Corneal ulcer
Reading File
Finding Sources
Finding Sources
Searching PubMed
"corneal ulcer" OR "corneal infection"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have thorough information from multiple textbooks. Here is the comprehensive clinical overview:
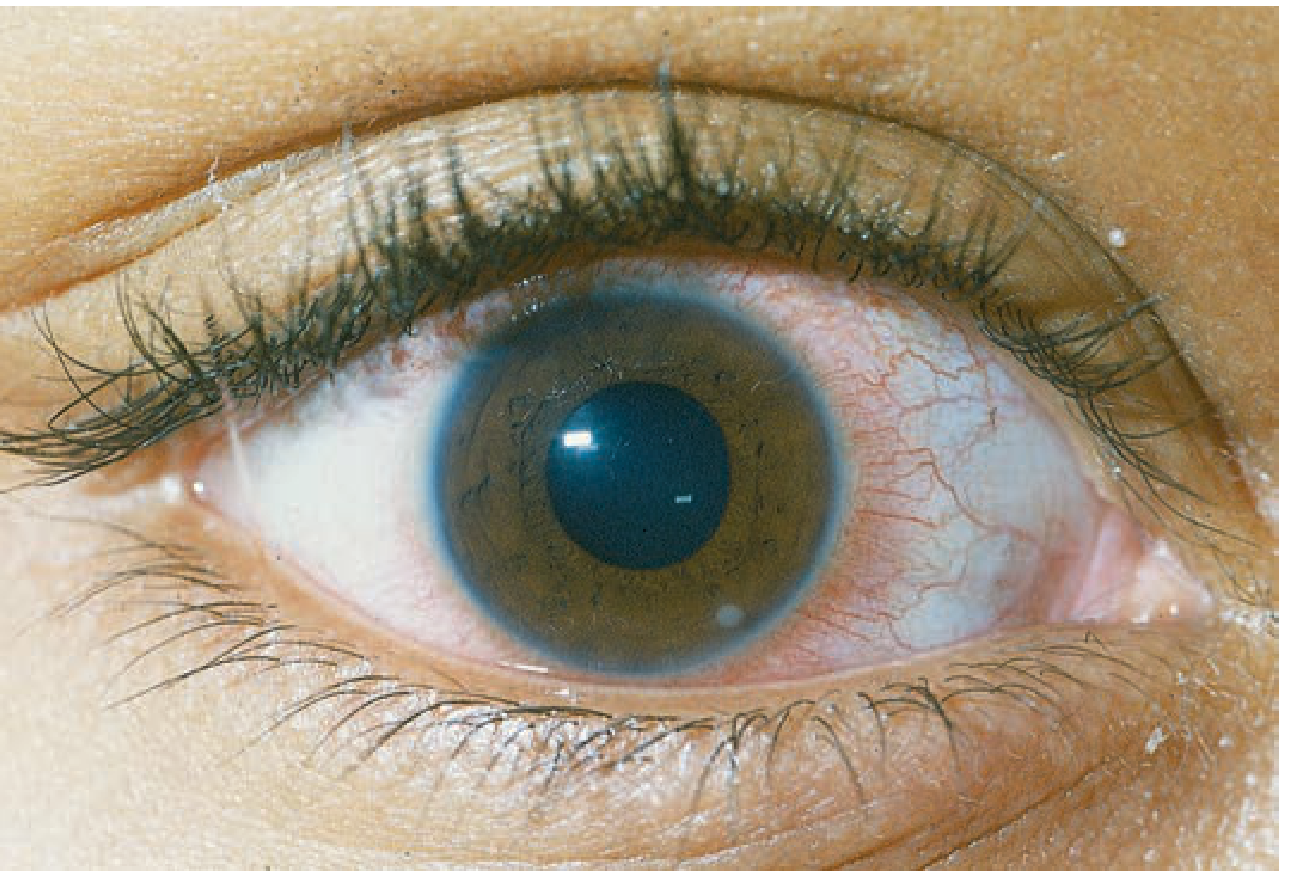
Corneal Ulcer
A corneal ulcer is a serious infection involving multiple layers of the cornea, developing secondary to a break in the epithelial barrier that allows infectious agents to invade the underlying stroma. It is the clinical end result of what is broadly called infectious (microbial) keratitis.
Definition
A corneal ulcer represents full-thickness epithelial loss with underlying stromal involvement and associated inflammatory infiltrate. It must be distinguished from a simple abrasion (epithelial loss only, no stromal involvement). The hallmark on slit-lamp is a focal white opacity (infiltrate) in the corneal stroma associated with an epithelial defect and underlying stromal thinning/tissue loss.
Pathogenesis
The initial disruption of the epithelium can occur via:
-
Desquamation (e.g., exposure keratitis from Bell's palsy, incomplete lid closure causing desiccation)
-
Trauma (direct inoculation of the cornea)
-
Direct microbial invasion (notably Neisseria gonorrhoeae, N. meningitidis, C. diphtheriae, and H. influenzae can penetrate an intact epithelium)
-
Contact lens wear - causes hypoxia, minor trauma, and direct bacterial adherence to the lens surface
-
Kanski's Clinical Ophthalmology, p. 211; Tintinalli's Emergency Medicine, p. (block 20)
Risk Factors
| Factor | Notes |
|---|---|
| Contact lens wear | Most important risk factor. Soft lenses > rigid gas permeable. Extended-wear dramatically increases risk. Pseudomonas causes >60% of contact lens-related keratitis |
| Trauma | Including refractive surgery (especially LASIK) |
| Ocular surface disease | Dry eye, bullous keratopathy, entropion |
| Immunosuppression | Topical or systemic steroids, systemic immunosuppressants |
| Previous ocular surgery | Penetrating keratoplasty, refractive surgery |
| Systemic disease | Diabetes, vitamin A deficiency, collagen vascular diseases |
Causative Organisms
Bacteria (most common cause overall)
- Pseudomonas aeruginosa - aggressive, accounts for >60% of contact lens-related keratitis
- Staphylococcus aureus - focal, fairly well-defined yellow-white infiltrate
- Streptococcus pneumoniae - often aggressive
- Moraxella species
- Serratia species
Viruses
- Herpes simplex virus (HSV) - may cause dendrites and stromal infiltrate
- Varicella zoster virus (VZV)
Fungi
- Candida - common in immunocompromised, often mimic bacterial ulcers
- Aspergillus, Fusarium, Penicillium, Acremonium - filamentous fungi; associated with vegetable/plant matter trauma and contact lens wear; feathery borders and satellite lesions on exam
Protozoa
-
Acanthamoeba - extremely painful, associated with soft contact lens wear, swimming/hot tub exposure; perineural invasion; late ring-shaped infiltrate
-
Tintinalli's Emergency Medicine, Table 241-5; Wills Eye Manual, Section 4.11; Kanski's Clinical Ophthalmology, p. 211
Clinical Features
Symptoms
- Red eye (moderate to severe)
- Moderate-to-severe ocular pain or foreign body sensation
- Photophobia (consensual photophobia if associated iritis)
- Decreased vision (especially if central ulcer)
- Mucopurulent discharge
- Acute contact lens intolerance
Signs
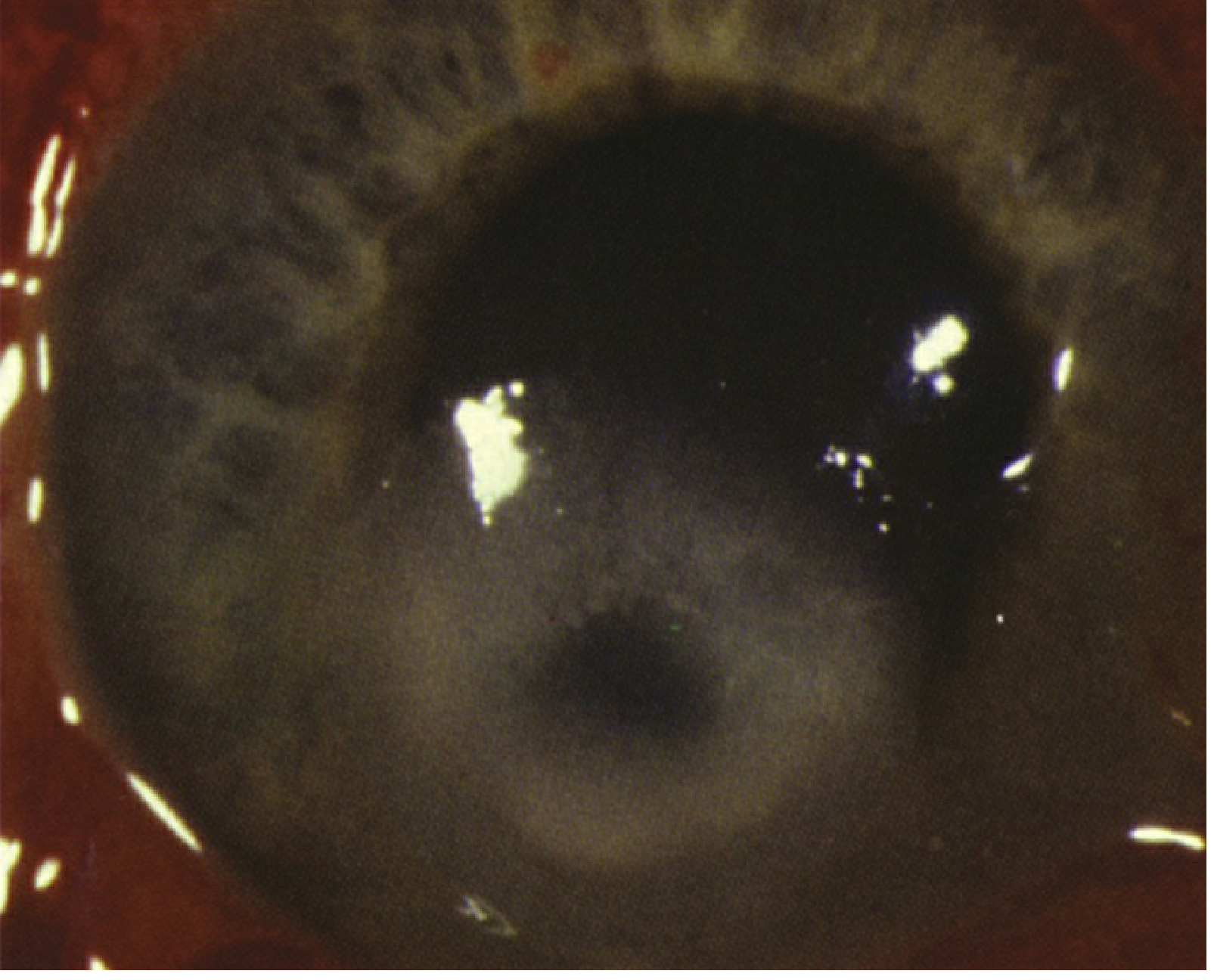
On slit-lamp examination (critical findings):
- Focal white/grey stromal infiltrate with overlying epithelial defect
- Heaped-up ulcer edges (vs. cleaner edges in a simple abrasion)
- Stromal edema and Descemet membrane folds
- Anterior chamber reaction (flare and cells)
- Hypopyon (sterile inflammatory cells in anterior chamber) - sign of severe keratitis
- Conjunctival injection (usually diffuse)
- Mucopurulent discharge, upper eyelid edema
Severe cases may also show:
- Posterior synechiae
- Hyphaema
- Elevated IOP
- Corneal perforation (a feared complication)
Note: A slit beam cannot see clearly through an infiltrate or ulcer to the iris, whereas stromal edema or mild scars are more transparent - this helps distinguish depth of involvement.
- Wills Eye Manual, p. 199-202
Organism-Specific Clues
| Organism | Clinical Clue |
|---|---|
| Pseudomonas | Contact lens wearer; aggressive, rapidly progressive; liquefactive necrosis; mucopurulent discharge |
| Staphylococcus | Focal, well-defined yellow-white infiltrate; often associated with blepharitis |
| Streptococcus | Often aggressive; hypopyon common |
| Fungi (filamentous) | Vegetable matter trauma; feathery borders; satellite lesions |
| Candida | Immunocompromised, preexisting ocular surface disease |
| HSV | Eyelid vesicles, dendrites; recurrent unilateral disease |
| Acanthamoeba | Extremely painful; contact lens + water exposure; ring-shaped infiltrate late; perineural invasion |
Differential Diagnosis
- Corneal abrasion - epithelial defect only, no stromal infiltrate, no white opacity
- Sterile corneal infiltrate - immune reaction to contact lens solution/hypoxia; multiple small peripheral lesions, little staining, minimal AC reaction
- Staphylococcal hypersensitivity - peripheral, often bilateral, clear space between infiltrate and limbus, localized injection, no/minimal AC reaction
- HSV stromal keratitis - no/poor response to antibiotics, dendrites, history of herpes
- Fungal keratitis - feathery borders, satellite lesions, must be considered after vegetable trauma
- Topical anesthetic abuse - large ring opacity, should be suspected with poor response to therapy
- Peripheral corneal thinning/melting - associated systemic disease (RA, Wegener's, PAN)
Investigations
Corneal culture (mandatory before starting antibiotics):
The ophthalmologist scrapes the center of the ulcer to culture the offending organism. Culture media used:
| Medium | Organisms Detected |
|---|---|
| Blood agar | Most bacteria and fungi (except Neisseria, Haemophilus, Moraxella) |
| Chocolate agar | Fastidious bacteria (H. influenzae, Neisseria, Moraxella) |
| Sabouraud dextrose agar | Fungi |
| Non-nutrient agar + E. coli | Acanthamoeba |
| Brain-heart infusion broth | Streptococci, meningococci, yeasts |
| Lowenstein-Jensen | Mycobacteria, Nocardia (keep for 8 weeks) |
PCR + nanopore sequencing is now available and can identify the exact species and antibiotic resistance profile.
- Kanski's Clinical Ophthalmology, Table 7.2, p. 229
Treatment
General Principles
- Treat aggressively - do not delay
- Obtain cultures before starting antibiotics
- Emergent ophthalmologic consultation is indicated
- Never pressure patch an infected eye; never patch a contact lens wearer
Topical Antibiotics (first-line)
Fluoroquinolones are the current standard:
- Ciprofloxacin (Ciloxan) or Ofloxacin (Ocuflox) - 1 drop every hour in the affected eye
- Moxifloxacin or Gatifloxacin are also commonly used (good Gram-positive and Gram-negative coverage)
For severe/sight-threatening ulcers - loading dose protocol:
1 drop every 5 minutes for five doses, then every 30-60 minutes around the clock
Adjunctive Measures
- Cycloplegic (e.g., cyclopentolate 1% TID) - for iritis/ciliary spasm
- Topical steroids - only after organism and sensitivities known, infection under control, and severe inflammation persists; avoid in fungal, atypical mycobacteria, Nocardia, or Pseudomonas keratitis
- Doxycycline 100 mg PO BID (MMP inhibitor) + Vitamin C 1-2 g/day - to suppress connective tissue breakdown and prevent perforation in thinning corneas
- Eye shield (not pressure patch) for corneal thinning
- No contact lens wear
Systemic Antibiotics
- Oral fluoroquinolones (ciprofloxacin 500 mg BID; moxifloxacin 400 mg daily) for scleral extension or impending/frank perforation
- Ceftriaxone 1 g IV q12-24h for N. gonorrhoeae with corneal involvement (single 1 g IM if conjunctival involvement only)
- Amoxicillin/clavulanate for H. influenzae infections (risk of systemic spread)
- Note: systemic fluoroquinolones are no longer recommended for gonococcal infections due to resistance
Indications for Hospitalization
-
Sight-threatening infection or impending perforation
-
Patient unable to administer drops at required frequency
-
Likely noncompliance
-
Suspected topical anesthetic abuse
-
Neisseria infection (requiring IV antibiotics)
-
Wills Eye Manual, p. 199-207; Tintinalli's Emergency Medicine, block 20
Complications
- Corneal scarring - permanent visual impairment
- Corneal perforation - may lead to endophthalmitis
- Endophthalmitis - fulminant, sight-threatening
- Descemetocele - Descemet membrane bulging through a full-thickness ulcer
- Adherent leucoma - iris adherent to posterior cornea
- Corneal vascularization
- Phthisis bulbi - end-stage shrinking of globe after severe infection
Recent Evidence (2024-2026)
A Cochrane network meta-analysis (2025) on topical antibiotics for bacterial keratitis is the most current high-level evidence available (PMID: 40728038). A 2024 systematic review of Fusarium keratitis (1969-2023, PMID: 39107598) highlights the growing importance of fungal corneal infections.
Sources: Tintinalli's Emergency Medicine (A Comprehensive Study Guide); The Wills Eye Manual (9th ed); Kanski's Clinical Ophthalmology (10th ed); Rosen's Emergency Medicine
Give in short
Corneal Ulcer - Quick Summary
Definition
Full-thickness epithelial loss + stromal infiltration/tissue loss. More serious than a simple abrasion.
Key Risk Factors
- Contact lens wear (especially extended-wear soft lenses) - #1 risk
- Trauma / ocular surgery
- Immunosuppression (topical/systemic steroids)
- Exposure keratitis (Bell's palsy)
Common Organisms
| Type | Examples |
|---|---|
| Bacteria | Pseudomonas (contact lens), S. aureus, S. pneumoniae |
| Virus | HSV, VZV |
| Fungi | Candida, Aspergillus, Fusarium |
| Protozoa | Acanthamoeba (contact lens + water exposure) |
Clinical Features
- Symptoms: Red eye, severe pain, photophobia, decreased vision, discharge
- Signs: White/grey stromal infiltrate, epithelial defect, hypopyon (severe), AC reaction
Diagnosis
- Slit-lamp exam (corneal scraping for culture before starting antibiotics)
Treatment
- Topical fluoroquinolone (ciprofloxacin/moxifloxacin) - 1 drop/hour; q5min loading for severe cases
- Cycloplegic for iritis
- Systemic antibiotics for Neisseria (ceftriaxone IV) or scleral extension
- No patching, no contact lenses
- Urgent ophthalmology referral
Complications
Corneal scarring → perforation → endophthalmitis → vision loss
This is a shared conversation. Sign in to Orris to start your own chat.