Teach me the development of inter ventricular septa with suitable images
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
I now have all the content and images needed to deliver a comprehensive, well-illustrated lesson. Let me compose the full response.
Development of the Interventricular Septum
Sources: The Developing Human: Clinically Oriented Embryology (Moore et al.) & Langman's Medical Embryology
Overview
The interventricular septum (IVS) divides the single primordial ventricle into the right and left ventricles. Its formation is one of the most complex partitioning events in cardiac embryology because it involves contributions from three distinct tissue sources and must be perfectly coordinated with outflow tract septation. Errors in this process produce ventricular septal defects (VSDs) - the most common congenital heart defect.
Stage 1: Appearance of the Primordial Ventricle (Week 4)
By the end of the 4th week, the primitive heart tube consists of several segments: the sinus venosus, atrium, atrioventricular canal, ventricle, bulbus cordis, and truncus arteriosus.
The primordial single ventricle begins to expand. As the two sides balloon outward (the left and right primitive ventricles), their medial walls become apposed and gradually merge at the floor of the ventricle, near the apex. This merging creates the first sign of the IVS.
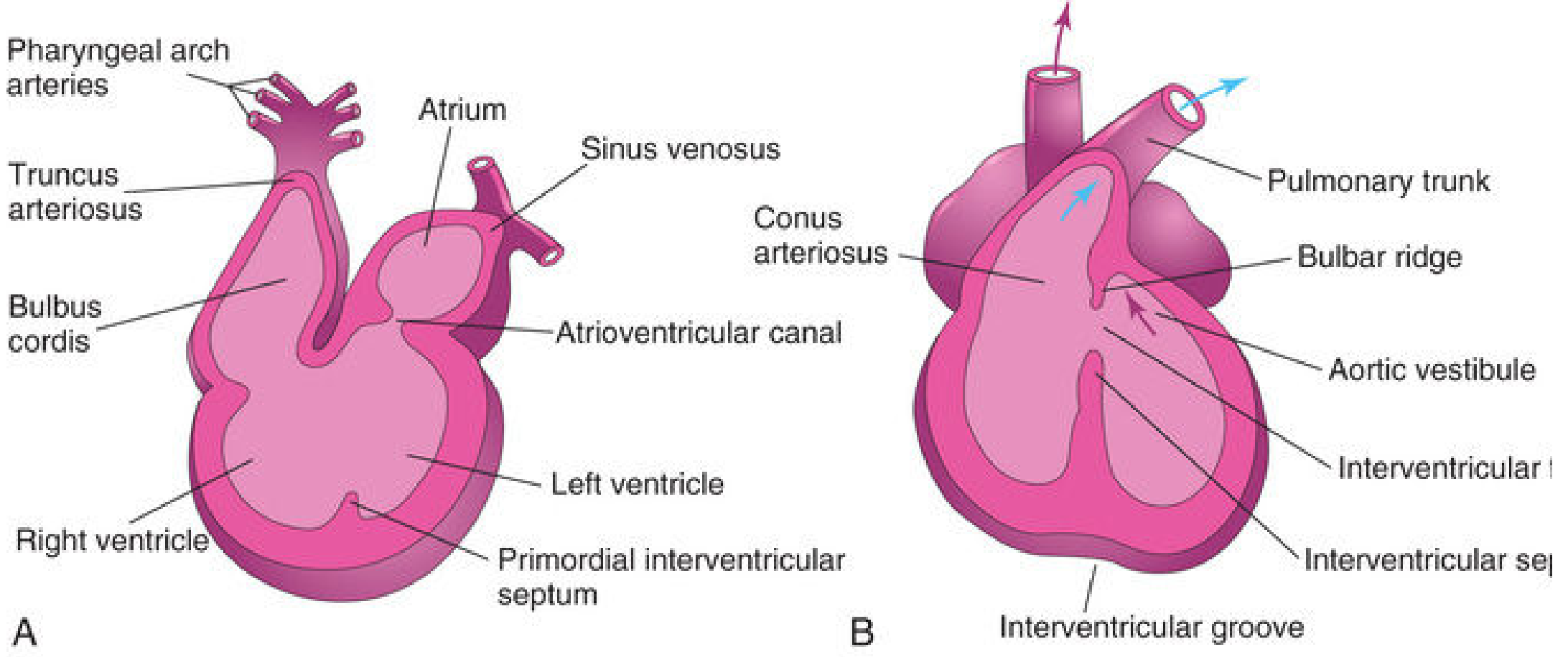
Stage 2: Formation of the Muscular Interventricular Septum (Weeks 4-6)
A median ridge - the muscular interventricular septum - rises from the floor of the ventricle near its apex. Key features:
- Myocytes from both the left and right primordial ventricles contribute to it
- The septum has a concave free (superior) edge, leaving a gap called the interventricular foramen
- Initially the septum grows primarily because the ventricles on either side dilate outward (passive growth)
- Later, active proliferation of myoblasts within the septum increases its size
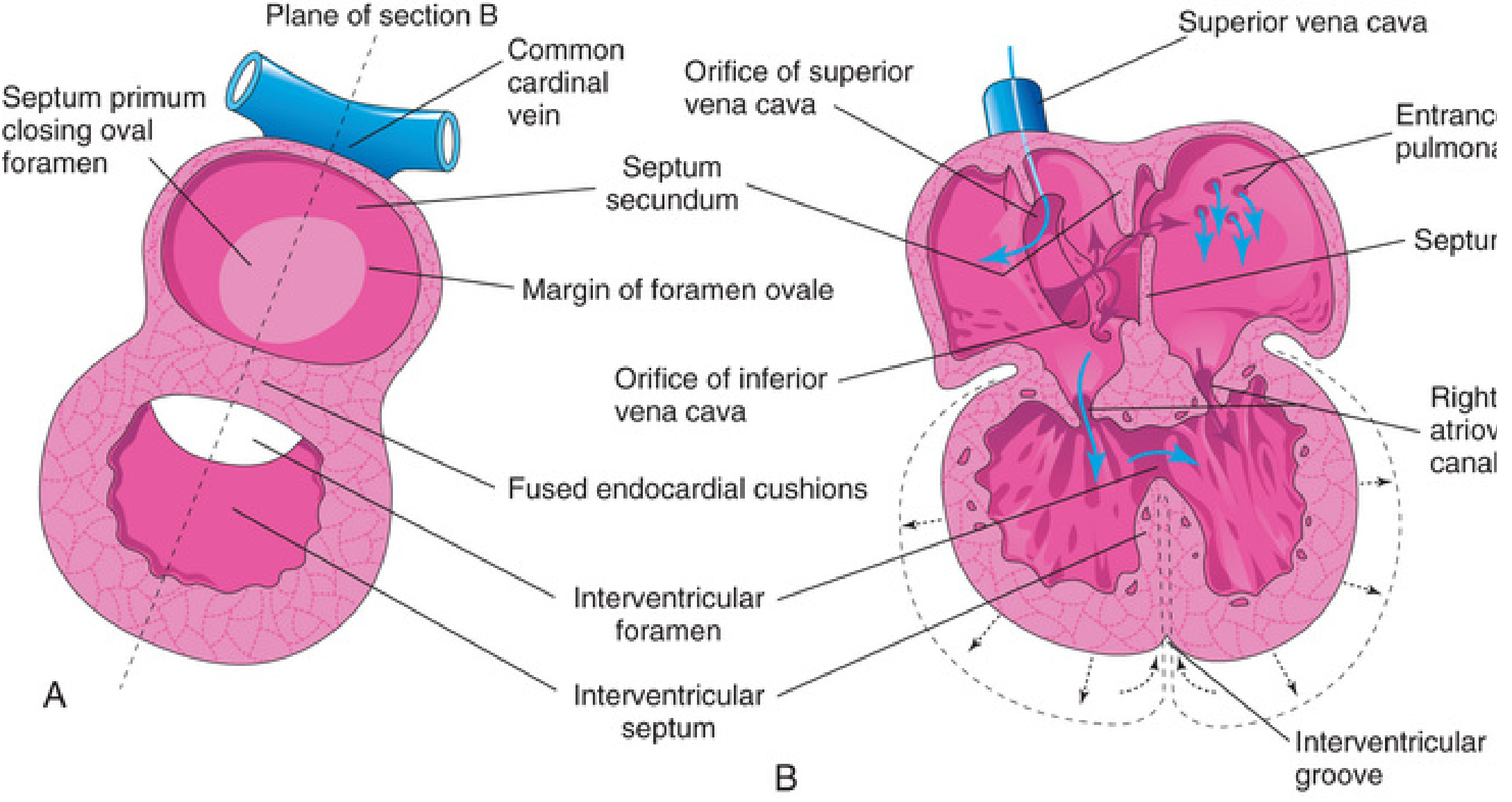
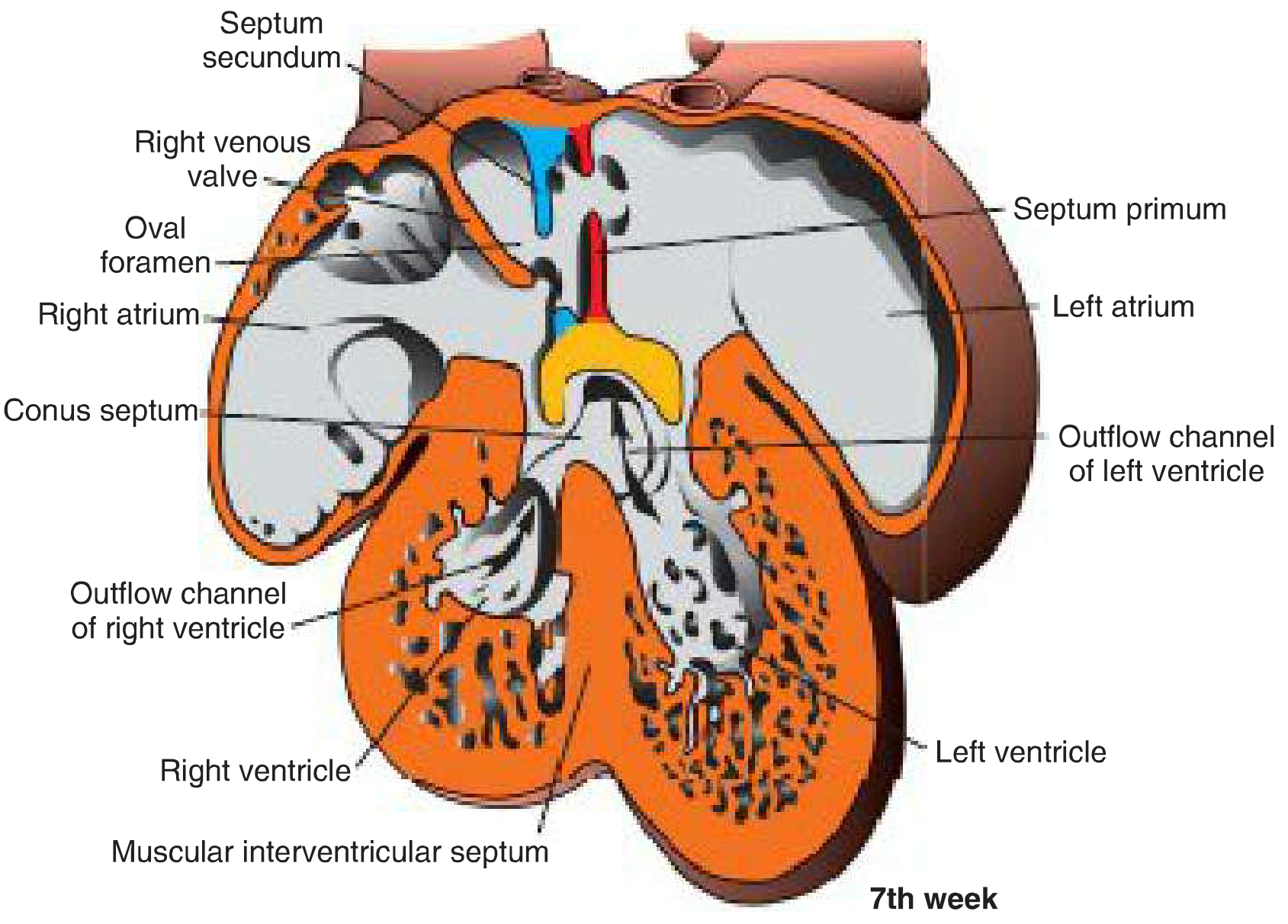
Stage 3: The Interventricular Foramen (Weeks 5-7)
Until the 7th week, a crescent-shaped interventricular foramen (IVF) sits between:
- The free (superior/concave) edge of the muscular IVS
- The fused endocardial cushions
This foramen allows right-left ventricular communication during development. It must be closed to complete cardiac septation.
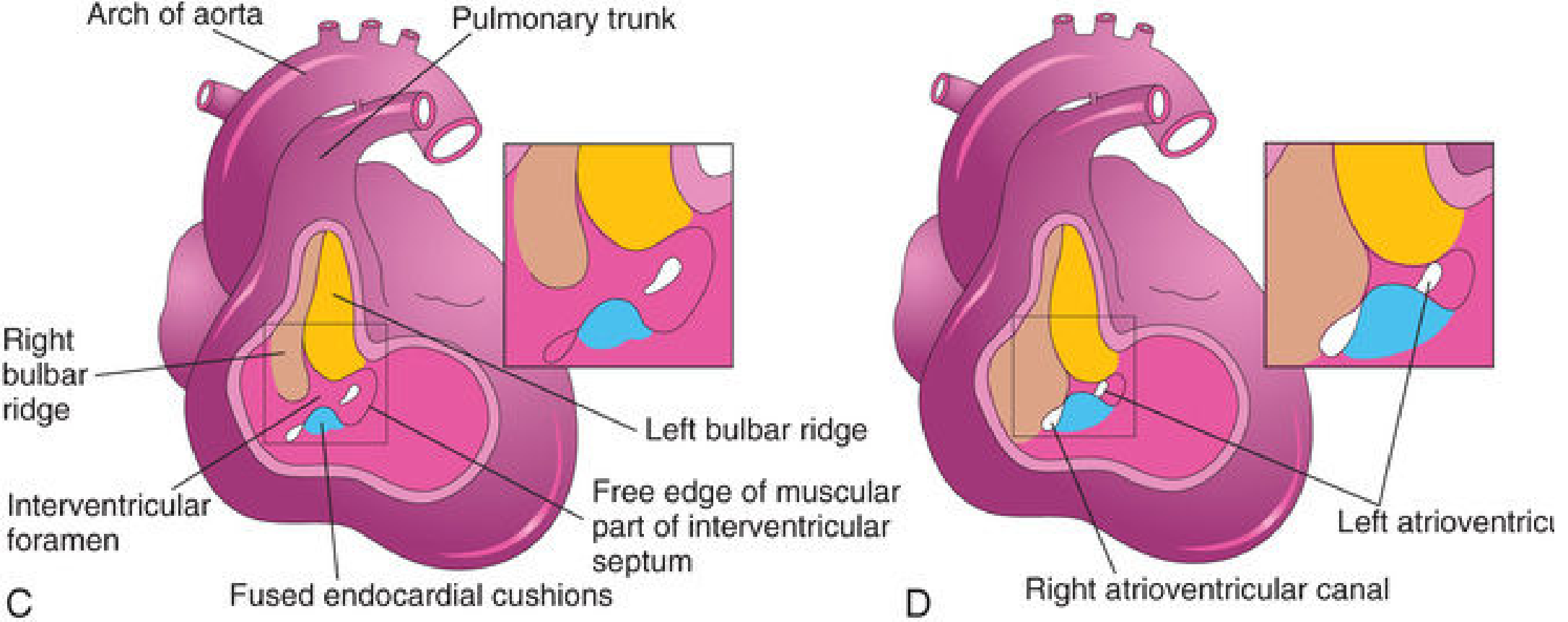
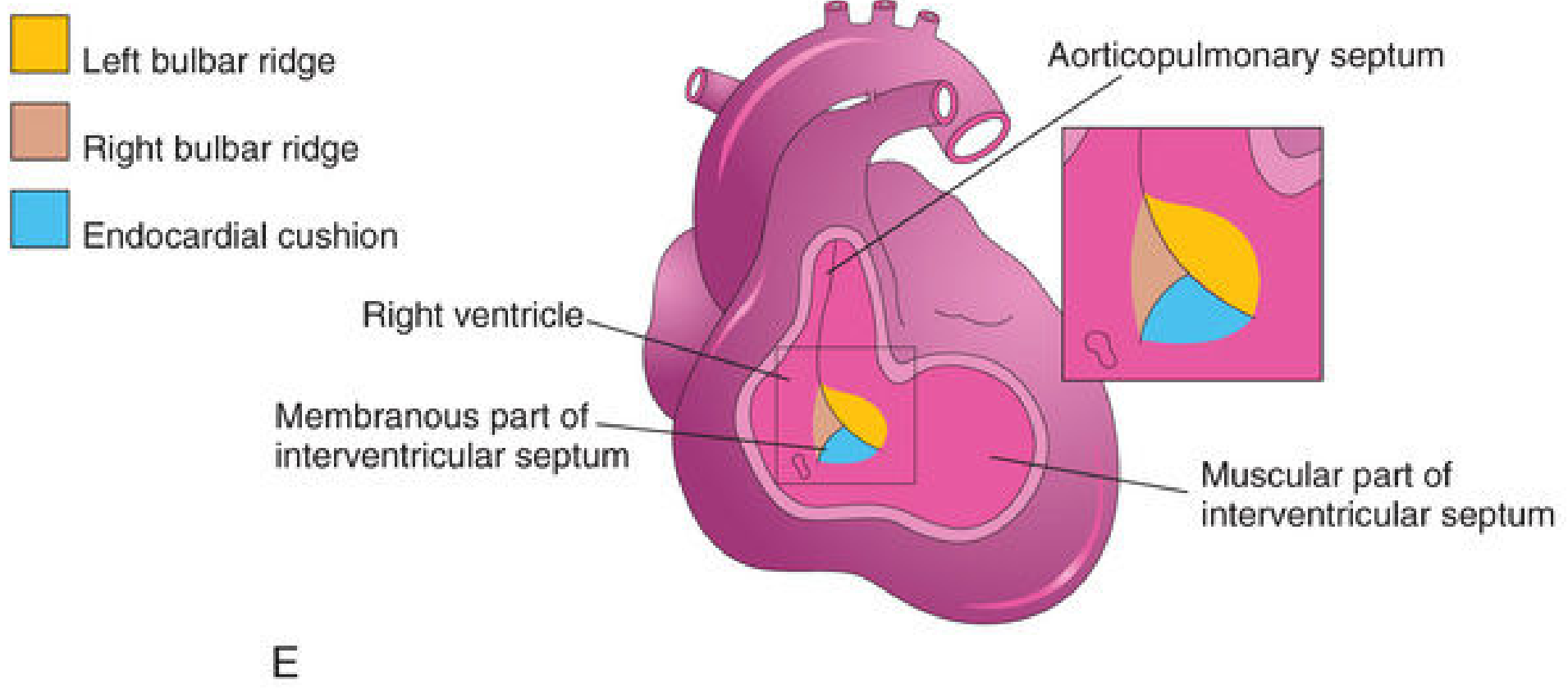
Stage 4: Closure of the Interventricular Foramen and Formation of the Membranous IVS (Week 7)
This is the most intricate step. The IVF closes by the end of the 7th week through fusion of tissue from three sources:
| Source | Contribution |
|---|---|
| Right bulbar ridge | Contributes to the membranous IVS from the right side |
| Left bulbar ridge | Contributes to the membranous IVS from the left side |
| Endocardial cushion | Subendocardial tissue extends from the right side of the endocardial cushion downward along the top of the muscular IVS |
These three tissues merge with each other and with the aorticopulmonary septum, completing the membranous part of the IVS.
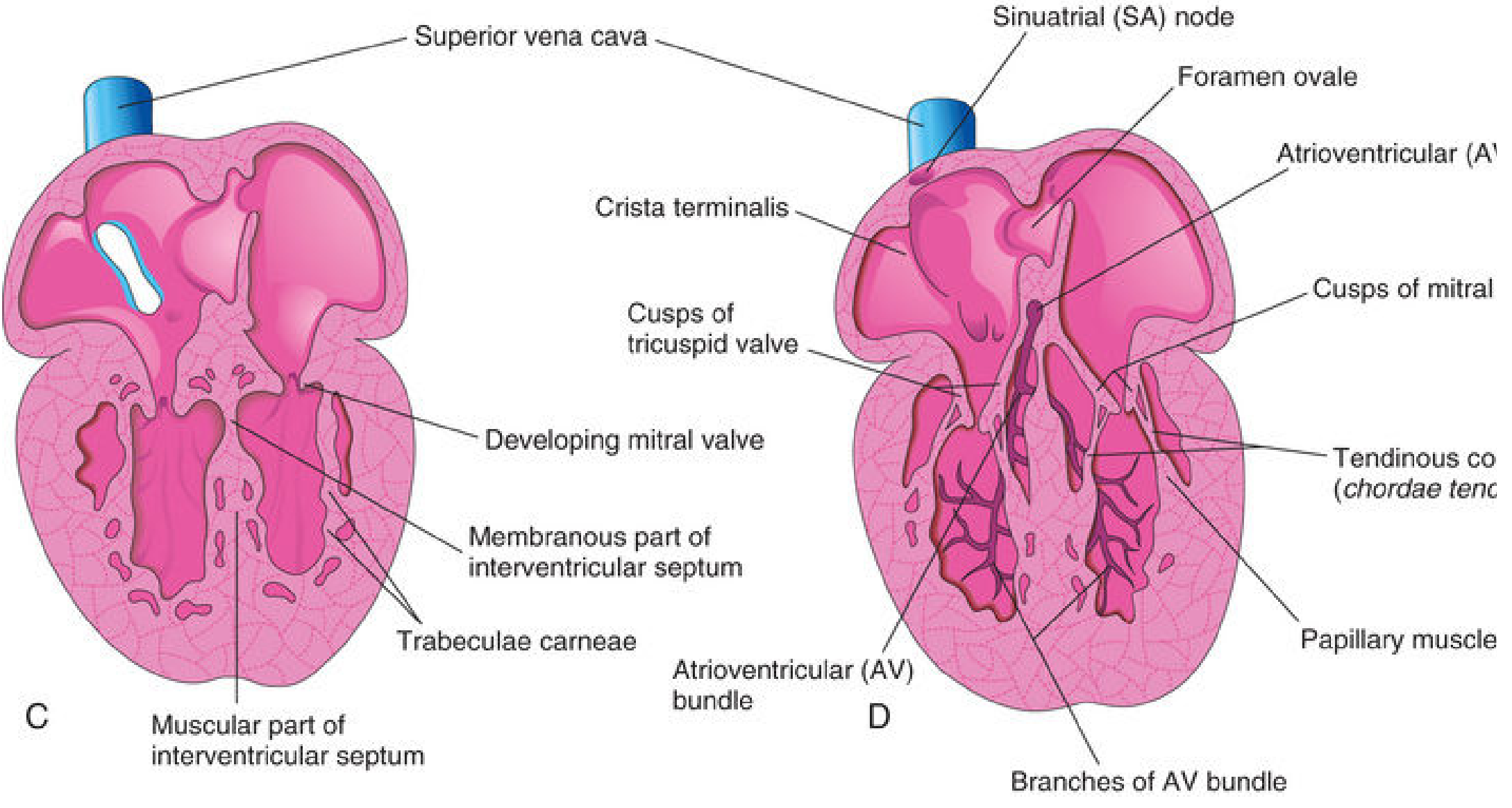
The Final IVS: Two Parts
After closure is complete, the IVS has two distinct regions:
1. Muscular Part (larger, inferior)
- Thick, myocardium-rich
- Formed by fusion of the medial walls of the expanding left and right ventricles
- Has trabeculations on its surfaces
2. Membranous Part (smaller, superior)
- Thin, fibrous, located in the upper-posterior IVS
- Derived from fusion of: right bulbar ridge + left bulbar ridge + endocardial cushion tissue + neural crest cells
- The most common site of ventricular septal defects
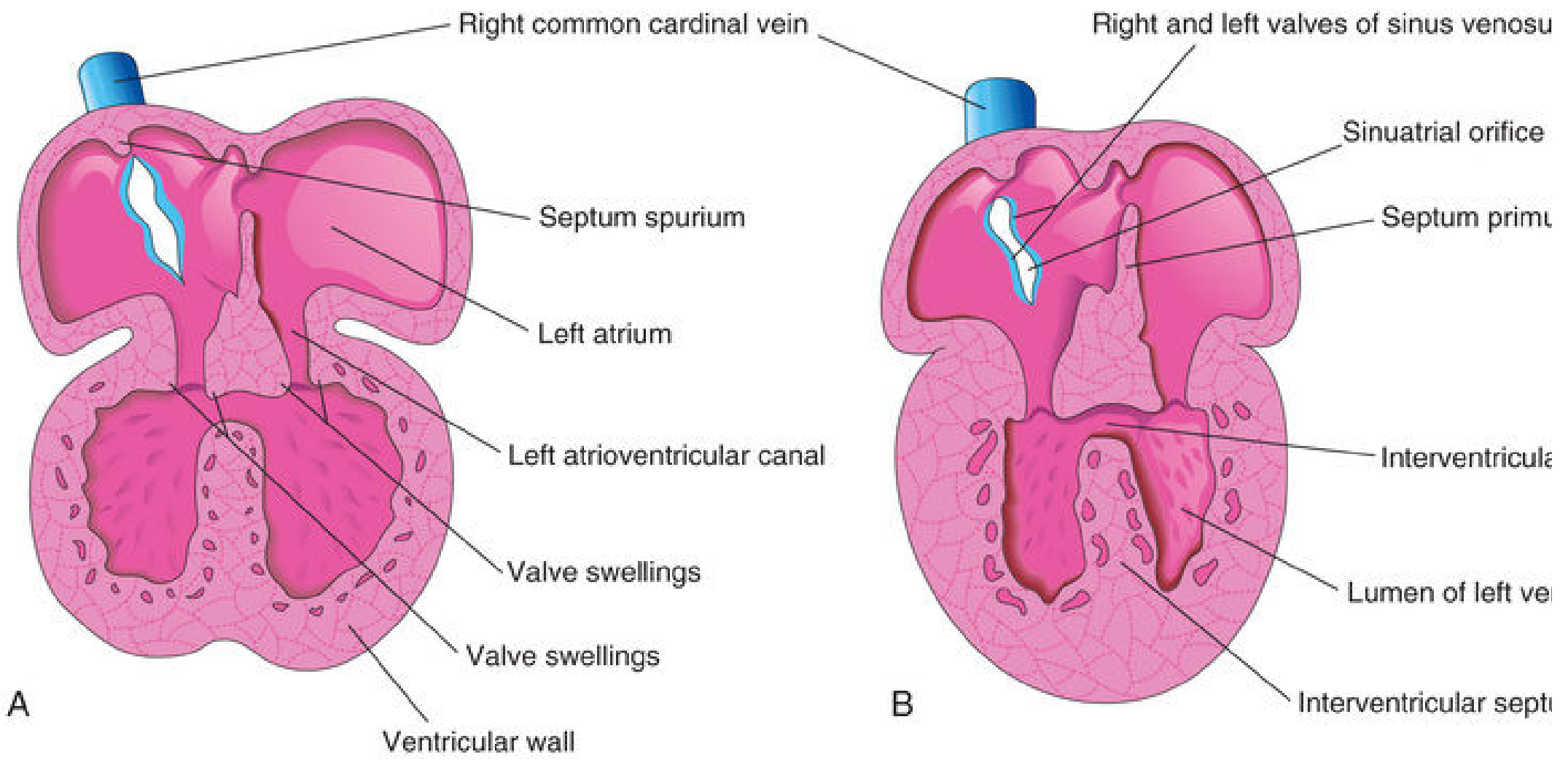
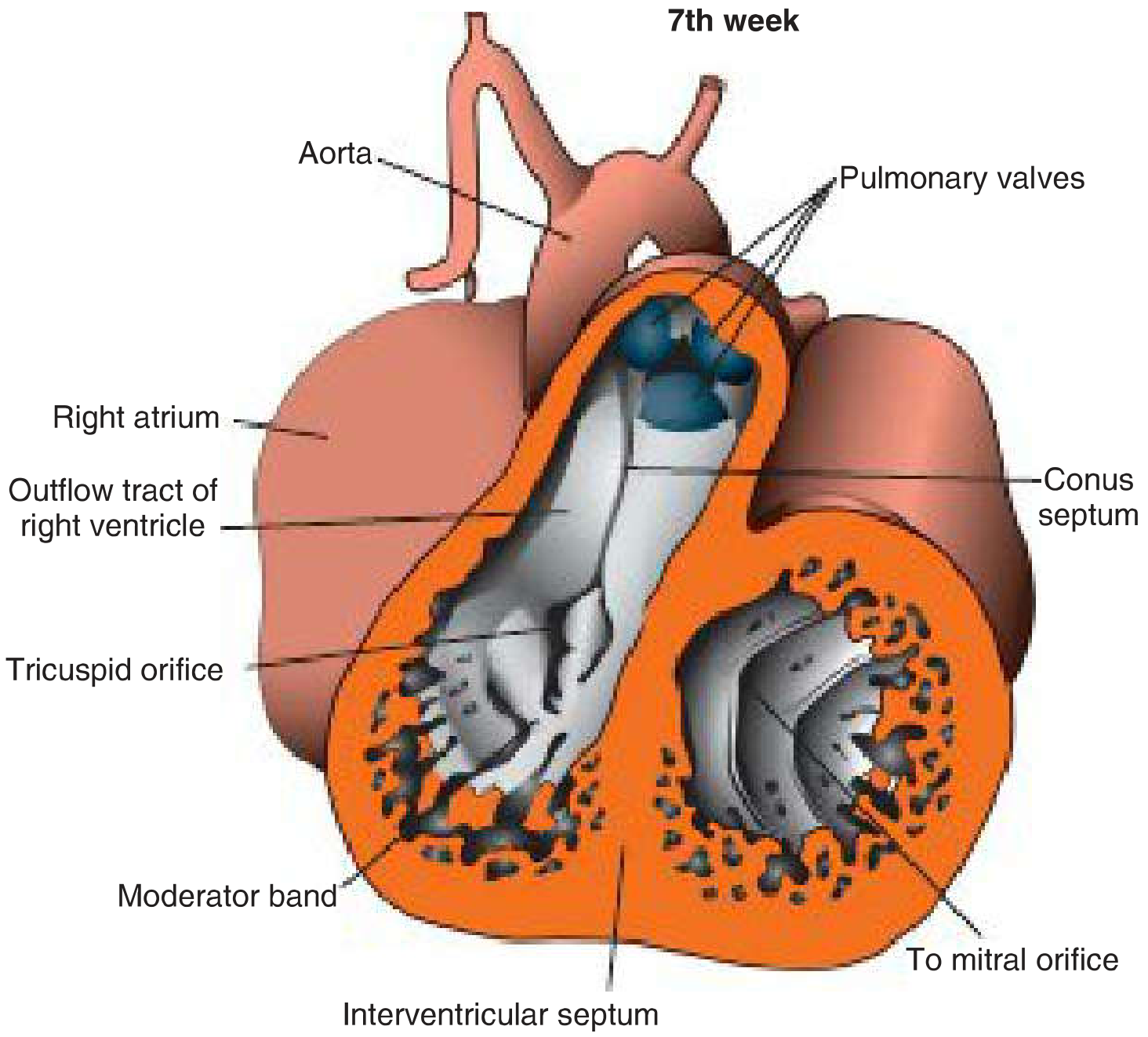
Langman's View: 7th-Week Cross-Section
Summary Timeline
| Week | Event |
|---|---|
| Week 4 | Primordial ventricle expands; medial walls begin merging → primordial muscular IVS appears at the apex |
| Weeks 4-6 | Muscular IVS grows upward; interventricular foramen remains open (crescent-shaped gap) |
| Week 6 | Bulbar ridges begin fusing; endocardial cushion tissue starts extending toward the IVS |
| Week 7 | IVF closes completely; membranous IVS formed from right bulbar ridge + left bulbar ridge + endocardial cushion; aorta and pulmonary trunk now connected to separate ventricles |
Clinical Correlation: Ventricular Septal Defects (VSDs)
VSDs are the most common congenital heart defect, accounting for ~25% of all CHDs.
| Type | Cause | Frequency |
|---|---|---|
| Membranous VSD | Failure of subendocardial tissue extension from endocardial cushion to fuse with the aorticopulmonary septum and muscular IVS | Most common (~80%) |
| Muscular VSD | Excessive cavitation of myocardial tissue during ventricular wall formation; can produce multiple small holes ("Swiss cheese" septum) | Less common |
| Single ventricle (cor triloculare) | Complete failure of IVS formation | Extremely rare |
Small VSDs (30-50%) close spontaneously in the first year of life. Large VSDs cause left-to-right shunting, increased pulmonary blood flow, pulmonary hypertension, dyspnea, and early cardiac failure.
Key memory point: The membranous IVS is the product of three-way fusion - right bulbar ridge + left bulbar ridge + endocardial cushion. Failure of any one of these to meet properly leaves a membranous VSD. - The Developing Human, p. 813-815; Langman's Medical Embryology, p. 219-220
This is a shared conversation. Sign in to Orris to start your own chat.