Discuss the indications, indications and complication of radical neck dissection in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Searching PubMed
"neck dissection" classification complications
Searching the Web
RGUHS ENT radical neck dissection 50 marks indications contraindications complications
Reading File
Reading File
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC9442196
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching PubMed
"neck dissection" AND "recent advances" AND head neck cancer
Reading File
Finding Sources
Searching PubMed
"neck dissection" sentinel lymph node robotic endoscopic
Loading Image
Reading File
Searching PubMed
"selective neck dissection" OR "modified radical neck dissection" outcomes
RADICAL NECK DISSECTION
Indications, Contraindications and Complications
(RGUHS 50-Mark Answer)
1. INTRODUCTION AND HISTORICAL BACKGROUND
Radical Neck Dissection (RND) is the gold standard operation for cervical lymph node metastasis from head and neck cancers. It was first described by George Crile Sr. in 1906 and later popularized by Hayes Martin in 1951. All other neck dissection procedures represent modifications of this gold standard.
"The gold standard procedure is RND, which for most patients is too extensive and results in excessive morbidity. Modifications of the RND procedure have evolved..."
- Cummings Otolaryngology Head and Neck Surgery, p. 2311
2. ANATOMY AND LYMPH NODE LEVELS OF THE NECK
Lymph Node Level Classification (AHNS System)
(Scott-Brown's Otorhinolaryngology; Cummings)
| Level | Name | Surgical Boundaries | Clinical Location |
|---|---|---|---|
| Ia | Submental | Between anterior bellies of digastric, above hyoid | Submental triangle |
| Ib | Submandibular | Body of mandible, posterior belly digastric, stylohyoid | Submandibular triangle |
| IIa | Upper jugular | Skull base to hyoid; medial to accessory nerve plane | Upper jugular |
| IIb | Upper jugular | As above; accessory nerve to posterior SCM border | Upper jugular (posterior) |
| III | Mid-jugular | Hyoid to cricoid level | Mid-jugular chain |
| IV | Lower jugular | Cricoid to clavicle | Lower jugular chain |
| Va | Posterior triangle | SCM posterior border to trapezius (above cricoid) | Posterior triangle |
| Vb | Supraclavicular | SCM posterior border to trapezius (below cricoid) | Supraclavicular |
| VI | Anterior compartment | Hyoid to sternal notch, between carotid arteries | Central compartment |
| VII | Superior mediastinal | Sternal notch to innominate artery | Retrosternal |
3. CLASSIFICATION OF NECK DISSECTION
AHNS Classification System (Cummings, Scott-Brown)
NECK DISSECTION
│
├── RADICAL (RND)
│ └── En-bloc: Levels I-V + SCM + IJV + Spinal Accessory Nerve
│
├── MODIFIED RADICAL (MRND)
│ ├── Type I → Levels I-V + preserves Spinal Accessory Nerve
│ ├── Type II → Levels I-V + preserves SAN + IJV
│ └── Type III → Levels I-V + preserves SAN + IJV + SCM
│ (= Functional Neck Dissection of Bocca)
│
├── SELECTIVE (SND)
│ ├── Supraomohyoid: Levels I-III (oral cavity)
│ ├── Lateral: Levels II-IV (oropharynx, larynx, hypopharynx)
│ ├── Posterolateral: Levels II-V (cutaneous malignancies, thyroid)
│ └── Central: Level VI (thyroid, subglottic larynx)
│
└── EXTENDED RADICAL
└── RND + Additional structures
(e.g., carotid artery, hypoglossal nerve, parotid gland, mandible)
From TABLE 118.3 - American Head and Neck Society Classification (Cummings, p. 2294)
4. DEFINITION OF RADICAL NECK DISSECTION
RND involves en-bloc removal of:
- Lymph node levels I through V (ipsilateral)
- Spinal Accessory Nerve (SAN / CN XI)
- Internal Jugular Vein (IJV)
- Sternocleidomastoid Muscle (SCM)
Boundaries:
- Superior: Lower border of mandible
- Inferior: Clavicle
- Anterior: Contralateral anterior belly of digastric + lateral border of strap muscles
- Posterior: Anterior border of trapezius muscle
NOT included: Postauricular, suboccipital, periparotid, perifacial, buccinator, retropharyngeal, and paratracheal nodes.
- Cummings Otolaryngology, p. 2293
5. INDICATIONS FOR RADICAL NECK DISSECTION
A. Absolute Indications (Cummings; Dhingra; StatPearls)
- Extensive cervical lymph node metastases with extracapsular spread (ECS) involving the SAN and IJV
- N3 neck disease - massive lymph node metastasis (>6 cm)
- Disease fixed to SCM/IJV/SAN - when non-lymphatic structures are directly invaded
- Recurrent cervical metastasis after previous conservative neck dissection
- Recurrent disease after previous irradiation - particularly post-chemoradiation salvage
- Gross extranodal spread with fixation to skin or deep structures
- Involvement of platysma or skin requiring sacrifice of overlying tissue
- Recurrent NPC (Nasopharyngeal Carcinoma) with controlled primary
B. Relative Indications
- Extensive primary lesion treated surgically (N0 neck) where pedicled reconstruction flap passes through the neck (controversial)
- Primary sites with >20% risk of occult nodal metastasis where SND/MRND is not feasible
C. By Primary Site (Dhingra; Hazarika; Zakir Hussain)
| Primary Site | Preferred Neck Dissection | Notes |
|---|---|---|
| Oral cavity T3-T4, N+ | MRND/RND (Levels I-III/I-V) | RND if SAN/IJV involved |
| Oropharynx N2-N3 | MRND or RND | Bilateral if N2c |
| Larynx/Hypopharynx N2-N3 | MRND / RND | RND for fixed nodes |
| Nasopharynx recurrence | RND | Post-radiation salvage |
| Thyroid cancer (advanced) | Central + lateral SND | RND rarely needed |
| Parotid malignancy | Parotidectomy + ND | RND if N+ clinically |
D. Elective (END) vs. Therapeutic (TND) Neck Dissection
NECK DISSECTION
│
├── ELECTIVE (Prophylactic/END)
│ ├── Clinically N0 neck
│ ├── >15-20% risk of occult metastasis
│ └── T3-T4 primary tumors
│
└── THERAPEUTIC (TND)
├── Clinically N+ neck (palpable nodes)
├── Radiologically confirmed nodal disease
└── Post-chemoRT residual disease
ECS (Extracapsular Spread) found in 20% of clinically N0 necks in supraglottic cancer - an important indicator for post-operative radiotherapy.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, p. 51
6. CONTRAINDICATIONS FOR RADICAL NECK DISSECTION
A. Absolute Contraindications (Cummings; StatPearls)
- Unresectable disease:
- Invasion of the skull base
- Invasion of prevertebral musculature/fascia (scalene, levator scapulae)
- Involvement of brachial plexus or phrenic nerve
- Circumferential carotid artery encasement - patient unable to tolerate balloon occlusion test
- Distant metastatic disease (M1) - surgery won't be curative
- Uncontrolled primary tumor - neck dissection not indicated if primary cannot be controlled
- N0 neck - not an indication for RND (selective or MRND preferred)
- High surgical risk - severe cardiopulmonary disease not optimizable preoperatively
B. Relative Contraindications
- Significant carotid artery involvement (wall adherent but not encasing) - resection causes high morbidity
- Uncompensated coagulopathy
- Poor neurocognitive state
- Synchronous bilateral RND (relative) - ligation of both IJVs risks severe cerebral/facial edema, increased ICP
- Fixed neck mass in deep cervical fascia without distant metastasis (borderline resectable)
- Poor overall health / ASA IV-V
"Patients in whom preoperative imaging suggests deep infiltration of the prevertebral space, scalene muscles, levator scapula muscle, phrenic nerve, and brachial plexus should not be considered suitable candidates."
7. FLOWCHART: MANAGEMENT OF CERVICAL LYMPHADENOPATHY
Below is the Cummings Algorithm for cervical lymphadenectomy:
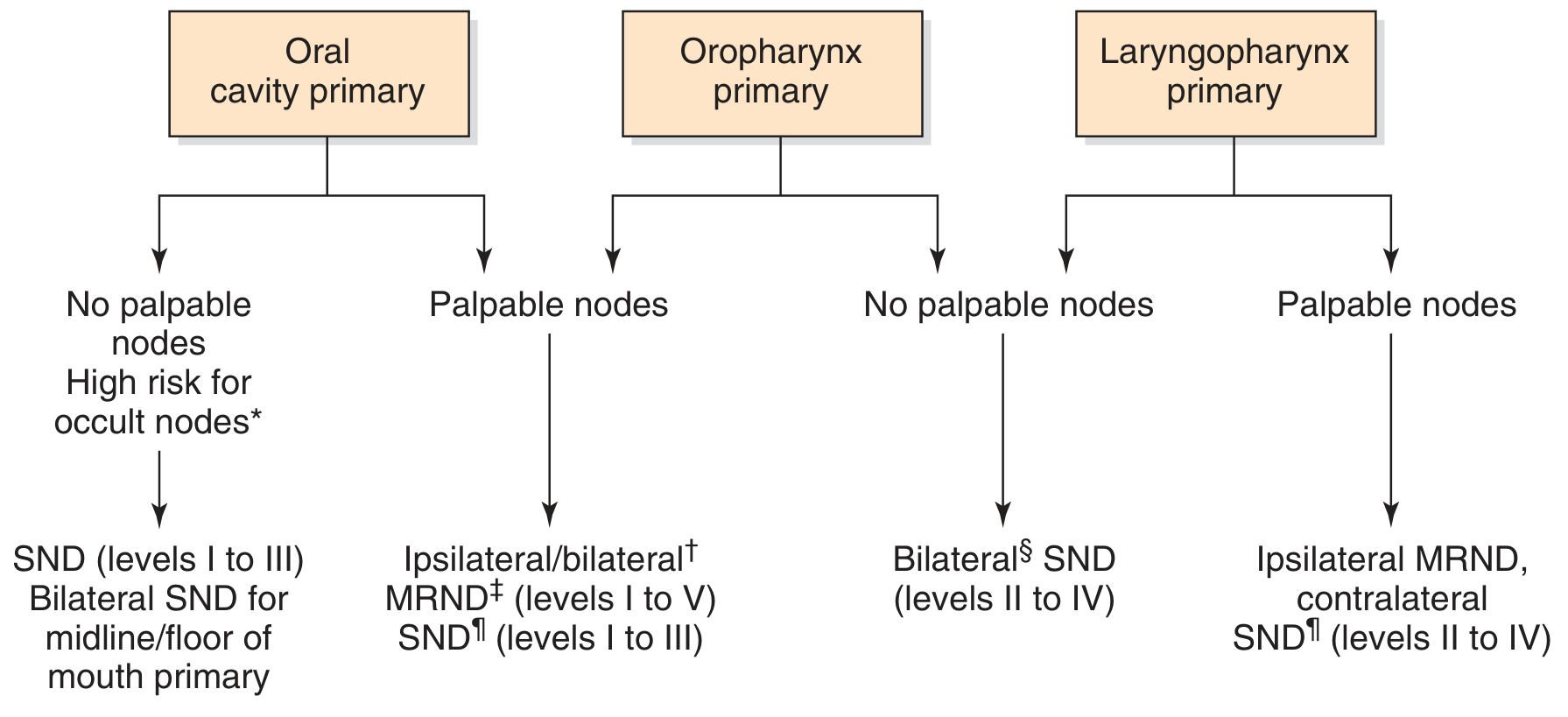
Fig. 118.18 - Algorithm for cervical lymphadenectomy options in patients with carcinomas of the upper aerodigestive tract. (Cummings Otolaryngology, p. 2311)
Additional Management Flowchart:
HEAD AND NECK MALIGNANCY WITH NECK DISEASE
│
├── Assess Primary Site + N-Stage
│
├── N0 Neck
│ ├── T1-T2, <15% occult risk → OBSERVE
│ └── T3-T4, >15-20% occult risk → ELECTIVE SND or MRND
│
└── N+ Neck
├── N1 (single node, <3 cm, no ECS) → SND or MRND
├── N2a/N2b (single/multiple ipsilateral) → MRND (I-V)
├── N2c (bilateral) → Bilateral MRND
└── N3 / Fixed / ECS / SAN-IJV involved
└── RADICAL NECK DISSECTION
├── Intraoperative SAN invasion → RND
└── Post-chemoRT persistent disease → Salvage RND
8. SURGICAL TECHNIQUE OF RND (Overview)
Positioning: Supine, shoulder roll, neck extended
Incisions (Cummings):
- Hockey stick / Boomerang - optimal for exposure + blood supply
- McFee incision - parallel horizontal incisions (better for irradiated necks)
- Apron incision - for bilateral dissections
- Avoid trifurcations over the carotid sheath
Steps:
- Raise subplatysmal flaps (superiorly and inferiorly)
- Identify and preserve marginal mandibular nerve
- Divide and ligate external jugular vein
- Dissect submandibular triangle (Level I) - ligate facial artery, submandibular duct
- Expose and divide SCM at mastoid and clavicle
- Ligate IJV superiorly (below jugular bulb) and inferiorly (above subclavian vein)
- Divide SAN at entry to SCM and at posterior triangle
- Dissect posterior triangle (Levels IV-V) - preserve phrenic nerve, brachial plexus
- Clear carotid sheath (Levels III-IV)
- Check thoracic duct area (left side) - ligate any lymphatics
- Insert drains + layered closure (platysma + skin)
9. COMPLICATIONS OF RADICAL NECK DISSECTION
A. Classification
COMPLICATIONS OF NECK DISSECTION
│
├── INTRAOPERATIVE
│ ├── Vascular: Hemorrhage from carotid/IJV
│ ├── Nerve Injury: CN VII (marginal mandibular), CN X, CN XI, CN XII
│ ├── Thoracic Duct Injury → Chyle Fistula
│ ├── Pneumothorax
│ └── Air Embolism
│
├── EARLY POSTOPERATIVE (within 72 hrs)
│ ├── Hematoma
│ ├── Air leak through drain
│ ├── Facial/Cerebral edema (bilateral RND)
│ ├── Wound infection
│ └── Chyle fistula
│
└── LATE POSTOPERATIVE
├── Carotid blowout / Rupture
├── Wound dehiscence
├── Shoulder dysfunction (SAN sacrifice)
├── Scar formation / Keloid
├── Hypothyroidism (if Level VI)
├── Lymphedema
└── Rare: Blindness, Air embolism, CVA, SIADH
B. Detailed Complications (Cummings, p. 2309-2311)
1. Hemorrhage / Hematoma
- Most common early complication
- External bleeding or subcutaneous ballooning of flaps
- Management: Early cases - "milking" drains; Established hematoma - return to OR under sterile conditions
2. Air Leaks
- Common day-after complication
- Entry via incision, displaced drains, or tracheostomy communication
- Potentially serious if contaminated secretions circulate through wound
3. Chylous Fistula (Cummings, p. 2309)
- Incidence: 1-2% of neck dissections with Level IV dissection
- Higher risk on left side (thoracic duct)
- Management:
- Low output (<600 mL/day) - Conservative: pressure dressings, low-fat diet, total parenteral nutrition
- High output (>600 mL/day) - Early surgical re-exploration and ligation
- Hemoclips or 5-0 silk suture ligatures over hemostatic sponge
4. Facial and Cerebral Edema
- Occurs with bilateral RND (both IJVs ligated)
- Dramatic facial edema from inadequate venous drainage
- Cerebral edema → increased ICP → impaired neurologic function, coma, SIADH
- Prevention: Preserve at least one external jugular vein; restrict IV fluids; monitor CVP and serum osmolarity
- Management: Fluid restriction, osmotic diuretics
5. Carotid Artery Rupture (Most feared lethal complication)
"The most feared and the most common lethal complication after surgery of the neck is the exposure and rupture of the carotid artery."
- Cummings Otolaryngology, p. 2310
- Predisposing factors: Salivary fistula, malnutrition, diabetes, infection, previous RT
- Prevention: Watertight closure of pharyngeal defects; vascularized flap coverage; "carotid precautions"
- Management:
- Manual pressure + fluid resuscitation
- Surgical ligation (preferred over repair in infected field)
- Saphenous vein graft if tolerated
- Preoperative carotid balloon occlusion test if resection planned
6. Nerve Injuries
| Nerve | Incidence | Result |
|---|---|---|
| Marginal mandibular (CN VII) | 5.5% - most common | Lower lip weakness, droop |
| Spinal accessory (CN XI) | 5.1% (intentional in RND) | Shoulder drop, winging of scapula, trapezius atrophy |
| Vagus (CN X) | Rare | Vocal cord paralysis (if below nodose ganglion); dysphagia + aspiration (if above) |
| Hypoglossal (CN XII) | Rare | Ipsilateral tongue deviation, dysarthria |
| Phrenic nerve | Uncommon | Hemidiaphragm paralysis, atelectasis |
| Sympathetic chain | Rare | Horner syndrome (ptosis, miosis, anhidrosis) |
| Lingual nerve | Very rare | Ipsilateral tongue numbness |
| Brachial plexus | Very rare | Arm weakness/numbness |
7. Wound Infection
- Incidence higher when: aerodigestive tract is entered, post-radiation field, diabetes
- "Aerodigestive tract entry is the single most important factor that contributes to risk of wound infection" (Cummings, p. 743)
- Prophylactic antibiotics indicated for contaminated procedures
8. Shoulder Dysfunction (Long-term)
- Consequence of SAN sacrifice in RND
- Trapezius muscle denervation → dropped shoulder, winging of scapula, inability to abduct arm >90°
- Chronic pain, frozen shoulder syndrome
- Physical therapy essential post-MRND (even nerve-preserving procedures cause temporary dysfunction)
9. Blindness (Rare - <5 cases reported)
- Bilateral RND only
- Intraorbital optic nerve infarction from combined hypotension + severe venous distension
- Catastrophic and irreversible
10. Rare Complications
- SIADH (Syndrome of Inappropriate ADH secretion) - bilateral IJV ligation
- Pneumothorax - apical pleural tear during Level IV dissection
- Air embolism - inadvertent venous entry
- Cerebrovascular accident - carotid manipulation/ligation
- Arteriovenous fistula - rare iatrogenic
10. SPECIFIC COMPLICATIONS FLOWCHART
POST-NECK DISSECTION MONITORING
│
├── Day 0-1: Drain output monitoring
│ ├── Milky/turbid fluid → CHYLE FISTULA
│ │ ├── >600 mL/day → Surgical re-exploration
│ │ └── <600 mL/day → Pressure dressing, low-fat diet, TPN
│ │
│ └── Serosanguinous + swelling → HEMATOMA
│ ├── Mild → Drain milking
│ └── Expanding → Return to OR
│
├── Day 1-3: Wound assessment
│ ├── Air through drain → Air Leak → Seal entry point
│ ├── Facial puffiness (bilateral RND) → Cerebral edema
│ │ └── Restrict fluids, osmotic diuretics, ICU monitoring
│ └── Fever + erythema → Wound Infection → IV antibiotics
│
├── Day 3-14: Oncological monitoring
│ ├── Fistula formation → Salivary Fistula
│ │ └── Risk factor for CAROTID RUPTURE
│ │ └── Carotid Precautions + Vascularized flap coverage
│ └── Shoulder drop → SAN injury → Physiotherapy
│
└── Long-term (months)
├── Persistent shoulder pain → Physiotherapy, TENS
├── Keloid formation → Steroid injection / Pressure garments
└── Lymphedema → Compression garment, Manual lymph drainage
11. MODIFIED RADICAL NECK DISSECTION (MRND)
Definition: En-bloc removal of Levels I-V with preservation of one or more of: SAN, IJV, SCM. (Cummings, p. 2296)
Major indication: Grossly visible lymph node disease not directly infiltrating non-lymphatic structures.
Types (Medina/Robbins Classification):
- Type I (MRND-I): Preserves SAN only
- Type II (MRND-II): Preserves SAN + IJV
- Type III (MRND-III / Functional ND): Preserves SAN + IJV + SCM - popularized by Bocca (Italy)
Rationale: Difficult to justify sacrifice of SAN if not directly involved, when hypoglossal and vagus nerves in similar proximity to nodes are spared.
12. SELECTIVE NECK DISSECTION
Definition: Neck dissection where one or more lymph node levels are preserved relative to RND.
| Type | Levels | Primary Indication |
|---|---|---|
| Supraomohyoid ND | I-III | Oral cavity cancers (N0) |
| Lateral ND | II-IV | Oropharynx, larynx, hypopharynx |
| Posterolateral ND | II-V | Cutaneous malignancies, thyroid |
| Anterior (Central) ND | VI | Thyroid, subglottic, cervical esophagus |
13. EXTENDED RADICAL NECK DISSECTION
Involves RND + removal of additional lymph node groups or non-lymphatic structures:
Additional lymph node groups: Suboccipital, retropharyngeal, parapharyngeal, parotid, facial (buccinator), Levels VI and VII
Additional non-lymphatic structures:
- Mandible
- Parotid gland
- Part of mastoid tip
- Prevertebral fascia/musculature
- Hypoglossal nerve
- External carotid artery
- Vagus nerve
- Paraspinal muscles
- Overlying skin
Indication: Primary tumor directly invading these structures combined with N+ neck disease.
14. RECENT ADVANCES (2021-2026)
A. Minimally Invasive / Endoscopic Neck Dissection (Cummings, p. 2311)
- Robotic-assisted neck dissection (RAND): Retroauricular or transaxillary approach
- Comparable lymph node yield to open procedure
- Significantly improved cosmesis (no neck scar)
- Much more expensive; technically demanding
- More suitable for upper levels (II, III)
- Endoscopically assisted neck dissection:
- Randomized controlled trial (Fan et al.) confirmed feasibility
- ~1 hour longer operative time
- No difference in lymph nodes retrieved or complication rate
- Economic advantage where surgical robot unavailable
B. Sentinel Lymph Node Biopsy (SLNB) (Scott-Brown)
- Injection of isotope around primary oral cancer
- Identifies first-echelon drainage nodes
- Increasingly used to determine whether neck dissection is needed at all in T1-T2 N0 oral SCC
- Avoids unnecessary elective neck dissection in sentinel-node-negative patients
C. FDG-PET/CT-guided Neck Management
- Planned neck dissection 6-8 weeks post-chemoradiation when residual neck disease suspected
- PET/CT reliability questionable before 3 months post-RT completion
- Landmark PETCT3 trial: PET-CT surveillance was cost-effective vs. planned neck dissection after chemoRT for advanced head and neck SCC
D. De-escalation in HPV+ Oropharyngeal Cancer
- HPV-positive oropharyngeal SCC has better prognosis
- Multiple trials exploring reduced neck dissection extent or watch-and-wait after chemoRT response
- Selective neck dissection replacing MRND for favorable N2 disease when post-op RT planned
E. Fluorescence-guided Surgery
- Near-infrared fluorescence imaging to identify lymphatic channels and sentinel nodes intraoperatively
- Reduces inadvertent thoracic duct injury and chyle fistula rates
F. Extracapsular Spread (ECS) and Adjuvant Therapy
- ECS found even in small clinically N0 nodes (20% of N0 supraglottic cancers - Scott-Brown)
- ECS + multiple positive nodes = indication for concurrent chemoradiotherapy (not just RT alone)
- RTOG 9501 / EORTC 22931: Concurrent cisplatin-based chemoRT after surgery significantly improves outcomes in ECS-positive necks
15. PROGNOSIS AND ONCOLOGICAL OUTCOMES
| Factor | Impact |
|---|---|
| Single node, no ECS | Good prognosis |
| Multiple nodes / ECS | Worse; requires adjuvant chemoRT |
| Bilateral neck disease (N2c) | Significantly worse |
| N3 (>6 cm or contralateral) | Poor; RND + chemoRT |
| Recurrent disease post-RT | Poor; salvage RND still best option |
16. SUMMARY TABLE - COMPARISON OF NECK DISSECTIONS
| Feature | RND | MRND | SND |
|---|---|---|---|
| Levels | I-V | I-V | Selected levels |
| SCM | Removed | Preserved (Type III) | Preserved |
| IJV | Removed | Preserved (Type II/III) | Preserved |
| SAN | Removed | Preserved (Types I/II/III) | Preserved |
| Morbidity | Highest | Moderate | Least |
| Indication | Fixed/ECS N3 disease | N+ without structure invasion | N0 or N1 selected |
| Shoulder dysfunction | Severe (permanent) | Mild-moderate | Minimal |
REFERENCES
- Cummings Otolaryngology Head and Neck Surgery, 7th ed. Flint PW et al. Chapter 118 - Neck Dissection. pp. 2293-2311 (Elsevier)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, 8th ed. Gleeson M et al. Neck Surgery Chapter (CRC Press)
- Dhingra PL, Dhingra S - Diseases of Ear, Nose and Throat & Head and Neck Surgery, 7th ed. Elsevier
- Hazarika P - Textbook of Ear, Nose & Throat Diseases
- Zakir Hussain - ENT for ENT (RGUHS reference)
- Stell and Maran's Head and Neck Surgery, 4th ed.
- Crile GW. On the surgical treatment of cancer of the head and neck. Trans South Surg Gynecol Assoc. 1906;19:109-127
- Robbins KT et al. Standardizing neck dissection terminology. Arch Otolaryngol Head Neck Surg. 2002
- PMC9442196 - Neck dissection complications systematic review (marginal mandibular nerve injury 5.5%, accessory nerve 5.1%)
- StatPearls - Radical Neck Dissection - Inman et al., 2026
- Li ZZ et al. Neck management in cT1-2N0 oral squamous cell carcinoma. Int J Cancer. 2025 [PMID: 40268514]
- Wei H et al. Modified Radical Neck Dissection for Cervical Metastasis. J Vis Exp. 2026 [PMID: 41801803]
RGUHS Exam Tip: For a 50-mark answer, the examiner expects:
- Definition + historical perspective (5 marks)
- Lymph node level classification with diagram (8 marks)
- Classification of neck dissections with flowchart (8 marks)
- Indications - absolute, relative, by primary site (10 marks)
- Contraindications (5 marks)
- Complications - intraoperative, early, late with flowchart (10 marks)
- Recent advances / modifications (4 marks)
This is a shared conversation. Sign in to Orris to start your own chat.