Mitral valve stenosis
Reading File
Finding Sources
Searching PubMed
"mitral stenosis" management
Reading File
Reading File
Searching Images
mitral stenosis echocardiography pathology
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of Mitral Valve Stenosis (MS) based on Harrison's Principles of Internal Medicine 22E, Schwartz's Principles of Surgery 11E, Braunwald's Heart Disease, and Fuster & Hurst's The Heart 15E.
Mitral Stenosis
Etiology
Rheumatic fever is the dominant cause, accounting for ~60% of pure MS cases. Chronic inflammation causes commissural fusion, chordal shortening, and calcification, producing the classic "fish-mouth" or funnel-shaped orifice. Other, less common causes include:
- Congenital MS (parachute valve, cor triatriatum)
- Severe mitral annular calcification with leaflet extension
- Systemic lupus erythematosus / rheumatoid arthritis
- Left atrial myxoma
- Infective endocarditis with large vegetations
- Prior chest radiation, mucopolysaccharidosis
MS has declined significantly in high-income countries but remains a major problem in sub-Saharan Africa, India, Southeast Asia, and Oceania.
Pathology
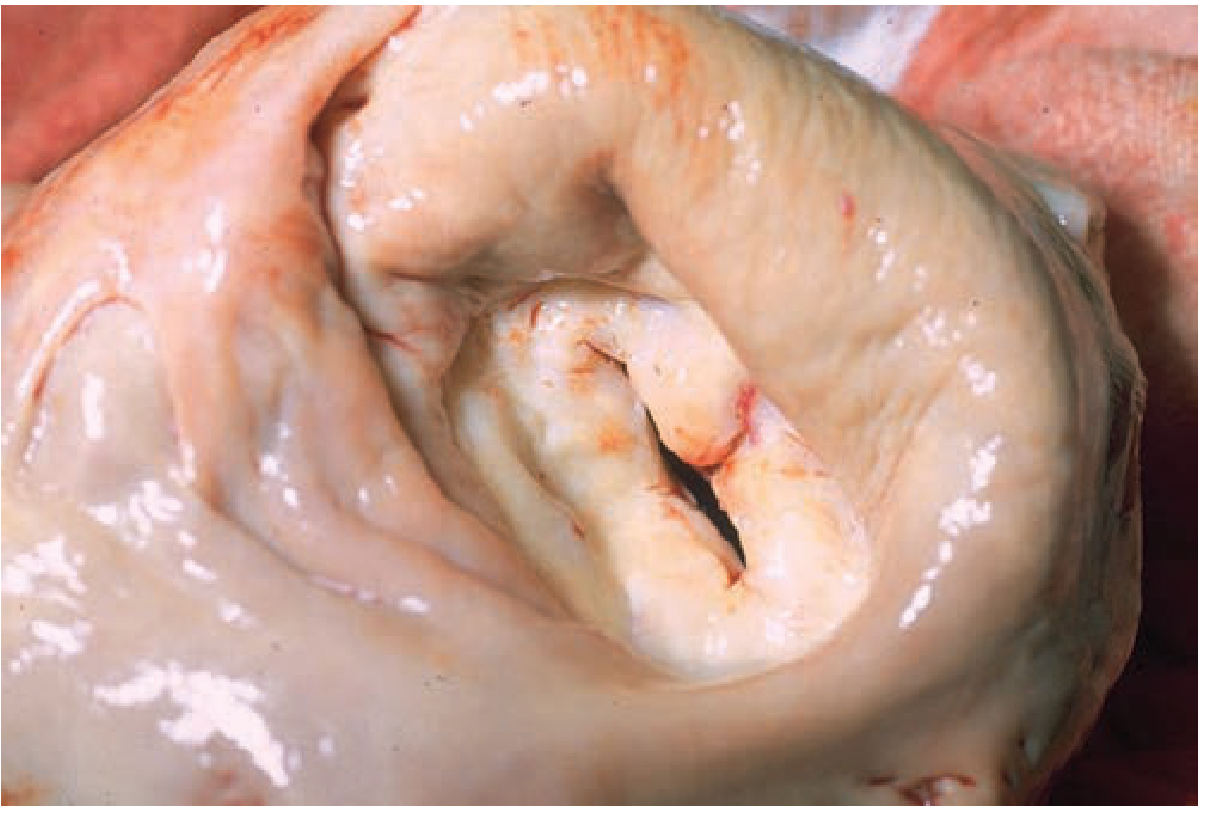
Gross specimen: thickened, fused mitral leaflets with a severely narrowed orifice — classic rheumatic MS (Schwartz's Principles of Surgery)
The rheumatic process causes:
- Diffuse leaflet thickening with fibrous tissue and calcium deposits
- Commissural fusion — the commissures fuse, narrowing the orifice
- Subvalvular involvement — chordae tendineae fuse and shorten
- The valve assumes a funnel shape with doming leaflets
- Later changes may be exacerbated by altered flow and ongoing inflammation
Pathophysiology
| Parameter | Normal | Significant MS | Severe MS |
|---|---|---|---|
| MVA (cm²) | 4–6 | ~2 | ≤1.5 |
| Mean gradient (mmHg) | — | 5–10 | >10 |
| PA systolic pressure (mmHg) | — | 30–50 | >50 |
When MVA falls below ~2 cm², the LA must generate an abnormally elevated pressure gradient to push blood into the LV. At MVA ≤1.5 cm² (severe MS), LA pressure of ~25 mmHg is required to maintain normal cardiac output.
Consequences in sequence:
- Elevated LA pressure → left atrial enlargement
- Pulmonary venous hypertension → dyspnea, orthopnea, pulmonary edema
- Reactive pulmonary arterial hypertension — vasoconstriction + intimal hyperplasia ("second stenosis") — protects against acute pulmonary edema but reduces cardiac output
- RV enlargement → secondary TR, PR, right-sided heart failure
- Atrial fibrillation (AF) — develops due to LA dilation; tachycardia shortens diastolic filling time and dramatically worsens the gradient
- Thromboembolism — LA thrombus (especially LA appendage) → stroke risk
Key hemodynamic point: Tachycardia is particularly dangerous because it shortens diastole proportionately more than systole, reducing filling time and sharply elevating LA pressure.
ACC/AHA Staging
| Stage | Definition | MVA |
|---|---|---|
| A | Risk factors (e.g., rheumatic fever), normal flow velocities | Normal |
| B | Progressive MS, increased velocities | >1.5 cm² |
| C | Severe, asymptomatic | ≤1.5 cm² |
| D | Severe, symptomatic | ≤1.5 cm² |
Symptoms
- Exertional dyspnea — the first and most common symptom, triggered by exercise, pregnancy, fever, or AF with rapid ventricular rate
- Orthopnea and paroxysmal nocturnal dyspnea
- Hemoptysis — from pulmonary venous hypertension
- Palpitations — from AF
- Systemic embolism / stroke
- Right-sided heart failure symptoms (edema, ascites) — in advanced disease
The latent period from rheumatic fever to symptoms is typically 20 years; progressive disability follows.
Physical Examination — The Auscultatory Triad
- Loud S1 — abrupt closure of the thickened but still mobile mitral valve
- Opening snap (OS) — the thickened valve snaps open; a shorter S2–OS interval = more severe stenosis (higher LA pressure)
- Low-pitched mid-diastolic rumble at the apex, best heard in the left lateral decubitus position with the bell; pre-systolic accentuation in sinus rhythm
Note: In elderly patients with heavy calcification, the opening snap and loud S1 may be absent. The murmur may be soft with low stroke volume.
Investigations
ECG:
- P mitrale — broad, notched P wave in lead II, biphasic in V1, indicating LA enlargement (in sinus rhythm)
- With pulmonary hypertension: right axis deviation, RV hypertrophy
- AF is common
Chest X-ray:
- Straightening of the left heart border (LA enlargement)
- Prominent main pulmonary arteries
- Dilated upper lobe pulmonary veins
- Kerley B lines — horizontal lines at the lung bases when resting mean LA pressure >20 mmHg
Echocardiography (gold standard):
- TTE: measures transmitral velocities (E wave, A wave), mean gradient, MVA by pressure half-time or planimetry, pulmonary artery pressure, RV function
- Wilkins score (echo score): assesses leaflet mobility, thickening, calcification, subvalvular involvement — critical for planning PMBC
- TEE: superior imaging; mandatory before PMBC to exclude LA thrombus; especially useful when TTE is suboptimal
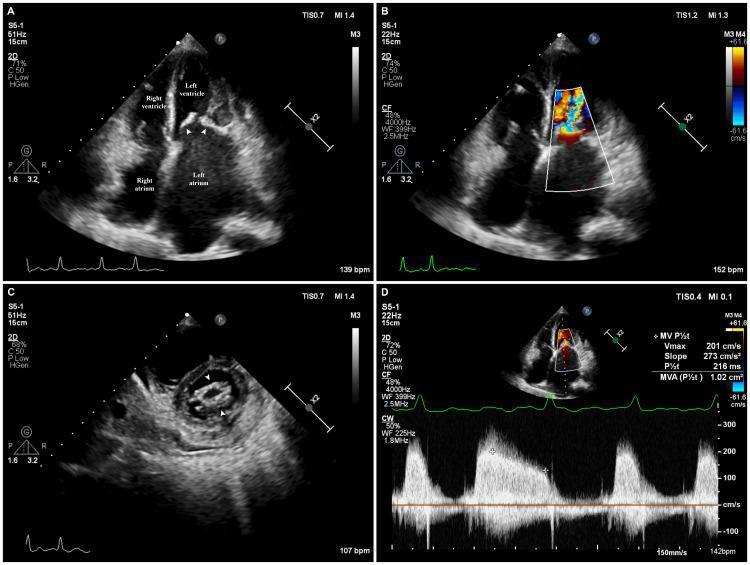
Echocardiographic hallmarks of severe MS: left atrial enlargement, turbulent diastolic inflow on color Doppler, fish-mouth orifice on short axis, and elevated diastolic gradient by CW Doppler
Cardiac catheterization: Reserved when there is discrepancy between clinical findings and noninvasive data.
Medical Management
| Indication | Treatment |
|---|---|
| Pulmonary congestion | Na restriction + oral diuretics |
| Rate control in AF | Beta-blockers, non-DHP CCBs (verapamil/diltiazem), or digoxin |
| Anticoagulation (AF, prior embolism, or LA thrombus) | Warfarin (VKA), target INR 2–3 |
| Anticoagulation in sinus rhythm with very enlarged LA (>5.5 cm) | Controversial; VKA generally used |
| Rheumatic fever prophylaxis | Penicillin (group A β-hemolytic streptococcal prevention) |
⚠️ DOACs are contraindicated in rheumatic MS with AF. A 2022 NEJM trial (ATTMOSPHERE/INVICTUS) confirmed significantly higher mortality with rivaroxaban vs. VKA in rheumatic MS-associated AF. — Harrison's 22E, referencing Connolly SJ et al., NEJM 2022
Cardioversion of AF: Indicated if recent-onset AF in a patient not severe enough for intervention. Requires ≥3 weeks of therapeutic anticoagulation or TEE to exclude LA thrombus first.
Interventional Management
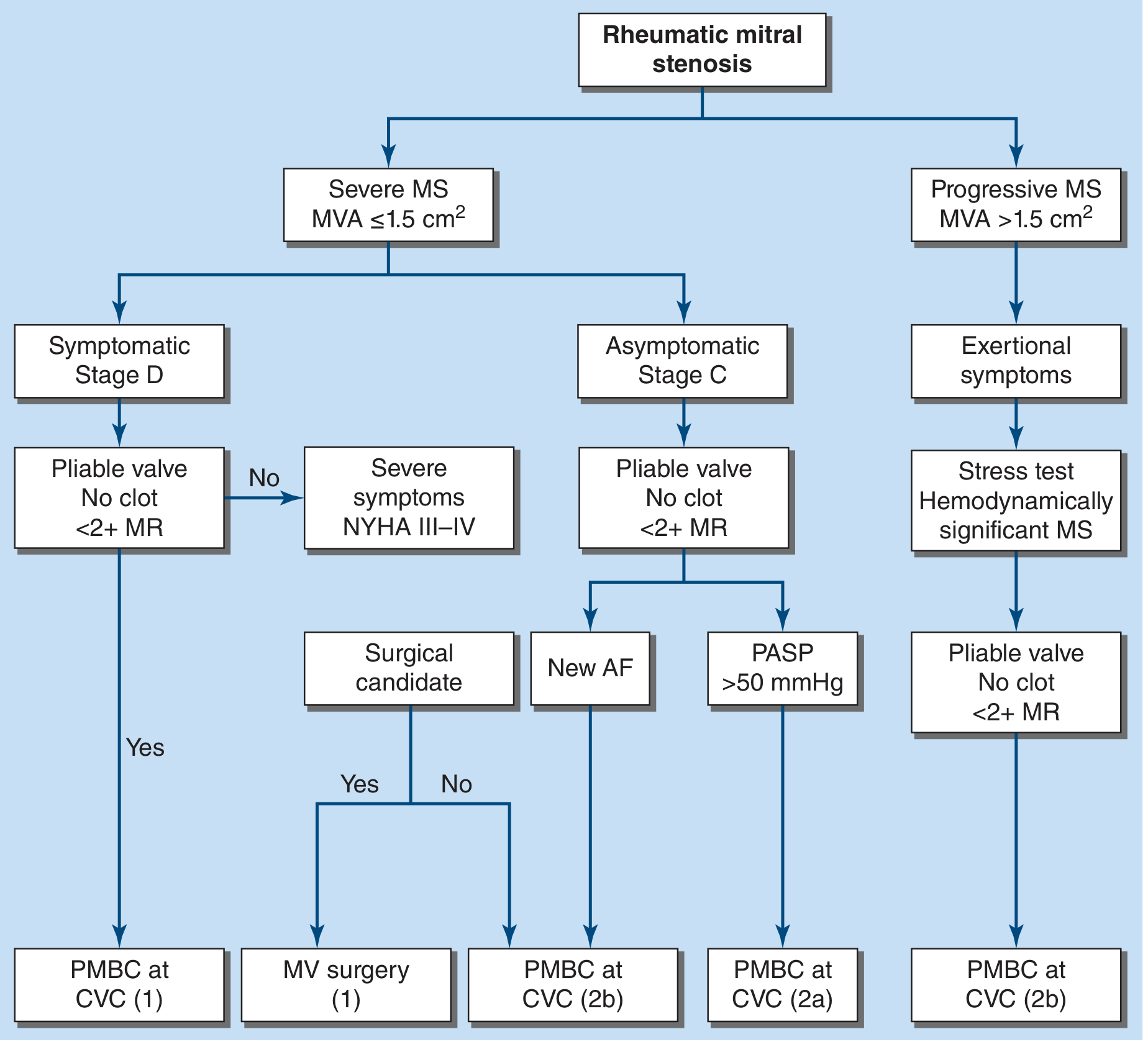
FIGURE 274-2 from Harrison's 22E — ACC/AHA 2021 guideline management algorithm
Percutaneous Mitral Balloon Commissurotomy (PMBC)
Indications (Class I):
- Symptomatic (NYHA II–IV) severe MS (MVA ≤1.5 cm² or <1 cm²/m² BSA), pliable valve, no significant MR (<2+), no LA thrombus
- Asymptomatic severe MS + new AF or PASP >50 mmHg (Class 2a–2b)
Favorable anatomy (Wilkins score ≤8):
- Pliable, non-calcified leaflets with minimal subvalvular involvement
- Absence of significant MR
Contraindications: LA thrombus, significant (≥2+) MR, heavily calcified or immobile valve
Outcomes: Doubles MVA; 5-year event-free survival ~60–70% in well-selected patients
Surgical Options
Open commissurotomy:
- Indicated for suitable anatomy when PMBC is not available or fails
- Operative mortality <1%; freedom from reoperation ~80% at 20 years
- Thromboembolic complications <1%/year
Mitral valve replacement (MVR):
- Indicated when severe calcification/immobility precludes commissurotomy, or when significant MR coexists
- Indication: severe MS (MVA ≤1.5 cm²), NYHA class III–IV despite optimal medical therapy
- Peri-operative mortality typically <5% in young patients; rises to ≥10% in elderly with comorbidities
- 10-year survival in surgical survivors ~70%
- Requires lifelong anticoagulation with mechanical prostheses
Complications
| Complication | Mechanism |
|---|---|
| Atrial fibrillation | LA enlargement, LA myopathy |
| Systemic thromboembolism / stroke | LA thrombus (especially LA appendage) |
| Pulmonary hypertension | Passive + reactive (second stenosis) |
| Right heart failure | Severe PAH → RV dilation, TR |
| Hemoptysis | Pulmonary venous hypertension → bronchial vein rupture |
| Infective endocarditis | Turbulent flow, deformed valve |
| Recurrent rheumatic carditis | Ongoing streptococcal infection |
Special Populations
Elderly: Loud S1 and OS often absent; calcified/immobile valve reduces PMBC success rates (<50%); MVR peri-operative mortality ≥10%.
Pregnancy: Tachycardia + increased blood volume can precipitate acute pulmonary edema in previously stable patients; PMBC can be performed during pregnancy (with radiation shielding).
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 274 — Mitral Stenosis
- Schwartz's Principles of Surgery 11E, Chapter 21 — Acquired Heart Disease
- Braunwald's Heart Disease, Chapters 75 & relevant sections
- ACC/AHA 2021 Guideline for Management of Valvular Heart Disease (Otto CM et al., Circulation 143:e72, 2021)
Recent literature note: A 2024 meta-analysis (PMID 37014563) on direct oral anticoagulants in AF + significant MS confirms that DOACs (rivaroxaban specifically) are associated with worse outcomes compared to VKA — consistent with current guidelines recommending warfarin for rheumatic MS.
This is a shared conversation. Sign in to Orris to start your own chat.