Portal hypertension anatomy, causes, clinical feature
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
I now have everything needed for a comprehensive answer. Here is a complete, well-structured overview:
Portal Hypertension
Definition & Measurement
Portal hypertension is defined as a sustained elevation in portal venous pressure, clinically quantified by the hepatic venous pressure gradient (HVPG) — the difference between wedged and free hepatic venous pressure:
- Normal HVPG: ≤5 mmHg (sinusoidal pressure 3–5 mmHg)
- Portal hypertension: HVPG >5 mmHg
- Clinically significant: HVPG >10 mmHg → varices begin to form
- Threshold for ascites & variceal hemorrhage risk: HVPG >12 mmHg
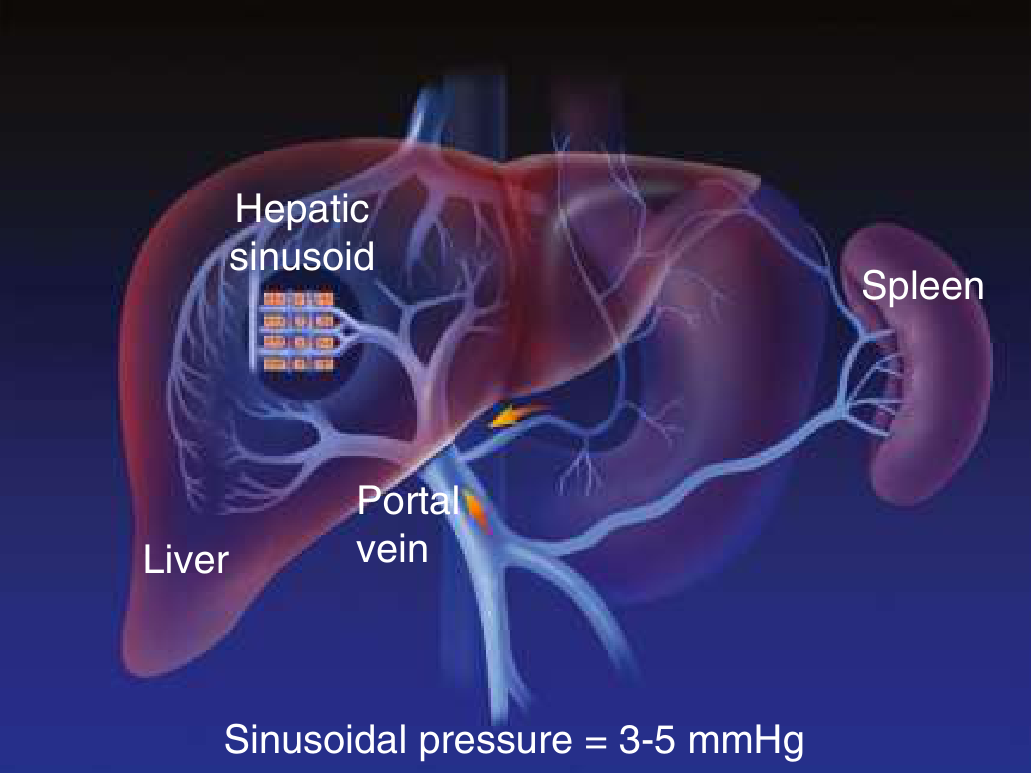
Anatomy of the Portal System
The portal vein is formed by the union of the superior mesenteric vein (SMV) and the splenic vein (the latter also receives the inferior mesenteric vein). It drains blood from the entire GI tract, spleen, and pancreas into the liver via the hepatic sinusoids, before exiting via the hepatic veins into the inferior vena cava (IVC).
Normal sinusoidal pressure = 3–5 mmHg
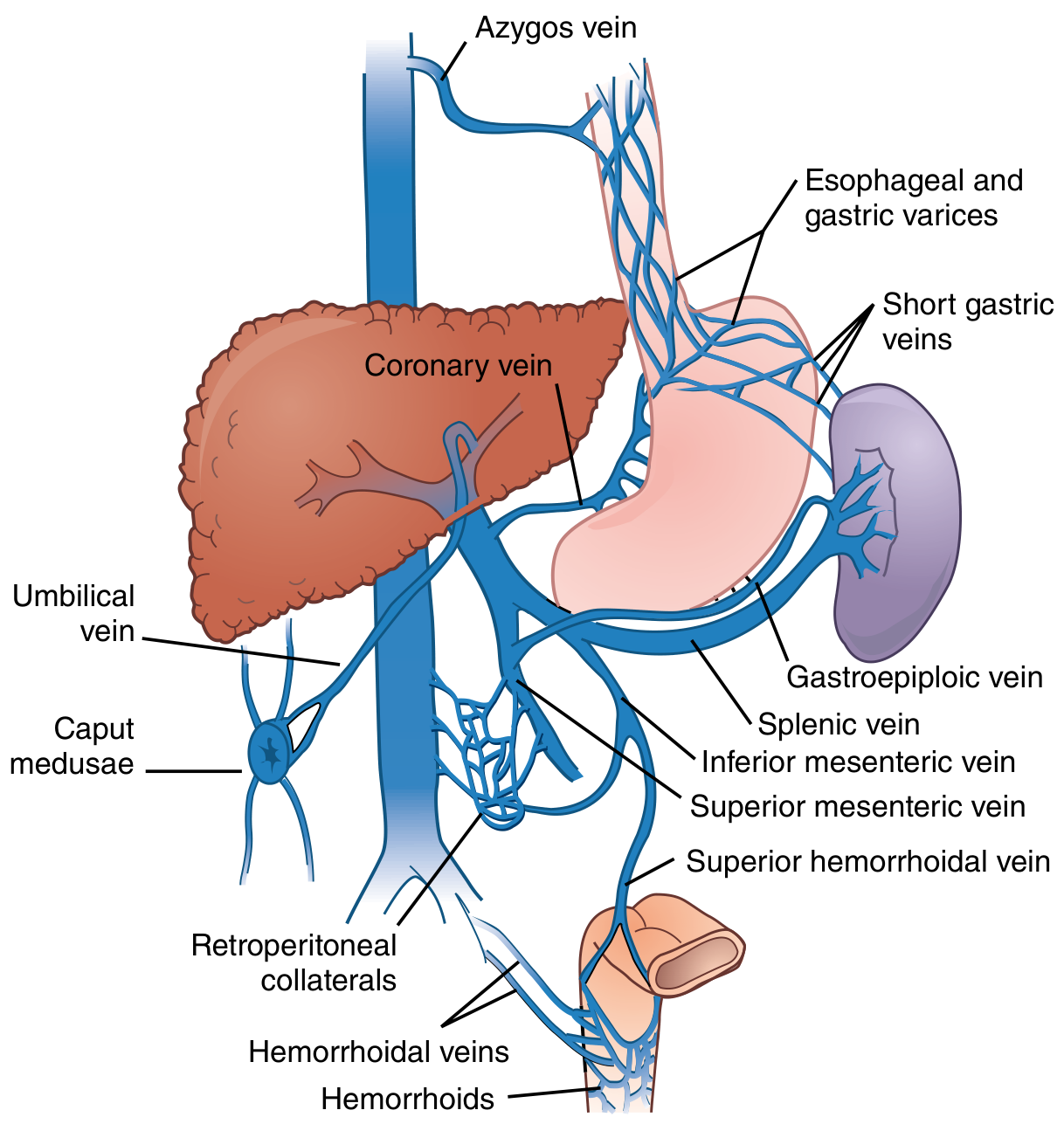
When portal pressure rises, portosystemic collaterals open at four key anatomical sites where portal and systemic venous systems are in apposition:
| Site | Collateral | Clinical Result |
|---|---|---|
| Lower esophagus/gastric cardia | Coronary/left gastric vein → azygos system | Esophageal & gastric varices |
| Umbilicus | Paraumbilical veins → epigastric veins | Caput medusae |
| Rectum | Superior hemorrhoidal vein → middle/inferior hemorrhoidals | Anorectal varices / hemorrhoids |
| Retroperitoneum | Retroperitoneal collaterals → systemic veins | Usually asymptomatic |
Pathophysiology
Portal hypertension arises from two interacting mechanisms:
1. Increased Intrahepatic Resistance
- Fixed component: Fibrosis + regenerative nodules compress sinusoids and distort hepatic veins
- Functional component: Active vasoconstriction driven by intrahepatic NO deficiency + excess endothelin/norepinephrine
2. Increased Portal Venous Inflow
As collaterals develop, splanchnic arteriolar vasodilation (paradoxically driven by excess extrahepatic NO production) increases portal blood inflow, perpetuating the hypertensive state. This causes:
- Systemic vasodilation → decreased effective arterial volume
- Activation of RAAS + sympathetic nervous system → sodium and water retention
- Hyperdynamic circulatory state (↑ cardiac output, ↓ SVR)
The NO paradox: Intrahepatic NO deficiency → vasoconstriction and ↑ resistance. Extrahepatic NO excess → splanchnic vasodilation and ↑ portal inflow. — Goldman-Cecil Medicine
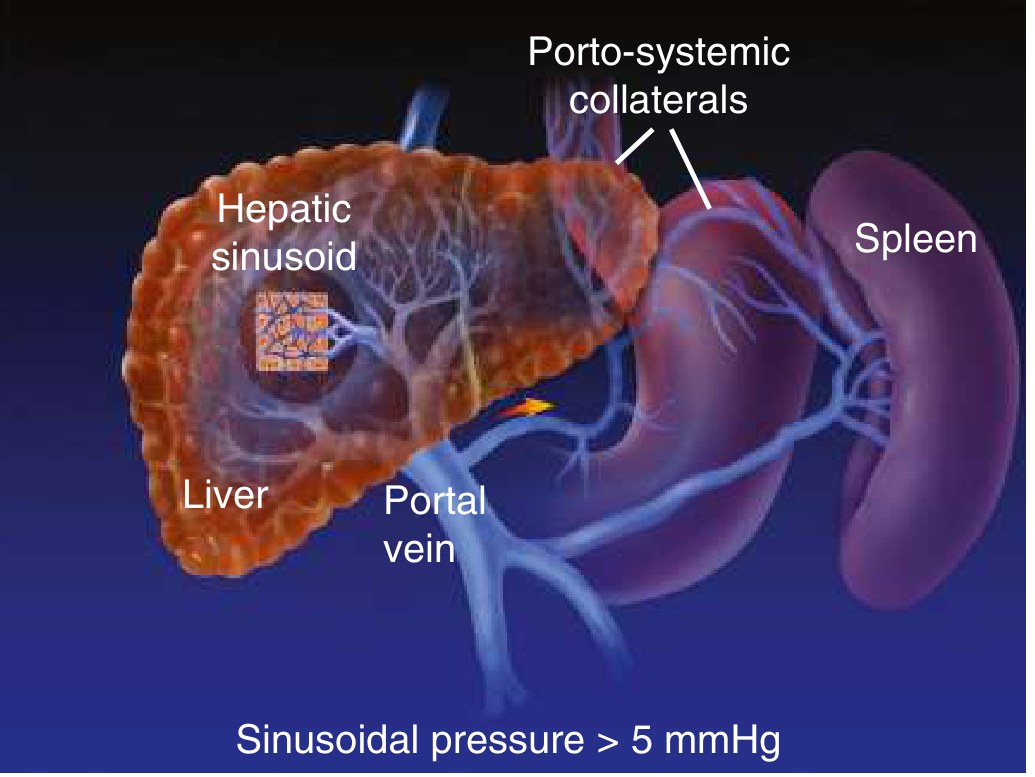
In cirrhosis, sinusoidal pressure is elevated (>5 mmHg), porto-systemic collaterals open, and the spleen enlarges:
Causes — Classified by Site of Resistance
Pre-hepatic (before liver)
- Portal vein thrombosis (PVT) — most common prehepatic cause; accounts for ~50% of portal hypertension in children
- When chronic: cavernomatous transformation of the portal vein develops
- Splenic vein thrombosis — "left-sided portal hypertension"; usually from pancreatic inflammation or neoplasm → gastric varices (not esophageal); cured by splenectomy alone
- Splanchnic arteriovenous fistula
Intrahepatic
Presinusoidal:
- Schistosomiasis (most common worldwide cause of presinusoidal portal hypertension)
- Primary biliary cholangitis, sarcoidosis
- Nodular regenerative hyperplasia
Sinusoidal (most common):
- Cirrhosis — alcoholic cirrhosis (most common cause in the US/West): collagen deposition in the space of Disse + regenerative nodules compress sinusoids
Postsinusoidal:
- Alcoholic hepatitis (perivenular fibrosis component)
- Veno-occlusive disease (sinusoidal obstruction syndrome)
Post-hepatic (after liver)
- Budd-Chiari syndrome (hepatic vein thrombosis)
- Constrictive pericarditis
- Right-sided heart failure / cardiac cirrhosis
Common vs. Less Common Summary (Sleisenger & Fordtran)
| Common | Less Common |
|---|---|
| Cirrhosis | Nodular regenerative hyperplasia |
| Schistosomiasis | Fibrocystic liver disease |
| Extrahepatic portal vein thrombosis | Sarcoidosis |
| Idiopathic portal hypertension | Malignancy |
| Cardiac fibrosis | Splanchnic arteriovenous fistula, HHT |
Clinical Features
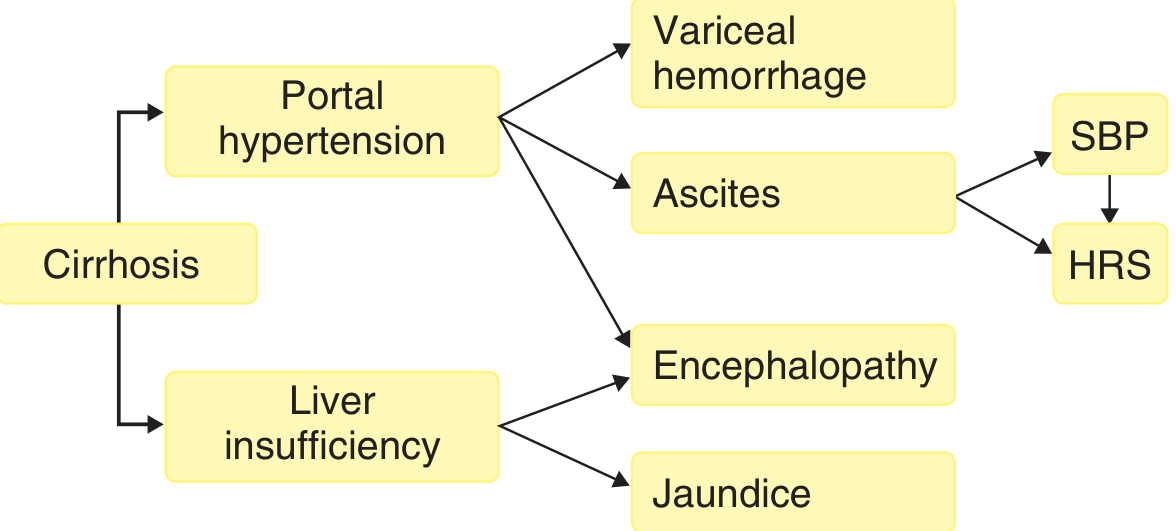
1. Gastroesophageal Varices & Variceal Hemorrhage
- Varices form when HVPG >10–12 mmHg (dilation of coronary/left gastric vein)
- Variceal rupture is the most feared complication; governed by LaPlace's law: wall tension ∝ (variceal diameter × intravariceal pressure) / wall thickness
- Presents as hematemesis or melena; massive and life-threatening
2. Ascites
- Threshold: HVPG >12 mmHg
- Mechanism: sinusoidal hypertension → hepatic lymph production exceeds thoracic duct capacity → peritoneal fluid accumulation + RAAS activation → sodium retention
- Presents as abdominal distension, shifting dullness, fluid thrill
3. Splenomegaly & Hypersplenism
- Splenic congestion → enlargement
- Sequestration of blood cells → thrombocytopenia, leukopenia, anemia
4. Caput Medusae
- Dilated periumbilical veins radiating from the umbilicus
- Represents collateral flow through the paraumbilical vein to the epigastric system
5. Anorectal Varices / Hemorrhoids
- Superior hemorrhoidal vein communicates with middle/inferior hemorrhoidal veins (systemic)
6. Portal Hypertensive Gastropathy
- Mosaic-like pattern on endoscopy; dilated submucosal vessels in the stomach → chronic blood loss
7. Hepatic Encephalopathy
- Due to both portal hypertension (portosystemic shunting) AND liver insufficiency
- Ammonia bypasses hepatic clearance via collaterals → systemic accumulation → astrocyte damage (Alzheimer type II astrocytosis)
- Clinical spectrum: subtle personality change → confusion → coma (grades I–IV)
8. Spontaneous Bacterial Peritonitis (SBP)
- Infection of ascitic fluid (without a perforated viscus)
- Mechanism: bacterial translocation from gut lumen → mesenteric lymph nodes → bacteremia → ascites colonization
- Precipitated by impaired Kupffer cell function (blood bypasses liver via collaterals)
9. Hepatorenal Syndrome (HRS)
- Progressive renal vasoconstriction secondary to extreme systemic vasodilation and RAAS activation
- Functional renal failure; oliguric with sodium-avid urine
10. Cardiopulmonary Complications
- Hepatopulmonary syndrome: pulmonary arteriolar vasodilation → intrapulmonary shunting → hypoxemia (platypnea-orthodeoxia)
- Portopulmonary hypertension: pulmonary arterial hypertension in the setting of portal hypertension
- Cirrhotic cardiomyopathy: hyperdynamic state → high-output heart failure
Key Pressure Thresholds Summary
| HVPG | Significance |
|---|---|
| >5 mmHg | Portal hypertension |
| >10 mmHg | Varices begin to form; clinically significant |
| >12 mmHg | Ascites forms; risk of variceal bleeding |
| >20 mmHg | Poor prognosis; treatment failure |
Sources: Goldman-Cecil Medicine, 26e | Sleisenger & Fordtran's Gastrointestinal and Liver Disease | Sabiston Textbook of Surgery, 21e | Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.