used for height - confirms the patient cannot stand, consistent with paraplegia and spinal fusion
Summary in One Sentence
This patient's severely reduced PImax and PEmax is a direct, expected, and fully explained consequence of the spinal cord injury and fusion spanning C5-T8 - which has denervated the intercostals and scalenes while partially sparing the diaphragm - compounded by NF thoracic scoliosis restricting chest mechanics, prolonged disuse atrophy, and ongoing immobility from paraplegia.
(Sources: Murray & Nadel's Respiratory Medicine - Diseases of the Spinal Cord, Table 130.1; Fishman's Pulmonary Diseases - Spinal Cord Injury)
This is a shared conversation. Sign in to Orris to start your own chat.