Contrast induced nephropathy management and prevention
Reading File
Finding Sources
Searching PubMed
"contrast induced nephropathy" prevention management
Searching the Web
contrast induced nephropathy prevention management guidelines 2024 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Contrast-Induced Nephropathy (CIN) - Management and Prevention
Terminology and Definition
The field has moved toward more precise language. Post-contrast AKI (PC-AKI) refers to any renal function deterioration within 48 hours of intravascular iodinated contrast, regardless of cause. Contrast-induced nephropathy (CIN) is a causative subset of PC-AKI where contrast is the actual culprit. The 2024 KDIGO guidelines further updated this to contrast-associated nephropathy, acknowledging that confounders (hypotension, atheroemboli, medications) often co-exist.
Quantitative definition most used: a rise in serum creatinine of ≥0.3 mg/dL or ≥25% above baseline, or urine output ≤0.5 mL/kg/h for ≥6 hours, appearing within 48 hours of contrast.
Pathophysiology
Two mechanisms drive CIN:
-
Renal vasoconstriction - Contrast triggers a biphasic hemodynamic response: brief initial vasodilation followed by prolonged vasoconstriction. Medullary hypoxia worsens due to increased blood viscosity from contrast (reduced flow in vasa recta), and osmotic diuresis increases oxygen consumption in the thick ascending limb of the loop of Henle.
-
Direct tubular toxicity - Contrast causes epithelial cell injury with generation of reactive oxygen species (ROS), evidenced by low-molecular-weight proteinuria indicating proximal tubular damage. The polyol-fructokinase pathway activation and uricosuria also contribute. - Comprehensive Clinical Nephrology, 7th Ed.
Risk Factors
| Category | Specific Factors |
|---|---|
| Renal | Pre-existing CKD (most important), eGFR <45 mL/min/1.73 m² |
| Cardiovascular | CHF, reduced cardiac output |
| Metabolic | Diabetes (especially diabetic nephropathy), hyperuricemia |
| Demographic | Age >75 years |
| Volume-related | Volume depletion, hypotension, concurrent diuretic use |
| Contrast-related | High-osmolar agents, large contrast volume, repeated contrast within 48-72 h |
| Drug interactions | NSAIDs, ACE inhibitors/ARBs, aminoglycosides, metformin |
Intraarterial contrast (e.g., cardiac catheterization, renal angiography) poses greater risk than intravenous contrast because higher doses are delivered directly to the renal circulation.
How Real is the Risk?
Importantly, recent evidence has questioned how often "CIN" is truly causative. Well-matched propensity studies show that IV contrast CT in patients with eGFR >30 mL/min/1.73 m² carries minimal independent AKI risk - rates are comparable to matched patients receiving non-contrast CT. The original studies often used high-osmolarity agents in under-hydrated populations, overstating true risk. That said, intra-arterial delivery and eGFR <45 mL/min/1.73 m² remain genuinely higher-risk scenarios. - Brenner & Rector's The Kidney, p.1071
Prevention
1. Risk Stratification Before Contrast
- Measure or estimate GFR in all patients before contrast administration
- Assess for modifiable risk factors (volume status, nephrotoxic drug use)
- Consider alternative imaging (ultrasound, non-contrast CT, MRI) in high-risk patients
Thresholds for concern:
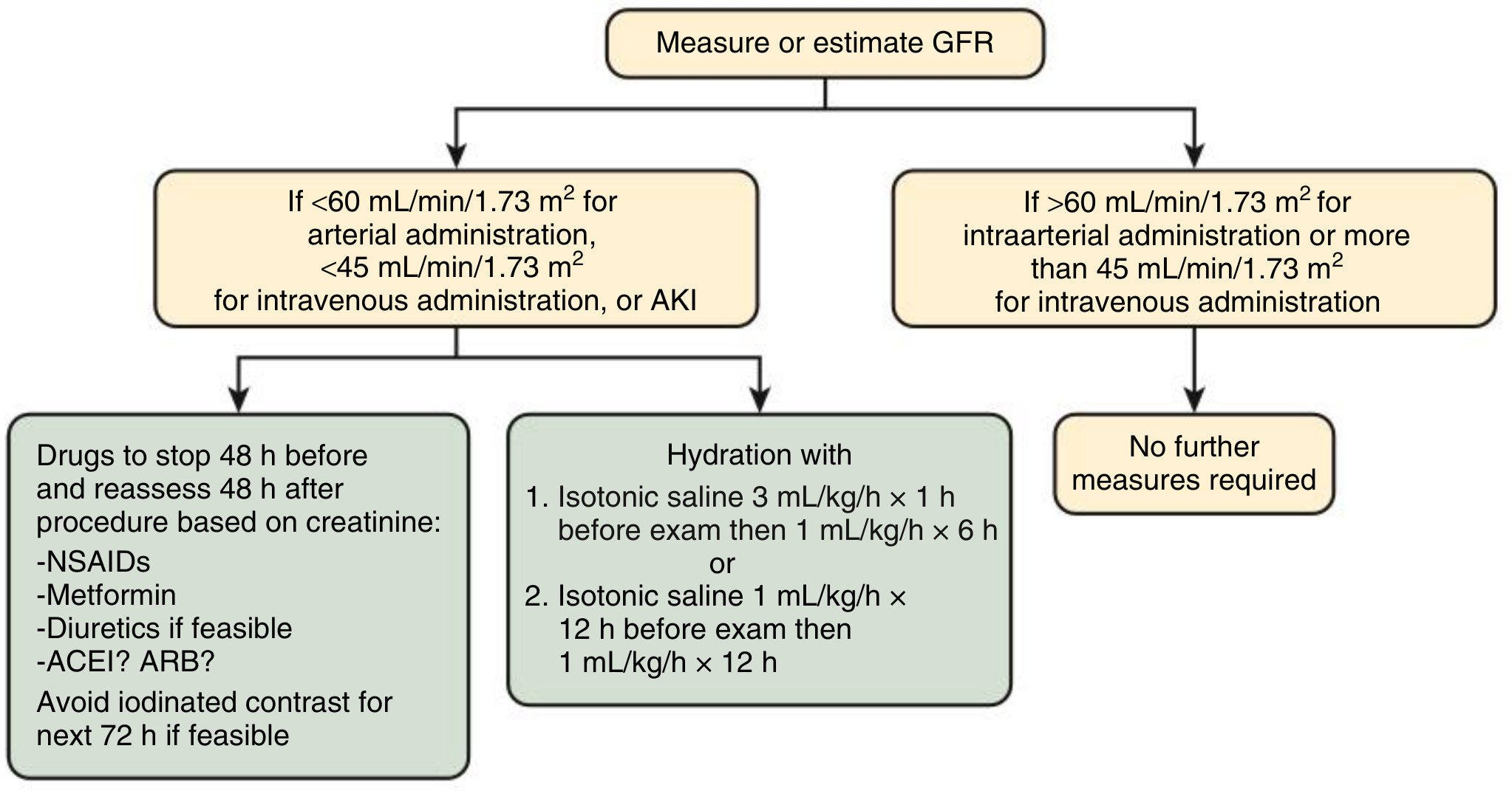
- IV contrast: eGFR <45 mL/min/1.73 m²
- Intraarterial contrast: eGFR <60 mL/min/1.73 m²
The management flowchart from Comprehensive Clinical Nephrology, 7th Ed. summarizes this clearly:
2. IV Hydration / Volume Expansion
The most evidence-supported preventive intervention. Volume expansion improves renal blood flow, dilutes contrast in tubules, and suppresses the RAAS.
Preferred regimen (KDIGO/ESC/EACTS):
- Protocol A: Isotonic saline 3 mL/kg/h for 1 hour before, then 1 mL/kg/h for 6 hours after
- Protocol B: Isotonic saline 1 mL/kg/h for 12 hours before and 12 hours after
Isotonic saline vs. sodium bicarbonate: Multiple early trials suggested bicarbonate was superior (urinary alkalinization reduces free radical generation). However, the large PRESERVE trial showed no benefit of sodium bicarbonate over saline. Current guidelines (ACR 2018, PRESERVE data, UK Kidney Association) recommend isotonic sodium chloride as the standard. Sodium bicarbonate is no longer recommended as the preferred choice. - Comprehensive Clinical Nephrology, 7th Ed. p.1004
Oral vs. IV hydration: IV hydration is preferred as it ensures certainty of volume delivered. Oral hydration may be equivalent in mild CKD in outpatients (PREPARED trial), but IV is the guideline recommendation when practical.
Special consideration in heart failure: In patients with CHF, active hydration carries fluid overload risk. Consider withholding diuretics the day before/day of contrast rather than aggressive IV hydration. Delay procedure if patient is in overt heart failure until recompensated.
3. Contrast Agent Selection and Volume Minimization
- Use iso-osmolar or low-osmolar contrast agents - iodixanol (iso-osmolar, ~290 mOsm/kg) and iopamidol/iohexol (low-osmolar, 600-800 mOsm/kg) are preferred over high-osmolar agents (~2000 mOsm/kg). Studies have not clearly shown iodixanol to be superior to low-osmolar agents for IV administration.
- Minimize contrast volume - V:CrCl ratio above 3.7 independently predicts CI-AKI
- Avoid repeat contrast studies within 48-72 hours when possible
- Do not delay a necessary procedure purely for contrast concern - KDIGO guidance
4. Nephrotoxic Drug Management
Hold the following 48 hours before and reassess 48 hours after the procedure (particularly if eGFR <45 mL/min/1.73 m²):
- NSAIDs - cause intrarenal vasoconstriction
- Metformin - risk of lactic acidosis if AKI develops; UK guideline recommends holding for 48 h post-contrast and rechecking eGFR before restarting
- Diuretics - worsen volume depletion (hold if feasible)
- ACEi/ARBs - consider withholding if eGFR <40 mL/min/1.73 m²; reassess 48 h post-procedure
5. Pharmacologic Agents
| Agent | Evidence Summary |
|---|---|
| N-acetylcysteine (NAC) | Multiple conflicting RCTs and meta-analyses. PRESERVE trial showed NO benefit. UK Kidney Association gives Grade 2D: "no convincing benefit." Not routinely recommended. May lower serum creatinine without true nephroprotection. |
| Sodium bicarbonate | No longer preferred over saline (PRESERVE trial). Grade 2D against. |
| Statins (high-dose) | Emerging evidence of benefit (especially in patients undergoing PCI). Some guidelines note potential benefit; not yet universally adopted. |
| Ascorbic acid (Vitamin C) | Some small trials show benefit; insufficient data for routine use. |
| Theophylline/adenosine antagonists | Theoretical basis (blocks adenosine-mediated vasoconstriction); insufficient data. |
| Fenoldopam | Renal vasodilator; inconsistent results; not recommended routinely. |
| SGLT2 inhibitors | A 2025 meta-analysis (PMID: 41366914) suggests pre-PCI use may reduce CIN in AMI patients - emerging area of interest. |
| Nicorandil | 2025 meta-analysis (PMID: 40340567) suggests potential benefit for CIN prevention in coronary angiography patients. |
6. Special Populations
Dialysis patients (CKD-5/ESRD):
- IV contrast can still be administered; dialysis removes contrast effectively
- Prophylactic hemodialysis or hemofiltration is NOT recommended by KDIGO to prevent CIN
- Risk of fluid overload from osmotic load causing thirst is a concern
- Timing of dialysis session can be arranged to remove contrast after administration if clinically needed
Metformin:
- Hold in eGFR <30 routinely; in eGFR 30-60, hold at time of procedure and restart only after confirming stable creatinine at 48 hours
Management After CIN Develops
- Supportive care - the AKI is typically transient (creatinine peaks at 96 hours, returns to baseline in 7-10 days in most cases)
- Ensure adequate hydration - avoid further volume depletion
- Stop nephrotoxins - NSAIDs, aminoglycosides, other contrast
- Monitor renal function - check U&E at 48-72 hours post-contrast in high-risk patients
- Avoid repeat contrast for at least 72 hours after episode
- Delay reintroducing ACEi/ARB and metformin until creatinine confirms recovery
- Dialysis - reserved for patients who develop severe, persistent AKI with fluid overload, severe electrolyte disturbance, or uremic symptoms. Not used prophylactically for contrast removal.
- No specific reversal agent exists - management is entirely supportive
Summary of Recommended Preventive Strategies (Evidence-Based)
| Intervention | Recommendation |
|---|---|
| IV isotonic saline hydration | Strong (Grade 1A) - cornerstone of prevention |
| Iso/low-osmolar contrast agents | Strong - preferred over HOCM |
| Minimize contrast volume | Standard practice |
| Avoid repeat contrast <48-72 h | Standard practice |
| Hold nephrotoxic drugs | Standard practice |
| Consider alternative imaging | When clinically equivalent |
| Sodium bicarbonate instead of saline | Not recommended (PRESERVE trial) |
| N-acetylcysteine | No convincing benefit (PRESERVE trial; Grade 2D) |
| Prophylactic dialysis | Not recommended (KDIGO) |
Recent Evidence Update (2023-2025)
- SGLT2 inhibitors before PCI appear to reduce CIN risk in AMI patients per a 2025 meta-analysis [PMID 41366914] - promising but not yet standard of care
- Nicorandil shows potential benefit in coronary angiography patients [PMID 40340567]
- RenalGuard system (matched hydration system) is being evaluated for high-risk CKD patients undergoing cardiac intervention [PMID 40099270]
- The 2024 KDIGO update shifted terminology to "contrast-associated nephropathy," reflecting that causality is often uncertain
- Inorganic nitrate (NITRATE-CIN trial, Eur Heart J 2024) showed benefit in patients undergoing coronary angiography for ACS
Sources: Brenner & Rector's The Kidney (pp. 1071-1073), Comprehensive Clinical Nephrology 7th Ed. (pp. 1004-1005), UK Kidney Association CI-AKI Prevention Guidelines, KDIGO AKI Guidelines, PRESERVE trial
This is a shared conversation. Sign in to Orris to start your own chat.