Breech presentation: classification, diagnosis, the course of labor. Indications abdominal delivery.
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive, textbook-based review of breech presentation.
Breech Presentation
1. Incidence and Etiology
Breech presentation occurs in approximately 3-4% of all deliveries at term. Its frequency declines with advancing gestation: ~24% at 18-22 weeks, ~8% at 28-30 weeks, ~7% at 34 weeks, and ~2.8% at 38-40 weeks.
Associated factors:
- Fundal-cornual placental implantation (occurs in only 7% of all pregnancies but strongly associated with breech)
- Uterine anomalies (septate, bicornuate uterus)
- Prematurity and multiple gestation
- Polyhydramnios or oligohydramnios
- Pelvic tumors or structural abnormalities
- Fetal neuromuscular disorders (reduced fetal movement/tone - infants with neuromuscular disorders have disproportionately high rates of breech at delivery)
- Hydrocephaly or other major fetal anomalies
(Creasy & Resnik's Maternal-Fetal Medicine, p. 953)
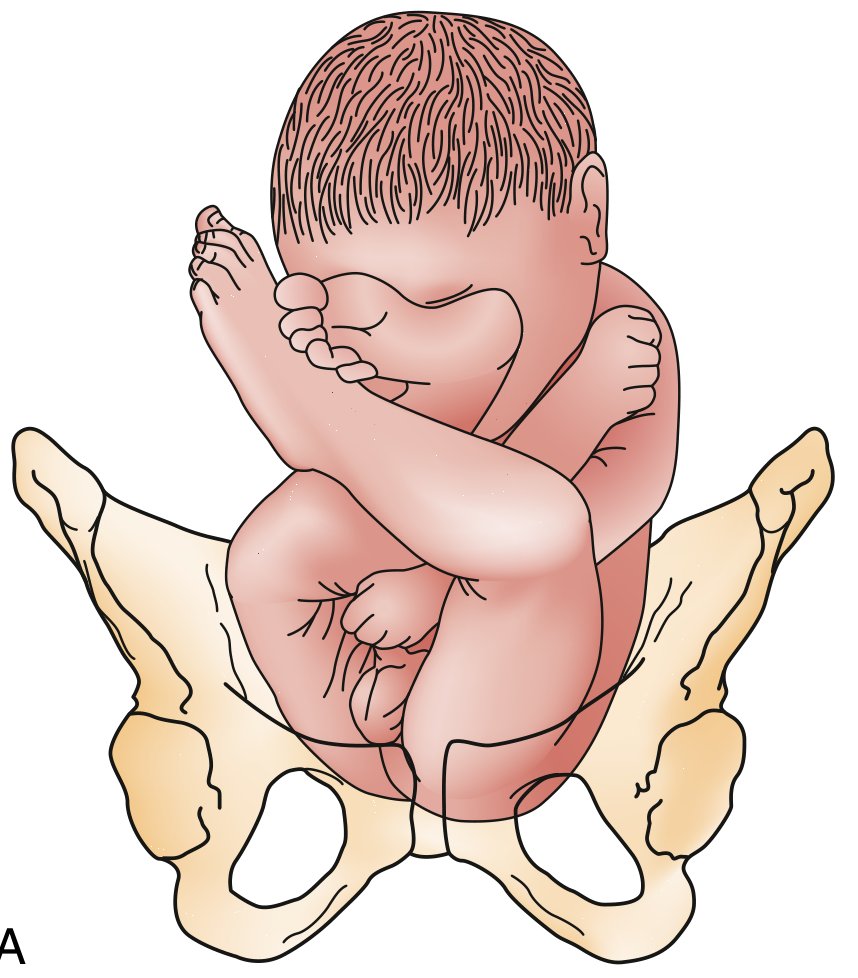
2. Classification
Breech presentations are classified into three main types. The sacrum is the reference point (denominator) for position.
A. Frank Breech (Extended Breech)
- Hips flexed, knees extended - legs lie alongside the trunk
- Most common: 60-65% of all breech presentations
- Buttocks act as a good dilating wedge
- Cord prolapse risk: ~0.5% (lowest of the three types)
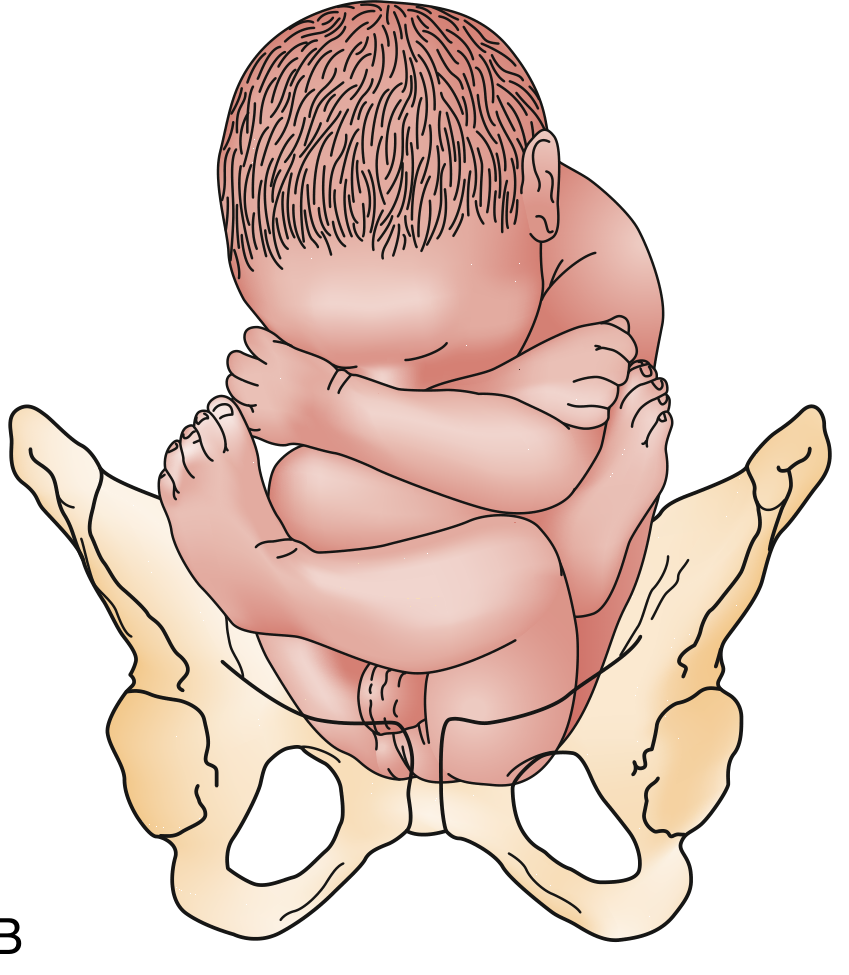
B. Complete Breech (Flexed Breech)
- Hips and knees both flexed - fetus in a "squatting" posture
- Least common: ~5% of all breech presentations
- Buttocks still act as a reasonable dilating wedge
- Cord prolapse risk: 5-6%
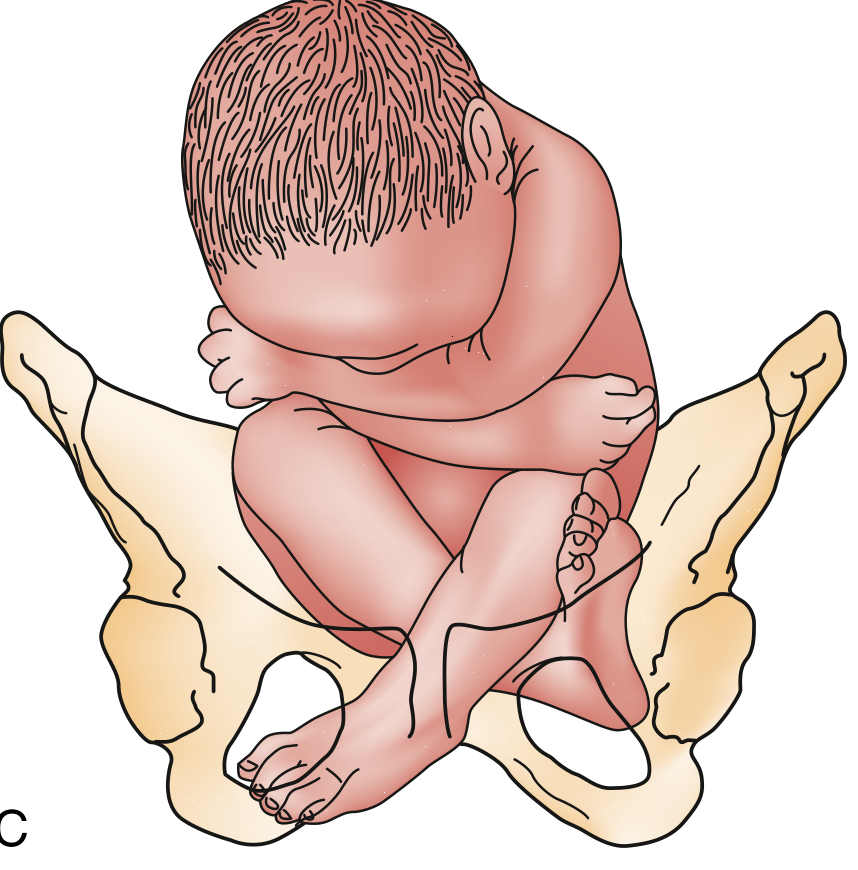
C. Incomplete (Footling) Breech
- One or both feet (or knees) are lowermost in the canal; incomplete hip flexion
- Frequency: 25-35% of all breech presentations
- Poor cervical dilating wedge
- Highest cord prolapse risk: 15-18%
(Rosen's Emergency Medicine, p. 3415; Roberts & Hedges' Clinical Procedures, p. 1351)
3. Diagnosis
Clinical Methods
Leopold's maneuvers (before or early labor):
- First maneuver: the hard, ballotable fetal head is felt in the fundus (instead of the softer breech)
- Third maneuver (Pawlik's): the presenting part above the symphysis is soft, irregular, and does not ballot as sharply as the head
- Fourth maneuver: the back is identified on one side, the small parts on the other
Vaginal examination (during active labor):
- The presenting part is soft and irregular
- The sacrum, ischial tuberosities, anus, and genitalia may be palpable
- Key differentiating clue: the anus is flanked by bony prominences on only two sides, whereas the face and skull have a complete circle of bone around them
- Whenever a fontanel cannot be identified on examination, breech presentation should be suspected
Ultrasound
Confirms the diagnosis and additionally provides:
- Type of breech (frank, complete, footling)
- Gestational age and estimated fetal weight
- Position of fetal arms and neck - hyperextension of the fetal neck is a contraindication to vaginal delivery (high risk of spinal cord injury)
- Placental location
- Amniotic fluid volume
- Fetal anomalies
(Rosen's Emergency Medicine, p. 3415; Roberts & Hedges', p. 1351)
4. Course of Labor
First Stage
Labor in breech presentation generally proceeds similarly to vertex presentations. However:
- The buttocks are a less effective dilating wedge (especially incomplete breech)
- Fetal monitoring is essential throughout - because the fetal abdomen and umbilical cord insertion are in the lower uterine segment during late first stage and second stage, significant variable decelerations are more likely than with cephalic presentation
- Membranes should be left intact as long as possible to provide hydraulic protection against cord compression
Second Stage - Mechanism of Labor
The widest engaging diameter is the bitrochanteric diameter.
Sequence of movements:
- Engagement - bitrochanteric diameter engages in an oblique diameter of the pelvic inlet
- Descent - the anterior hip descends more rapidly than the posterior hip
- Internal rotation - bitrochanteric diameter rotates to assume the anteroposterior (AP) diameter of the outlet
- Lateral flexion - the anterior hip catches beneath the symphysis pubis, allowing the posterior hip to be born first, then the anterior hip
- Shoulder engagement - the fetal body rotates so the shoulders engage obliquely; they descend and rotate to the AP diameter; the anterior shoulder follows lateral flexion, and the posterior shoulder is born first
- Delivery of the after-coming head - the head engages in the same diameter as the shoulders; flexion, descent, and rotation bring the posterior neck under the symphysis; the head is born in flexion
Risks Inherent in Labor
- Prolapse of the umbilical cord - especially in footling breech
- Trapping of the after-coming head by an incompletely dilated cervix - particularly dangerous in preterm infants (<1500 g) and with CPD
- Trauma from extension of the fetal head or nuchal position of the arms
- Fetal acidosis - breech labors are more often associated with significant fetal acidosis than cephalic presentations; fetal blood sampling from the buttock is possible if the heart rate pattern is ominous
Prognostic Scoring (Zatuchni-Andros Index)
Points are assigned for parity, gestational age, estimated fetal weight, previous breech deliveries, cervical dilation, and fetal station. A score of ≥4 is associated with a higher success rate for vaginal delivery.
(Creasy & Resnik's MFM, p. 954-955)
Criteria for Allowing a Trial of Labor (Vaginal Breech Delivery)
If vaginal delivery is to be attempted, the following criteria should be met:
- Frank or complete breech presentation (not footling)
- Estimated fetal weight 2000-3800 g
- Normal gynecoid pelvis with adequate measurements (AP inlet ≥11 cm, widest transverse inlet ≥12 cm, interspinous diameter ≥9 cm)
- Flexed fetal head (not hyperextended)
- Experienced obstetrician present
(Creasy & Resnik's MFM, p. 955)
Types of Vaginal Breech Delivery
- Spontaneous breech: infant delivers without manipulation - rare at term, minimal traumatic morbidity
- Partial (assisted) breech extraction: spontaneous to the umbilicus, then body is extracted
- Total breech extraction: entire body extracted by clinician - rarely indicated except for second twin in emergency
Mauriceau maneuver: the fetal mouth is used to flex the fetal neck and draw in the chin for delivery of the after-coming head; avoids neck extension and cord injury.
Piper forceps: applied to the after-coming head; reduces neonatal mortality and is the preferred method for head delivery in vaginal breech.
5. Indications for Cesarean (Abdominal) Delivery
Absolute / Standard Indications Relating to Breech
| Indication | Rationale |
|---|---|
| Footling/incomplete breech at term | Poor dilating wedge, very high cord prolapse risk (15-18%); vaginal delivery is unsafe |
| Failed or contraindicated external cephalic version (ECV) | ACOG recommends planned cesarean if ECV is unsuccessful |
| Hyperextended fetal head | High risk of spinal cord injury with vaginal delivery |
| Estimated fetal weight >3800 g or <2000 g | Macrosomia increases dystocia risk; prematurity increases head-entrapment risk |
| Inadequate pelvis (CPD, pelvic measurements below threshold) | Mechanical obstruction; pelvimetry showing AP inlet <11 cm, transverse inlet <12 cm, interspinous <9 cm |
| Fetal distress (pH <7.20 early in second stage, ominous FHR) | Expeditious abdominal delivery preferred |
| Cord prolapse with bradycardia | Emergency delivery necessary |
| Preterm breech <32 weeks | Retrospective data shows increased neonatal mortality with vaginal attempt vs. planned cesarean at 24-32 weeks |
| Lack of experienced operator | If the obstetrician is not skilled in vaginal breech delivery, cesarean is preferred |
General Indications for Cesarean That Apply to All Presentations (from Morgan & Mikhail)
Labor unsafe for mother and fetus:
- Increased risk of uterine rupture (previous classic cesarean section, previous extensive myomectomy)
- Central or partial placenta previa
- Abruptio placentae
Dystocia:
- Fetopelvic disproportion (CPD)
- Abnormal fetal presentation (transverse/oblique lie, breech)
- Dysfunctional uterine activity
Emergent delivery:
- Fetal distress
- Umbilical cord prolapse with fetal bradycardia
- Maternal hemorrhage
- Active genital herpes with ruptured membranes
- Impending maternal death
(Morgan & Mikhail's Clinical Anesthesiology, p. 1625; Creasy & Resnik's MFM, p. 954-962)
The Hannah Trial (Term Breech Trial, 2000)
The landmark RCT by Hannah et al. (2088 subjects) found that planned vaginal delivery was associated with significantly greater perinatal morbidity and mortality compared to planned cesarean delivery, without significant differences in maternal morbidity. This study, despite methodological limitations (lack of pelvimetry in >90%, uncontrolled oxytocin use, 22% of vaginal deliveries unattended by an obstetrician), cemented the shift to routine cesarean for term breech. ACOG subsequently recommended planned cesarean delivery when ECV fails.
(Creasy & Resnik's MFM, p. 954)
Summary
| Type | Hips | Knees | Frequency | Cord Prolapse Risk |
|---|---|---|---|---|
| Frank | Flexed | Extended | 60-65% | ~0.5% |
| Complete | Flexed | Flexed | ~5% | 5-6% |
| Incomplete/Footling | Partial/Extended | Variable | 25-35% | 15-18% |
The overall management trend is toward planned cesarean for term breech when ECV has failed or is contraindicated, as evidence consistently shows lower perinatal morbidity and mortality compared to planned vaginal delivery. Vaginal delivery remains acceptable in carefully selected cases (frank or complete breech, adequate pelvis, estimated weight 2000-3800 g, flexed head, experienced obstetrician).
This is a shared conversation. Sign in to Orris to start your own chat.