I now have everything I need to give a thorough, well-illustrated explanation. Let me compile the full answer.
Foot Inversion vs. Eversion: The Muscular Tug-of-War
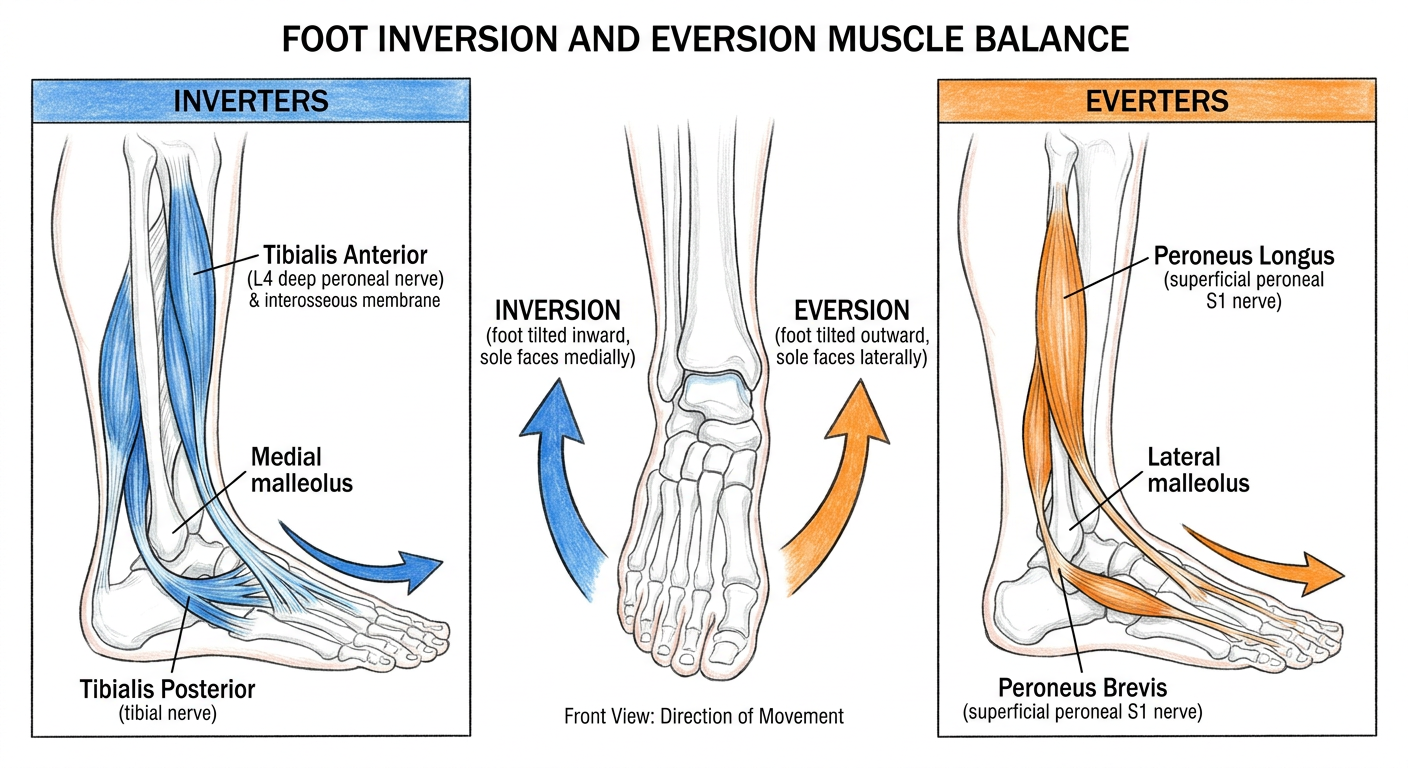
The subtalar and midtarsal joints allow two opposing rotary movements at the foot: inversion (sole turns medially) and eversion (sole turns laterally). These movements are controlled by two competing muscle groups that must remain balanced for normal gait and arch support.
The Concept: A Mechanical Balance
Think of the foot as a see-saw balanced at the subtalar joint. Muscles on the medial side pull the foot inward (inversion), while muscles on the lateral side pull it outward (eversion). Normal stance and walking require dynamic equilibrium between these two groups.
THE INVERTERS
1. Tibialis Anterior
| Feature | Detail |
|---|
| Compartment | Anterior compartment of leg |
| Origin | Lateral surface of tibia (upper 2/3) + interosseous membrane |
| Insertion | Medial cuneiform + base of 1st metatarsal |
| Nerve | Deep peroneal nerve (L4) |
| Primary actions | Dorsiflexion + inversion |
Tibialis anterior runs diagonally across the front of the ankle, crossing medially to insert on the medial aspect of the foot. This medial insertion is what gives it its inversion vector - as it contracts, it lifts the medial border of the foot upward and inward. It is the most powerful dorsiflexor, but its inversion role is equally important.
2. Tibialis Posterior
| Feature | Detail |
|---|
| Compartment | Deep posterior compartment of leg |
| Origin | Posterior surface of interosseous membrane + adjacent tibia + fibula |
| Insertion | Tuberosity of navicular (primary) + medial cuneiform + multiple tarsal bones |
| Nerve | Tibial nerve (L4, L5) |
| Primary actions | Plantarflexion + inversion + support of medial arch |
Tibialis posterior is the deepest and most centrally placed muscle in the posterior compartment. Its tendon courses behind the medial malleolus (under the flexor retinaculum) and fans out to attach broadly across the medial tarsus. This broad medial insertion makes it the most powerful inverter of the foot and a key dynamic stabilizer of the medial longitudinal arch.
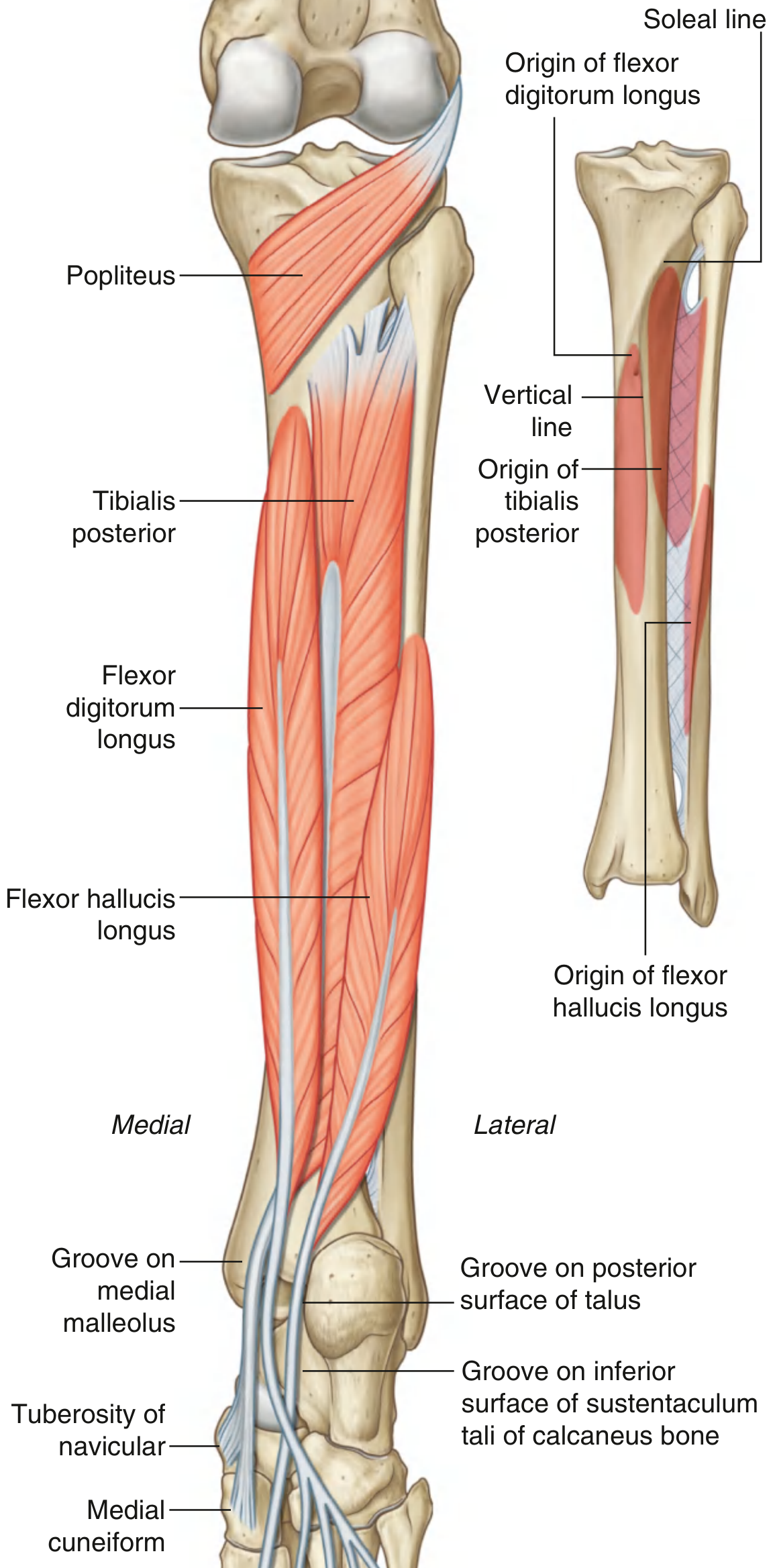
Key anatomical diagram - posterior compartment muscles:
(Gray's Anatomy for Students - Deep Group, Posterior Compartment of the Leg. Notice how tibialis posterior originates from the interosseous membrane and inserts at the navicular tuberosity and medial cuneiform.)
THE EVERTERS (counterbalancers)
Peroneus Longus + Peroneus Brevis
| Feature | Peroneus Longus | Peroneus Brevis |
|---|
| Compartment | Lateral compartment | Lateral compartment |
| Origin | Proximal 2/3 fibula | Distal 2/3 fibula |
| Insertion | Medial cuneiform + base 1st metatarsal | Tuberosity of 5th metatarsal |
| Nerve | Superficial peroneal (S1) | Superficial peroneal (S1) |
| Actions | Eversion + plantarflexion + arch support | Eversion (primary) |
Both peroneal muscles run behind the lateral malleolus and pull the foot outward and downward - the exact opposite of tibialis posterior. Peroneus longus has an especially interesting course: it wraps under the cuboid and crosses the sole of the foot obliquely to reach the medial side, tensioning the transverse arch in the process.
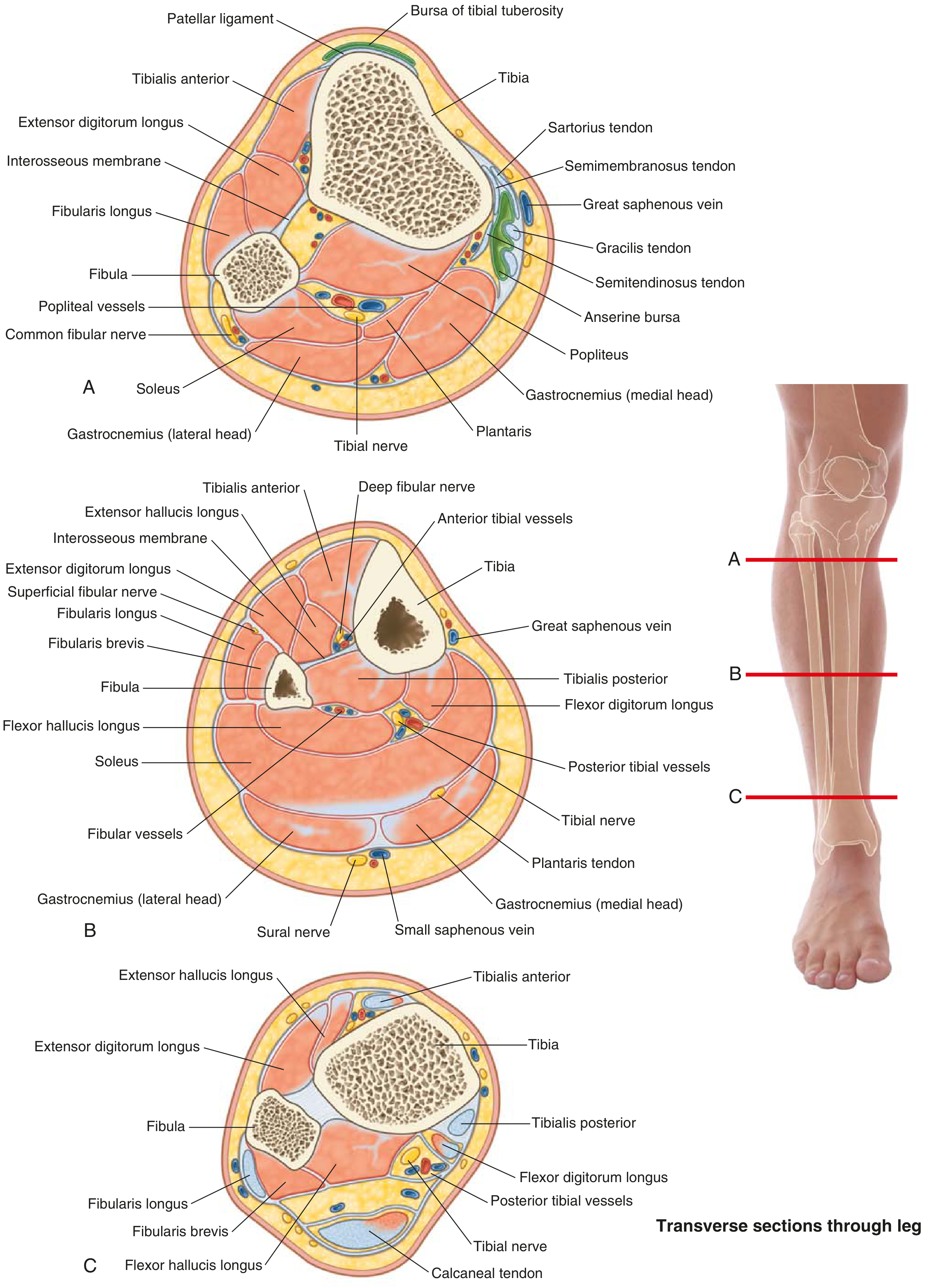
Cross-Sectional View of the Leg - Seeing the Balance
This transverse section diagram shows how the two groups are anatomically separated by the interosseous membrane and fibula:
(Miller's Review of Orthopaedics / Gray's Atlas - Transverse sections through the leg at three levels)
Notice:
- Tibialis anterior sits anteromedially (anterior compartment)
- Tibialis posterior sits deepest in the posteromedial compartment
- Fibularis (peroneus) longus and brevis sit in the lateral compartment, directly opposite
This anatomical positioning - medial muscles vs. lateral muscles - creates the mechanical lever arms for inversion vs. eversion, respectively.
Summary: The Balance Table
| Inverters | Everters |
|---|
| Muscles | Tibialis anterior, Tibialis posterior | Peroneus longus, Peroneus brevis |
| Compartment | Anterior + Deep posterior | Lateral |
| Nerve | Deep peroneal (L4), Tibial (L4-5) | Superficial peroneal (S1) |
| Movement | Sole turns medially | Sole turns laterally |
| Route past ankle | Behind/in front of medial malleolus | Behind lateral malleolus |
| Arch role | Support medial arch | Tension transverse + lateral arch |
Clinical Significance
Why this balance matters:
- Tibialis posterior dysfunction (e.g., tendon rupture in adult flatfoot): eversion goes unchecked → progressive flatfoot, hindfoot valgus, forefoot abduction
- Peroneal nerve palsy (common fibular nerve injury): evertors are paralyzed → unopposed inversion by tibialis anterior/posterior → foot drop with a supinated, inverted posture
- Charcot-Marie-Tooth disease: peroneal muscles weaken early, tibialis posterior and anterior dominate → pes cavus (high-arched foot) with hindfoot varus
In the words of Gray's Anatomy for Students describing CMT: "The stronger tibialis posterior muscle... elevates the medial longitudinal arch and inverts the foot. The exaggerated inversion produces hindfoot varus."
The two groups also work together: during the stance phase of gait, tibialis posterior fires first (mid-stance) to lock the subtalar joint and stiffen the foot for push-off, while the peroneals control the degree of pronation during heel strike and loading. This coordinated timing - not just static opposition - is the true meaning of "counterbalance."
Sources: Miller's Review of Orthopaedics 9th Ed, p. 202-203 | Gray's Anatomy for Students, p. 728 | Rockwood and Green's Fractures in Adults 10th Ed