Stoppas approach
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive overview of the Stoppa Approach (Anterior Intrapelvic / Modified Stoppa Approach) for acetabular and pelvic fracture surgery, drawn from Campbell's Operative Orthopaedics 15th Ed 2026 and Rockwood & Green's Fractures in Adults 10th Ed 2025.
Stoppa Approach (Anterior Intrapelvic / Modified Stoppa Approach)
Also called the Anterior Intrapelvic (AIP) approach, this is a preperitoneal approach to the inner pelvis, most widely used for acetabular fracture fixation. It replaces the medial window of the traditional ilioinguinal approach with a less morbid dissection plane.
Indications
- Anterior wall and anterior column acetabular fractures
- Quadrilateral surface fractures - especially comminuted ones requiring direct buttress plating; this is the primary indication over the ilioinguinal approach
- Anterior column-posterior hemitransverse fractures
- Both-column fractures (anterior approach component)
- T-shaped fractures with anterior displacement
- Transverse fractures combined with pubic symphysis disruption
- Can be combined with the lateral (first) window of the ilioinguinal approach to avoid dissecting the middle window (femoral neurovascular bundle)
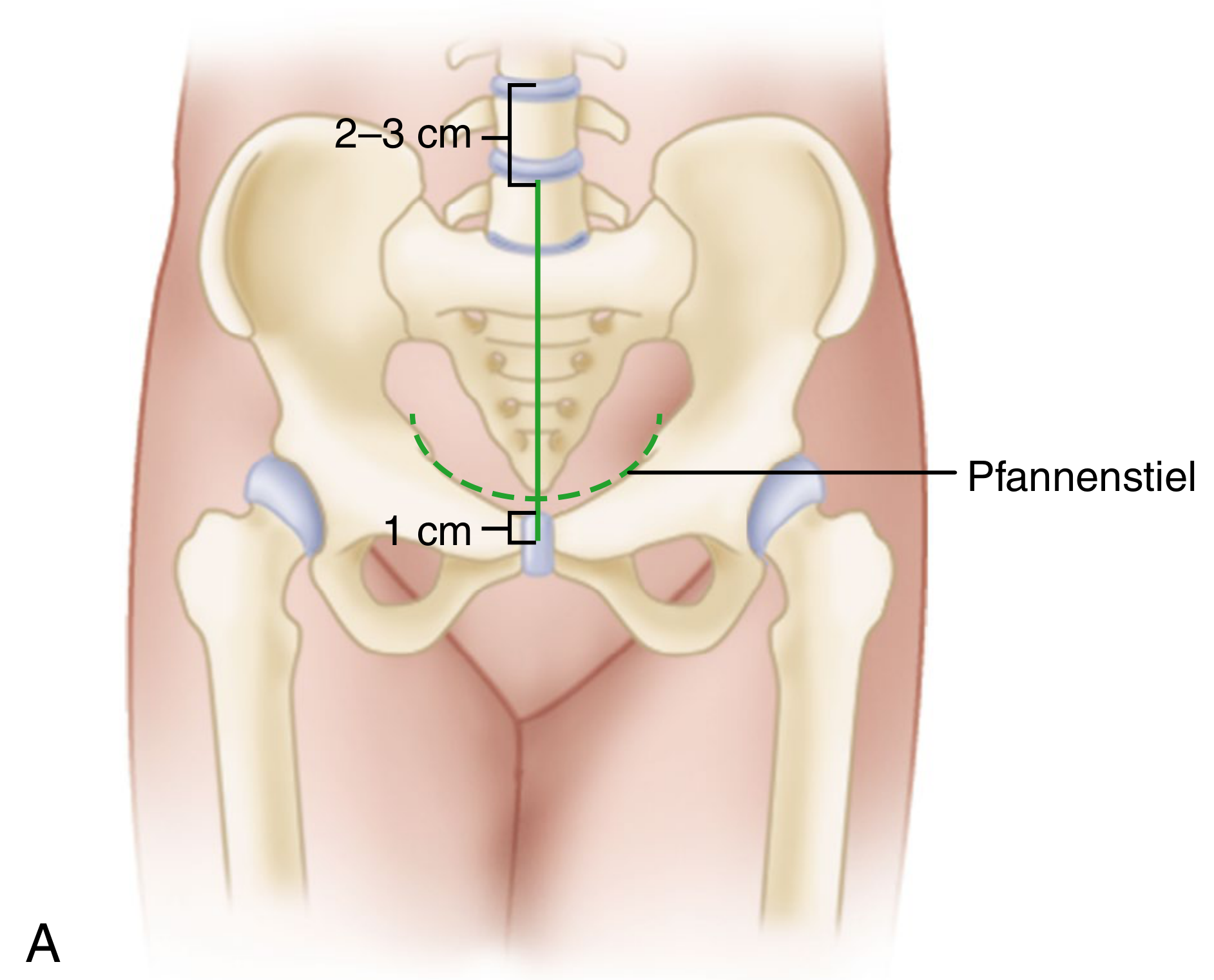
Incision
Two options:
- Pfannenstiel incision (preferred) - transverse, approximately 2 cm above the pubic symphysis (shown in the diagram below)
- Vertical midline incision - starting 1 cm inferior to the symphysis, ending 2-3 cm below the umbilicus; used when a prior laparotomy incision exists
Step-by-Step Technique
- Make Pfannenstiel or midline skin incision and divide subcutaneous tissue down to the rectus fascia.
- Identify the linea alba (decussation of fascial fibers); incise the rectus fascia longitudinally along the linea alba.
- Gently retract both rectus abdominis bellies laterally.
- Stay in the preperitoneal (retropubic) space - do NOT open the peritoneum.
- Pack a damp laparotomy sponge in the retropubic space and place a malleable retractor to protect the bladder.
- Release the rectus muscle off the anterior surface of the pubic tubercle.
- Sharply dissect periosteum from the superior pubic bone; carry blunt dissection deeper.
- Identify the superior pubic ramus (pectin pubis) and carry dissection laterally along the pelvic brim.
- Place a sharp Hohmann retractor over the ramus lateral to the tubercle; use a Deaver retractor laterally to protect iliac vessels.
- Identify and ligate the corona mortis vessels (anastomoses between the obturator vessels and the external iliac or inferior epigastric vessels) - a critical safety step.
- Continue subperiosteal dissection along the pelvic brim to the iliopectineal eminence.
- Dissect the iliopectineal arch from the bone to allow elevation of the femoral vessels and nerve.
- Continue over the anterior acetabular wall; place Hohmann/custom retractors near the iliopubic eminence.
- Continue lateral dissection along the pelvic brim to the entire internal surface of the superior pubic ramus.
- At the quadrilateral surface: identify the obturator neurovascular bundle, protect it, and place a custom pelvic floor retractor into the lesser sciatic notch.
- Elevate the periosteum and obturator internus with a Cobb elevator to expose the quadrilateral surface.
- After full pelvic brim exposure, a sharp Hohmann retractor can be impacted at the posterior top of the acetabulum into the ilium just lateral to the sacroiliac joint.
Key Anatomy and Hazards
| Structure | Risk |
|---|---|
| Corona mortis | Must be ligated - vascular anastomosis between obturator and external iliac/inferior epigastric vessels |
| Bladder | Retracted medially with malleable retractor; protected with wet sponge in retropubic space |
| Obturator neurovascular bundle | At risk during quadrilateral surface dissection; requires direct identification |
| External iliac vessels | Protected by Deaver retractor; avoid excessive stretch |
| Peritoneum | Must not be opened; entire approach stays in the preperitoneal space |
| Lateral femoral cutaneous nerve | At risk if the lateral window of the ilioinguinal approach is added |
Advantages over the Ilioinguinal Approach
- Avoids the middle window of the ilioinguinal approach, thus no dissection around the femoral vein, artery, nerve, and lymphatics
- Excellent direct access to the quadrilateral surface for buttress plating
- Better access for cleaning the anterior column fracture line
- Can be combined with the lateral (first) ilioinguinal window - the "AIP + lateral window" combination is increasingly favored over the full ilioinguinal approach
- Adding an ASIS osteotomy can further improve access to the anterior wall and psoas gutter (the territory of the middle ilioinguinal window)
Limitations
- Does not provide direct hip joint access (articular surface not directly visualized; reduction is inferred from extra-articular fracture lines and fluoroscopy)
- Fractures with significant posterior displacement may require an additional posterior Kocher-Langenbeck approach
- Limited access to posterior column fractures unless combined
Position and Setup
- Patient supine on a radiolucent flat-top table
- Affected limb prepped into the field (allows intraoperative manipulation)
- Some surgeons use a pelvic reconstruction table
- Skeletal traction aids visualization, especially through the lateral window
- A triangle under the hip relaxes the iliopsoas
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026, pp. 90 & 3507-3510
- Rockwood and Green's Fractures in Adults 10th Ed 2025, pp. 2525-2530
This is a shared conversation. Sign in to Orris to start your own chat.