Dermoid cyst
Reading File
Finding Sources
Finding Sources
Searching Images
dermoid cyst histology gross pathology
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive material. Here is a full clinical overview:
Dermoid Cyst
Definition and Pathogenesis
A dermoid cyst is an epithelial-lined congenital cyst formed by sequestration of ectodermal tissue along embryonic fusion planes during development. The cyst wall is lined by keratinizing stratified squamous epithelium and — critically — contains mature adnexal structures (pilosebaceous units, sweat glands, hair follicles, smooth muscle), which distinguishes it from an epidermoid cyst (no adnexal structures).
They are a separate entity from benign cystic teratomas (ovarian "dermoids"), which are neoplasms derived from all three germ layers. — Dermatology 2-Volume Set 5e
Classification
| Type | Origin | Notes |
|---|---|---|
| Congenital/inclusion dermoid | Fusion plane entrapment | Most common; head/neck, periorbital, midline |
| Tubulodermoid | Entrapment around embryonic tubular structures | Spinal/sacral region |
| Implantation (acquired) dermoid | Traumatic implantation of surface ectoderm | Fingertip/hand after thorn prick or needle injury |
| Ovarian (mature cystic teratoma) | Germ cell origin | Neoplasm — see below |
Cutaneous / Craniofacial Dermoid Cysts
Sites
Occur along embryonic closure zones:
- Lateral eyebrow (external angular dermoid) — most common
- Nasal root / dorsum of nose (fistula of the dorsum of the nose)
- Midline forehead, scalp (frontal → occipital)
- Mastoid process, floor of mouth, neck midline
- Chest, back, abdomen, perianal/sacral area, scrotum
Clinical Features
- Firm, non-compressible, non-pulsatile subcutaneous nodule, 1–4 cm
- Does not transilluminate
- Mobile under skin but often tethered to underlying periosteum
- No attachment to overlying skin
- A punctum or hair-tufted pit may be present → signifies underlying sinus
- Present within first year of life; 70% identified by age 5
Intracranial Extension ⚠️
- Nasal and midline scalp dermoids have ~25% overall risk of intracranial extension
- If a sinus ostium is present → risk rises to ~50%
- A nasal dermoid may extend to widen the nasal bridge
- Spinal dermoid/sinus may connect to subarachnoid space → risk of meningitis
- Intracranial dermoids can rupture → chemical meningitis or hydrocephalus from keratinous/sebaceous CSF contamination
Nasal and eyebrow dermoids may run in families (genetic component).
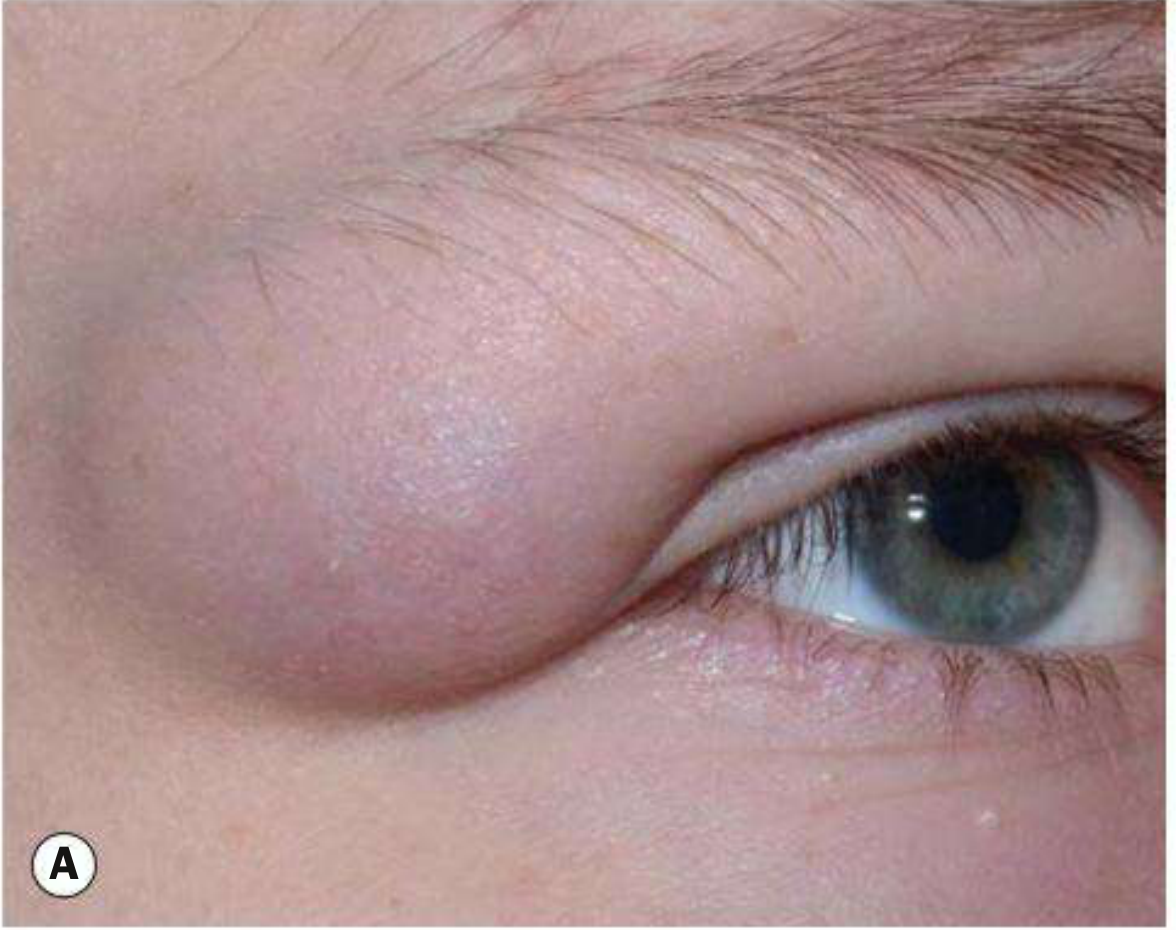
Orbital Dermoid Cyst
An orbital dermoid is a choristoma — histologically normal tissue in an abnormal location — displaced ectoderm along embryonic lines of closure.
Superficial vs. Deep
| Feature | Superficial | Deep |
|---|---|---|
| Presentation | Infancy; painless nodule | Adolescence/adult; proptosis or acute inflamed orbit |
| Location | Superotemporal > superonasal orbit | Posterior to orbital septum |
| Exam | Firm, 1–2 cm, mobile, posterior margin palpable | Proptosis, dystopia, indistinct posterior margins |
| Imaging | Well-circumscribed heterogeneous cystic lesion | Well-circumscribed; may extend intracranially via bony defect |
Treatment: Excision in toto. Take care not to rupture the cyst wall — leakage of keratin causes severe granulomatous inflammation in surrounding tissue.
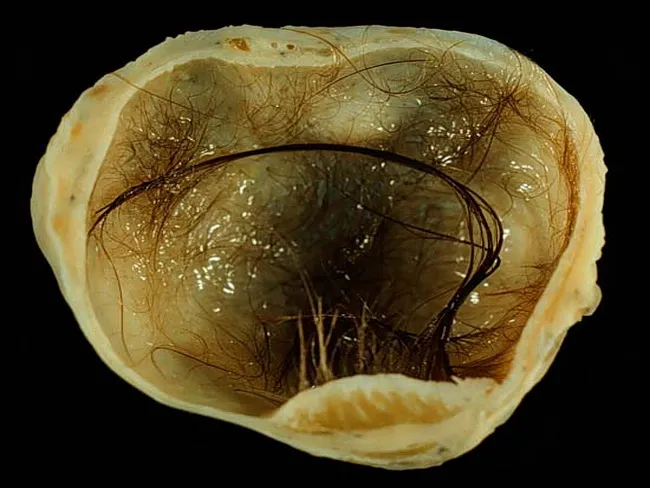
Histopathology
- Wall: keratinizing stratified squamous epithelium
- Contents: keratin debris, hair shafts, sebaceous material
- Wall structures: pilosebaceous units, apocrine/eccrine glands, smooth muscle bundles
- Portions of the wall may show a "shark tooth" (wavy eosinophilic) pattern resembling steatocystoma — Andrews' Diseases of the Skin
Ovarian Dermoid Cyst (Mature Cystic Teratoma)
The most common benign ovarian neoplasm in reproductive-age women. Strictly a germ cell tumor containing tissues from all three germ layers, but dominated by ectodermal derivatives.
Key Features
- Contains: hair shafts, sebaceous material, teeth (odontogenic tissue), neural tissue
- Rokitansky protuberance (dermoid plug): mural nodule from which teeth and hair arise — pathognomonic on gross examination
- ~60% are clinically asymptomatic (found incidentally)
- Bilateral in ~10–15% of cases
Complications
- Ovarian torsion — most common complication
- Rupture → chemical peritonitis
- Infection
- Malignant transformation — rare (<2%), more common with advanced age
- Paraneoplastic anti-NMDA receptor encephalitis — when neural elements express NMDA-R antigens
Imaging
- Ultrasound: hyperechoic plug with posterior shadowing (Rokitansky protuberance); dermoid mesh pattern
- CT/MRI: fat attenuation/signal within the lesion is diagnostic; fat-fluid level, calcification (teeth)
Management
- Laparoscopic ovarian cystectomy — appropriate regardless of size; preserves fertility
- Oophorectomy — for larger cysts replacing the entire ovary
- Laparotomy — for very large cysts or when malignancy cannot be excluded
Cervical / Neck Dermoid
- Usually midline of the neck, asymptomatic
- Does not elevate with tongue protrusion (distinguishes from thyroglossal duct cyst, which does)
- May become acutely infected
- Treatment: Simple cystectomy after resolution of acute infection
Differential Diagnosis
| Lesion | Distinguishing Feature |
|---|---|
| Epidermoid cyst | No adnexal structures on histology |
| Pilonidal cyst | Midline sacral, symptomatic in adolescence |
| Thyroglossal duct cyst | Elevates with tongue protrusion/swallowing |
| Branchial cleft cyst | Lateral neck; lymphoid follicles on histology |
| Encephalocele | Pulsatile, compressible, impulse on coughing |
| Nasal glioma | No intracranial connection (usually) |
| Hemangioma | Vascular, compressible, may involute |
Imaging Guidelines
Preoperative imaging (CT first, followed by MRI if bony changes found) is mandatory before excision for:
- Midline nasal dermoids
- Midline scalp dermoids
- Posterior spinal dermoids
- Any lesion with a draining sinus ostium
Lateral eyebrow dermoids generally do not require pre-excision imaging.
Treatment Summary
| Site | Treatment |
|---|---|
| Periorbital/facial | Surgical excision in toto; neurosurgery consult if intracranial extension |
| Nasal/scalp midline | Preoperative CT/MRI mandatory; neurosurgery if CNS connection |
| Neck midline | Simple cystectomy |
| Spinal | MRI to exclude tethered cord; neurosurgical excision |
| Ovarian | Laparoscopic cystectomy; oophorectomy for large/whole-ovary replacement |
Sources: Andrews' Diseases of the Skin, p. 780 | Fitzpatrick's Dermatology, Vol. 1–2 | Dermatology 2-Volume Set 5e | Kanski's Clinical Ophthalmology 10th | Sabiston Textbook of Surgery | Cummings Otolaryngology | K.J. Lee's Essential Otolaryngology
This is a shared conversation. Sign in to Orris to start your own chat.