Neuroraphy in orthopaedics 10 marks pg answer with flow chart and images
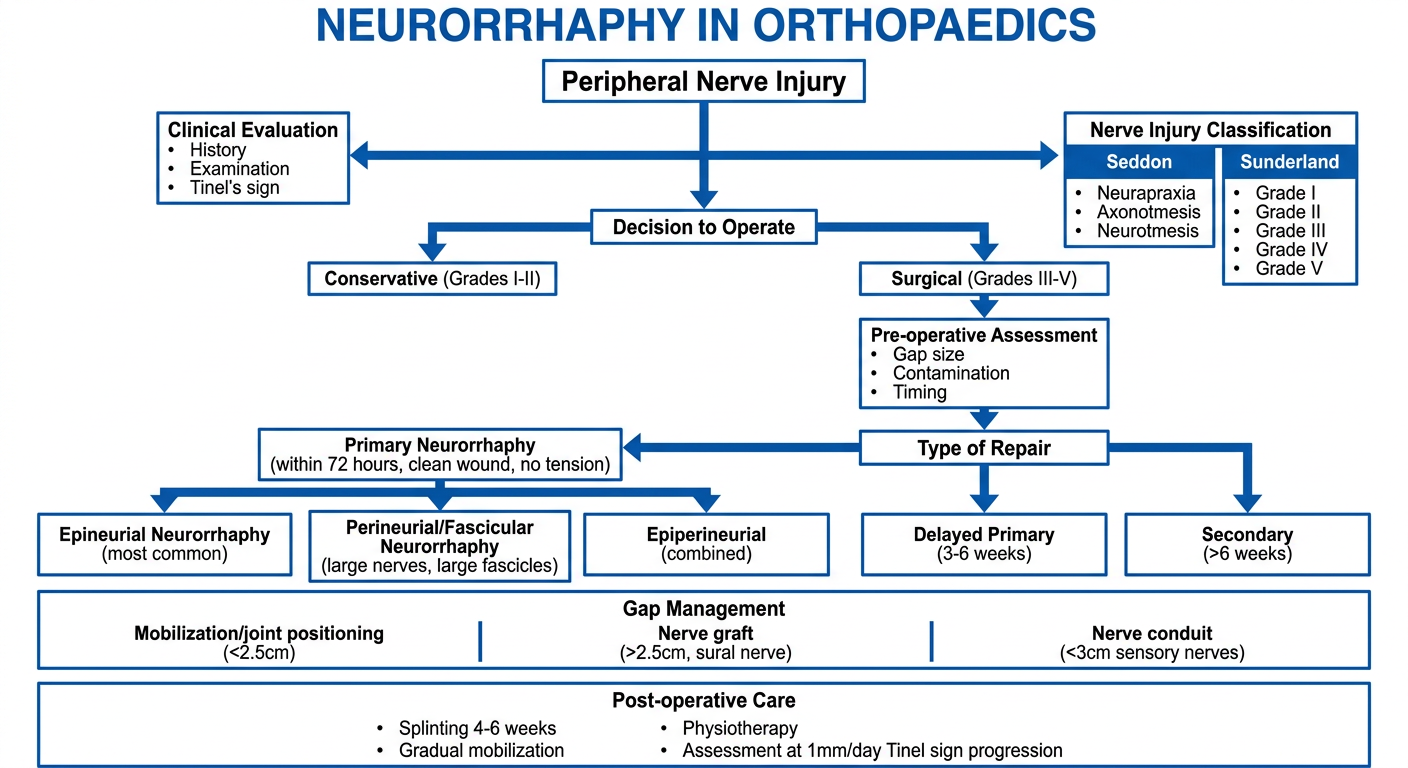
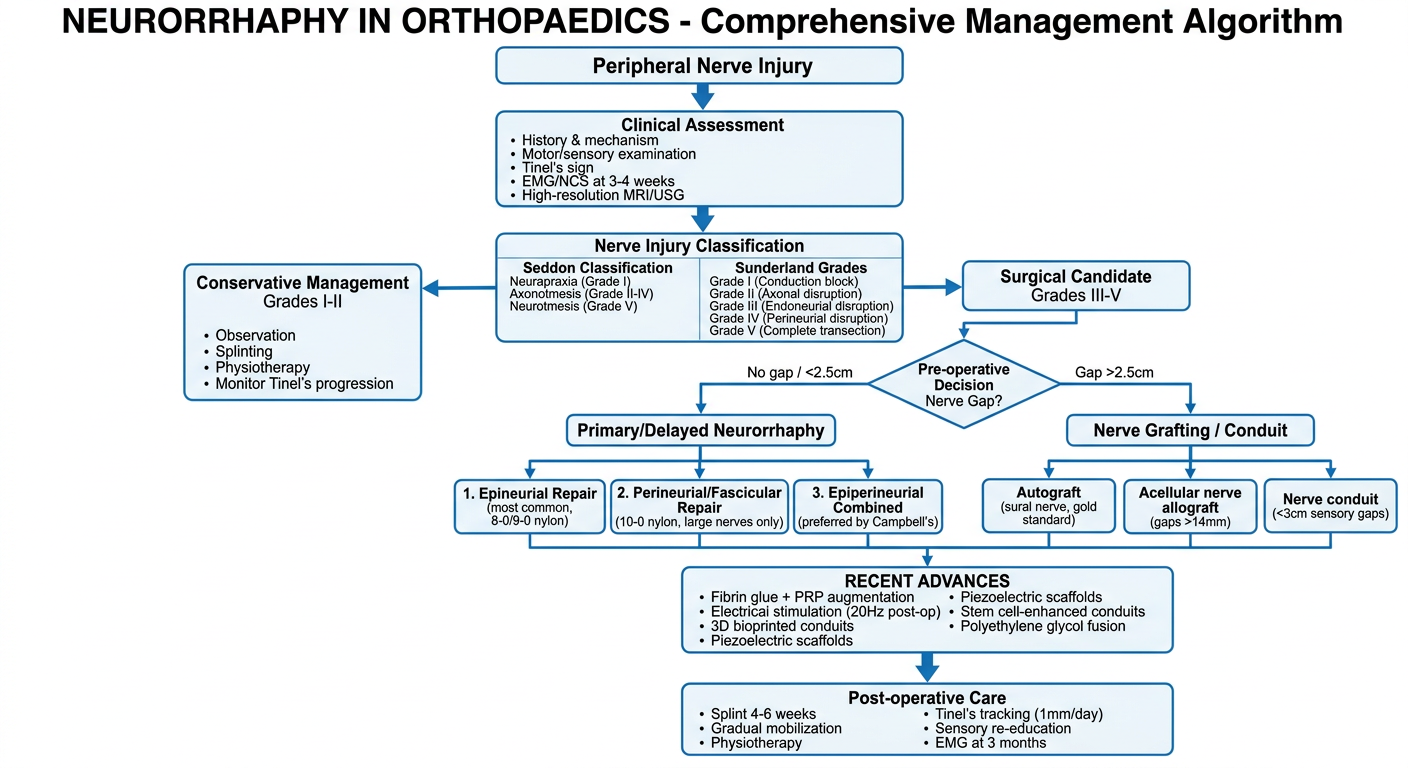
A detailed medical flowchart titled "NEURORRHAPHY IN ORTHOPAEDICS" showing the decision-making algorithm for peripheral nerve repair. The flowchart starts at the top with "Peripheral Nerve Injury" which branches into assessment steps: "Clinical Evaluation (History, Examination, Tinel's sign)" then "Nerve Injury Classification" showing Seddon (Neurapraxia, Axonotmesis, Neurotmesis) and Sunderland (Grade I-V). This flows to "Decision to Operate" with branches for "Conservative (Grades I-II)" and "Surgical (Grades III-V)". The surgical branch leads to "Pre-operative Assessment: Gap size, Contamination, Timing". Then to "Type of Repair" with three branches: "Primary Neurorrhaphy (within 72 hours, clean wound, no tension)", "Delayed Primary (3-6 weeks)", and "Secondary (>6 weeks)". The primary neurorrhaphy branch splits into "Epineurial Neurorrhaphy (most common)" and "Perineurial/Fascicular Neurorrhaphy (large nerves, large fascicles)" and "Epiperineurial (combined)". Below this shows "Gap Management" with options: "Mobilization/joint positioning (<2.5cm)", "Nerve graft (>2.5cm, sural nerve)", "Nerve conduit (<3cm sensory nerves)". Final box shows "Post-operative Care: Splinting 4-6 weeks, Gradual mobilization, Physiotherapy, Assessment at 1mm/day Tinel sign progression". Clean medical diagram style with blue and white color scheme.
NEURORRHAPHY IN ORTHOPAEDICS
DEFINITION
FLOWCHART: DECISION ALGORITHM FOR NEURORRHAPHY
CLASSIFICATION OF NERVE INJURIES (Prerequisite to Repair Decision)
| Seddon | Sunderland | Pathology | Spontaneous Recovery |
|---|---|---|---|
| Neurapraxia | Grade I | Conduction block only | Complete, weeks |
| Axonotmesis | Grade II | Axon disrupted, endoneurium intact | Yes, 1 mm/day |
| Axonotmesis | Grade III | Endoneurium disrupted | Partial |
| Axonotmesis | Grade IV | Perineurium disrupted | None without surgery |
| Neurotmesis | Grade V | Complete nerve division | None without surgery |
TIMING OF REPAIR
| Type | Timing | Indication |
|---|---|---|
| Primary | Within 6-8 hours | Clean sharp wounds, no tension, healthy tissue |
| Delayed Primary | 3-6 weeks | Contaminated or crush wounds; allows demarcation of viable tissue |
| Secondary | >3-6 months | Missed injuries, failed primaries |
PREREQUISITES FOR NEURORRHAPHY
- Clean, well-vascularized wound bed
- No tension at the repair site
- Healthy nerve ends (confirmed by serial cuts until normal fasciculi are visible under microscope)
- Use of magnification (operating microscope or loupes)
- Meticulous hemostasis
- Non-reactive, non-absorbable suture material (monofilament nylon)
TYPES OF NEURORRHAPHY
1. EPINEURIAL NEURORRHAPHY (Most Common)
- Expose and dissect the nerve ends; confirm the gap can be closed without tension
- Resect the neuroma/glioma with a sharp razor blade or diamond-bladed knife against a sterile wooden tongue depressor (nerve miter box)
- Make serial 1-mm cuts until normal fasciculi are visible under the operating microscope
- Control bleeding with thrombin or gelatin sponges
- Determine rotational alignment using surface vessels and fascicular patterns; place epineurial orientation sutures 1 cm from each cut edge
- Place a rubber/plastic background under the nerve for contrast
- Place first suture on the deep (posterior) surface of the epineurium and leave it long for easier rotation
- Place sutures in all four quadrants, then add sufficient interrupted 8-0 or 9-0 monofilament nylon to complete the repair
- Before closure, assess tension through range of motion to guide postoperative mobilization
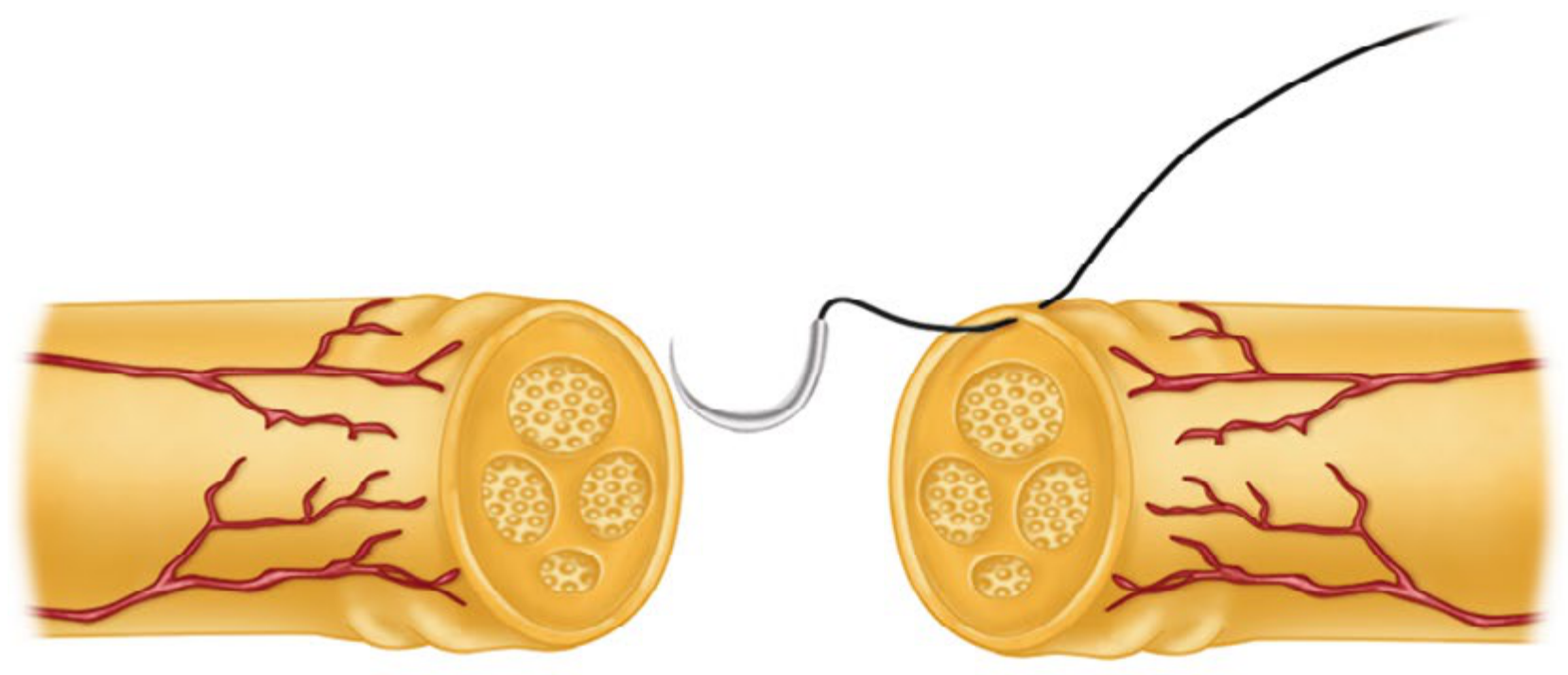
A: Nerve ends trimmed, fascicles identified. B: Epineurial suture placed through matching fascicular site. C: Repair completed.
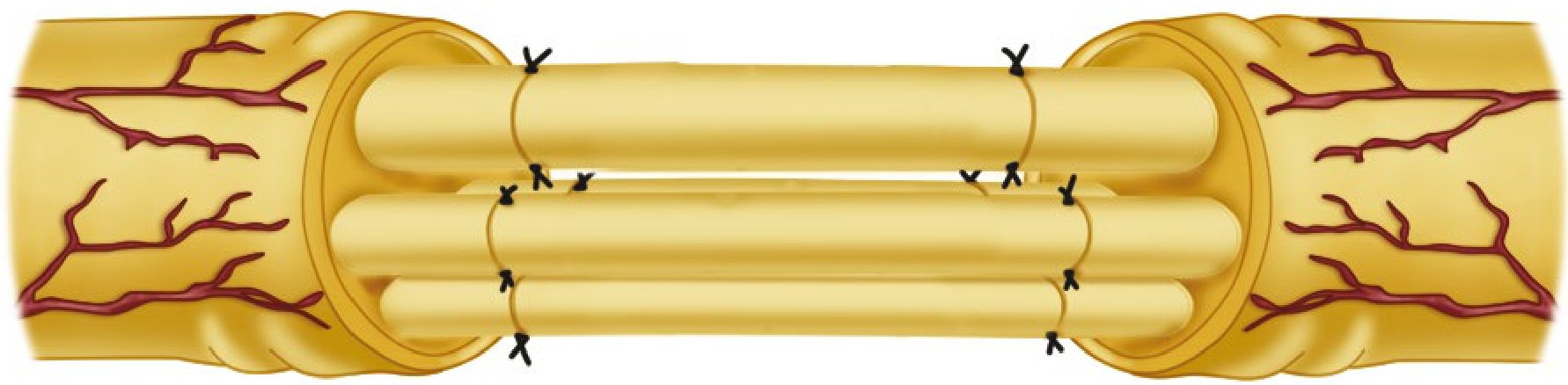
2. PERINEURIAL (FASCICULAR) NEURORRHAPHY
- Surgeon must be proficient with the operating microscope and 10-0 suture
- Resect nerve ends as for epineurial repair
- Place nerve ends in proper rotational alignment
- Under magnification, identify corresponding fascicular groups in proximal and distal stumps (diagram the arrangement on sterile paper)
- Incise the epineurium longitudinally to expose fasciculi
- Approximate corresponding fasciculi individually with interrupted 9-0 or 10-0 nylon sutures
- Typically 2 sutures per fascicle are sufficient
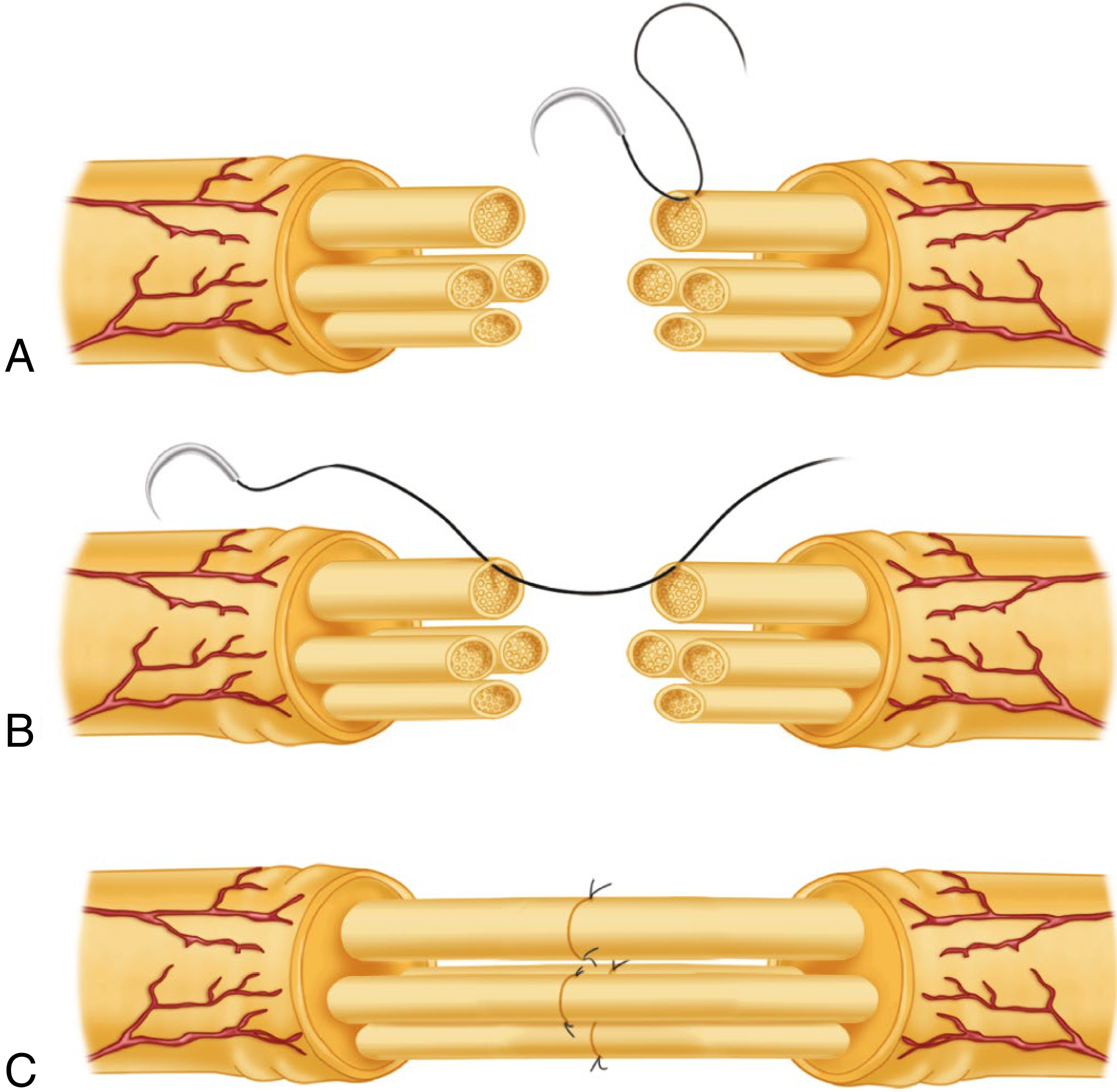
A: Epineurium excised, fascicles exposed. B: Suture passed through corresponding fascicles on either side. C: Neurorrhaphy completed, usually with two 10-0 nylon sutures per fascicle.
3. EPIPERINEURIAL (COMBINED) NEURORRHAPHY
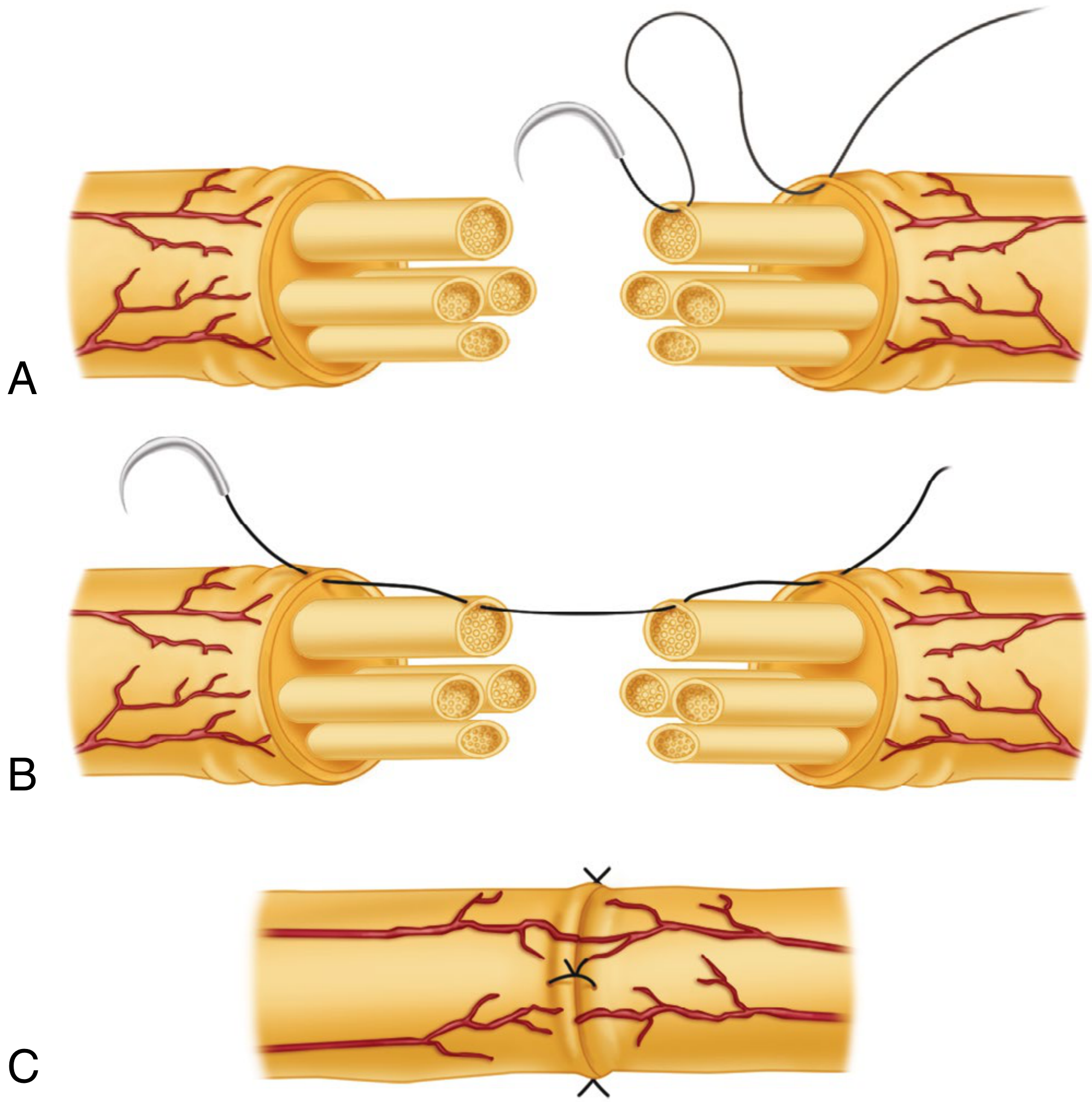
A: Epineurium excised/retracted; sutures placed through epineurium near large peripheral fascicle and through its perineurium. B: Suture passed through matching fascicle on opposite cut surface. C: Repair completed.
4. PARTIAL NEURORRHAPHY
- If >50% of a large nerve (especially sciatic or brachial plexus) is disrupted - partial neurorrhaphy is advisable
- If stimulation of remaining fascicles shows good motor response, do NOT risk injuring intact fascicles (e.g., peroneal or ulnar) just to restore sensation
GAP MANAGEMENT
| Gap Size | Method |
|---|---|
| <2.5 cm | Nerve mobilization, joint flexion positioning |
| >2.5 cm (motor nerves) | Nerve grafting (interfascicular - sural nerve donor) |
| <3 cm (sensory nerves) | Nerve conduit (collagen tube) |
| >14 mm | Acellular nerve allograft outperforms conduits |
SUTURE MATERIALS
| Technique | Suture Size |
|---|---|
| Epineurial (large nerves) | 8-0 monofilament nylon |
| Epineurial (wrist/hand level) | 9-0 monofilament nylon (optimal tension) |
| Perineurial (fascicular) | 9-0 or 10-0 monofilament nylon |
POSTOPERATIVE CARE
- Immobilization: Plaster splint/cast for 4-6 weeks
- Upper extremity: posterior molded plaster splint x 4 weeks
- Shoulder involvement: Velpeau dressing + plaster
- Lower extremity (sciatic/peroneal): spica cast x 6 weeks minimum
- Wound review: Day 7-10, suture removal
- Mobilization: Gradual extension over 2-3 weeks after cast removal
- Lower limb: Long leg brace controlling knee extension after cast removal
- Physiotherapy: Active and passive range of motion; sensory re-education
FACTORS AFFECTING RESULTS
| Favorable | Unfavorable |
|---|---|
| Young age | Delayed repair (>3 months) |
| Distal nerve level | Proximal injury (long regeneration distance) |
| Sharp clean injury | Avulsion/crush injury |
| Early repair | Contaminated wound |
| Good fascicular matching | Poor rotational alignment |
| Tension-free repair | Tension at repair site |
KEY PRINCIPLES SUMMARY
- Tension-free repair is the single most important technical principle
- Fascicular alignment prevents wasteful misdirection of regenerating axons (around 50% of axons fail to cross even a well-performed repair site)
- Magnification (operating microscope) is mandatory for all neurorrhaphy
- Monofilament non-absorbable nylon remains the gold standard suture
- Literature has NOT shown perineurial repair to be superior to epineurial repair; at most institutions, epineurial repair is preferred to limit suture bulk trauma
- Sunderland's conditions for fascicular repair: (1) large enough fascicular groups, (2) wasteful regeneration likely with epineurial repair, (3) fascicular groups occupy constant positions (median/ulnar at wrist, radial at elbow)
Include recent advances and generate new one
neurorrhaphy peripheral nerve repair recent advances
nerve repair conduit scaffold regeneration orthopaedic
recent advances neurorrhaphy nerve repair 2023 2024 2025 fibrin glue electrical stimulation polyethylene glycol
PMID: 41948775
https://link.springer.com/article/10.1186/s12967-025-07567-z
PMID: 39025114
A detailed professional medical flowchart titled "NEURORRHAPHY IN ORTHOPAEDICS - Comprehensive Management Algorithm" with clean clinical design. TOP: "Peripheral Nerve Injury" box ↓ "Clinical Assessment" box with bullet points: History & mechanism, Motor/sensory examination, Tinel's sign, EMG/NCS at 3-4 weeks, High-resolution MRI/USG ↓ "Nerve Injury Classification" box showing two columns: LEFT: Seddon Classification - Neurapraxia (Grade I), Axonotmesis (Grade II-IV), Neurotmesis (Grade V). RIGHT: Sunderland Grades I through V with brief description ↓ splits into two branches: LEFT branch: "Conservative Management" for Grades I-II: Observation, Splinting, Physiotherapy, Monitor Tinel's progression RIGHT branch: "Surgical Candidate" for Grades III-V RIGHT branch continues ↓ "Pre-operative Decision" diamond: "Nerve Gap?" - "No gap / <2.5cm" → "Primary/Delayed Neurorrhaphy" - "Gap >2.5cm" → "Nerve Grafting / Conduit" "Primary/Delayed Neurorrhaphy" splits into 3 boxes: 1. Epineurial Repair (most common, 8-0/9-0 nylon) 2. Perineurial/Fascicular Repair (10-0 nylon, large nerves only) 3. Epiperineurial Combined (preferred by Campbell's) "Nerve Grafting/Conduit" splits into: - Autograft (sural nerve, gold standard) - Acellular nerve allograft (gaps >14mm) - Nerve conduit (<3cm sensory gaps) Both merge into "RECENT ADVANCES" box containing: Fibrin glue + PRP augmentation, Electrical stimulation (20Hz post-op), 3D bioprinted conduits, Piezoelectric scaffolds, Stem cell-enhanced conduits, Polyethylene glycol fusion ↓ Final box: "Post-operative Care" - Splint 4-6 weeks, Gradual mobilization, Physiotherapy, Tinel's tracking (1mm/day), Sensory re-education, EMG at 3 months Blue and white color scheme, medical diagram style, clear arrows, professional typography
NEURORRHAPHY IN ORTHOPAEDICS
10-Mark PG Answer with Recent Advances
COMPREHENSIVE MANAGEMENT FLOWCHART
1. DEFINITION
2. NERVE INJURY CLASSIFICATION
| Seddon | Sunderland | Pathology | Recovery |
|---|---|---|---|
| Neurapraxia | Grade I | Conduction block; no structural damage | Spontaneous, weeks |
| Axonotmesis | Grade II | Axon disrupted; endoneurium intact | Spontaneous, 1 mm/day |
| Axonotmesis | Grade III | Endoneurium disrupted | Partial, may need surgery |
| Axonotmesis | Grade IV | Perineurium disrupted | No spontaneous; surgery needed |
| Neurotmesis | Grade V | Complete division | No spontaneous; surgery needed |
Neurorrhaphy is indicated for Sunderland Grade III-V injuries.
3. DIAGNOSIS AND ASSESSMENT
- Clinical: Motor/sensory deficit, Tinel's sign progression (1 mm/day = healthy regeneration)
- EMG/NCS: At 3-4 weeks to confirm denervation and assess prognosis
- Imaging: High-resolution MRI neurography and ultrasound - can identify neuroma-in-continuity, scarring, and gap length
4. TIMING OF NEURORRHAPHY
| Type | Timing | Indication |
|---|---|---|
| Primary | Within 6-8 hours | Clean sharp wound, tension-free, healthy tissue |
| Delayed primary | 3-6 weeks | Contaminated/crush wounds; allows tissue demarcation |
| Secondary | 3-6 months | Missed injuries, failed primary repairs |
5. PREREQUISITES FOR NEURORRHAPHY
- Clean, well-vascularized wound bed
- No tension at repair site
- Healthy nerve ends confirmed by serial 1-mm cuts under operating microscope
- Magnification (operating microscope or minimum 3.5x loupes)
- Non-reactive, non-absorbable monofilament nylon suture
- Meticulous hemostasis
6. TYPES OF NEURORRHAPHY (Surgical Techniques)
A. EPINEURIAL NEURORRHAPHY (Most Common)
- Expose nerve, confirm tension-free closure is possible
- Resect neuroma/glioma: serial 1-mm cuts with razor blade or diamond knife in a nerve miter box until normal fasciculi are visible
- Achieve rotational alignment using surface vessels and fascicular patterns; place epineurial orientation sutures 1 cm proximal and distal to cut
- Place rubber/plastic background beneath nerve for suture contrast
- Begin with a deep (posterior) epineurial suture (8-0 or 9-0 nylon), leave long for rotation
- Place sutures in all 4 quadrants, then add sufficient interrupted sutures for a watertight repair
- Assess repair tension through range of motion before wound closure
B. PERINEURIAL (FASCICULAR) NEURORRHAPHY
- Requires operating microscope proficiency and ease with 10-0 suture
- Resect nerve ends as above
- Diagram fascicular arrangement on sterile paper
- Incise epineurium longitudinally to expose fasciculi
- Approximate corresponding fasciculi with interrupted 9-0 or 10-0 nylon (2 sutures per fascicle)
C. EPIPERINEURIAL (COMBINED) NEURORRHAPHY
Literature has not shown perineurial repair to be superior to epineurial repair. Epineurial repair is preferred at most centers to limit foreign material inside the nerve.
D. PARTIAL NEURORRHAPHY
7. GAP MANAGEMENT
| Gap | Method |
|---|---|
| < 2.5 cm | Nerve mobilization + joint flexion positioning |
| > 2.5 cm (motor nerves) | Interfascicular nerve grafting (sural nerve) |
| < 3 cm (sensory nerves) | Nerve conduit (collagen or synthetic tube) |
| Gaps < 14 mm | Conduit achieves MRC S3+ in 67% of digital nerve reconstructions |
| Gaps > 14 mm | Acellular nerve allograft outperforms synthetic conduits |
8. SUTURE MATERIALS AND SIZE
| Level | Suture |
|---|---|
| Large nerve trunks (epineurial) | 8-0 monofilament nylon |
| Wrist and hand level | 9-0 monofilament nylon (optimal tension setting) |
| Fascicular repair | 9-0 or 10-0 monofilament nylon |
9. POSTOPERATIVE CARE
- Immobilization: 4 weeks for upper extremity; 6 weeks spica cast for sciatic/peroneal repairs
- Wound review: Day 7-10; suture removal
- Mobilization: Gradual extension over 2-3 weeks after cast/splint removal; long leg brace for lower limb
- Physiotherapy: Active-passive ROM, sensory re-education, desensitization
- Monitoring: Tinel's progression monthly (1 mm/day), EMG at 3 months
10. RECENT ADVANCES (2023-2026)
A. FIBRIN GLUE NEURORRHAPHY + PRP AUGMENTATION
- Fibrin glue neurorrhaphy (FGN) achieves comparable motor and sensory recovery to microsuture neurorrhaphy
- Shorter operative time and simpler technical execution
- When FGN is combined with platelet-rich plasma (PRP): faster functional recovery with no major complications
- PRP provides neuroprotective, anti-inflammatory, and neurotrophic support for axonal regeneration
B. ELECTRICAL STIMULATION (ES) - MOST PROMISING ADVANCE
- Brief intraoperative electrical stimulation (20 Hz, 1 hour, immediately post-neurorrhaphy) accelerates axonal sprouting and Schwann cell activity
- Stimulation promotes: increased Schwann cell proliferation, neurotrophic factor secretion, myelin production, and vascular growth
- Wireless piezoelectric scaffolds (PVDF-TrFE nanofibers): deliver localized electrical stimulation non-invasively without implanted batteries
- Graphene-based conductive scaffolds combined with ES show superior regeneration in 15-mm defect models
- Bordett et al. 2024: Ultrasound, laser, and magnetic stimulation are also being explored as adjuncts
C. ADVANCED NERVE CONDUITS AND SCAFFOLDS
| Generation | Material | Advantage |
|---|---|---|
| 1st gen | Silicone tubes | Mechanical protection only |
| 2nd gen | Collagen conduits (current standard) | Biodegradable, FDA-approved for <3 cm sensory gaps |
| 3rd gen (emerging) | Hyaluronic acid scaffolds | Aligned channels, anti-scarring properties |
| Cutting-edge | 3D bioprinted patient-specific conduits | Custom geometry, controlled porosity, dual electroactive properties |
- Hyaluronic acid-based conduits (2025): mechanistic advances in mimicking native extracellular matrix to guide axons
- Auxilium NeuroSpan Bridge trial (enrolled May 2025): scaffold-based peripheral nerve regeneration for long-gap injuries
D. STEM CELL-ENHANCED REPAIR
- Adipose-derived stem cells (ADSCs) embedded in polycaprolactone conduits: prevents muscle atrophy and restores innervation in 6-mm sciatic nerve defects
- iPSC-derived mesenchymal stem cells in 3D bioengineered conduits: superior morphology, function, and neurotrophic factor expression vs. silicone tubes
- Stem cell exosomes (cell-free approach): reduce risks of live cell transplantation while preserving neurotrophic and immunomodulatory effects
E. POLYETHYLENE GLYCOL (PEG) AXONAL FUSION
- PEG applied within 24 hours of sharp nerve transection can fuse divided axons directly, preventing Wallerian degeneration
- Ghergherehchi et al. (2023): PEG-fused hydrogel on viable transected nerve ends showed encouraging early results
- Less scarring than fibrin glue; comparable tensile strength
- Limitation: degrades slowly (up to 20 months at implant site); pressure on surrounding vasculature due to swelling
F. GENE THERAPY
- Targeted viral vector delivery of BDNF, GDNF, and NT-3 genes to Schwann cells to sustain neurotrophic support during long regeneration periods
- Genetic modification of Schwann cell phenotype to remain in a regeneration-supportive state for longer
- Currently pre-clinical only
G. IMPROVED IMAGING FOR DIAGNOSIS AND SURGICAL PLANNING
- High-resolution MRI neurography: identifies neuroma-in-continuity, fascicular injury patterns, and gap length preoperatively
- Intraoperative ultrasound: real-time fascicular mapping during repair
- AI-assisted image analysis: early identification of reinnervation patterns and treatment response monitoring
11. FACTORS AFFECTING OUTCOME
| Favorable | Unfavorable |
|---|---|
| Young age | Delayed repair (>3 months) |
| Distal level (hand/wrist) | Proximal injury (long regeneration to target) |
| Sharp clean transection | Avulsion / crush mechanism |
| Tension-free repair | Tension at repair site |
| Good fascicular alignment | Poor rotational orientation |
| Early physiotherapy | Muscle denervation >12-18 months |
| Use of PRP/ES adjuncts (emerging) | Heavy contamination |
12. SUMMARY TABLE - NEURORRHAPHY TYPES AT A GLANCE
| Type | Suture Layer | Suture Size | Best For |
|---|---|---|---|
| Epineurial | Epineurium only | 8-0 / 9-0 | Most peripheral nerves |
| Perineurial | Perineurium of fascicles | 10-0 | Large fascicular nerves (median/ulnar at wrist) |
| Epiperineurial | Both layers | 8-0 + 10-0 | Campbell's preferred technique |
| Partial | Partial nerve | As above | Partial nerve injuries (sciatic, brachial plexus) |
Key take-home points for PG exam:
- Tension-free repair is the single most important technical factor
- ~50% of regenerating axons fail to cross even a technically perfect repair site - this is why fascicular alignment matters
- Literature does NOT show fascicular repair superior to epineurial repair in clinical outcomes
- Fibrin glue + PRP = comparable outcomes to microsuture with shorter OR time (2026 systematic review)
- Brief intraoperative electrical stimulation (20 Hz, 1 hr) is the most promising emerging adjunct
- Axonal regeneration = 1 mm/day; track with Tinel's sign progression