
Make it in flowcahrt
A clean vertical flowchart titled "Mechanism of Breathing" with the following hierarchy and structure: TOP BOX: "Mechanism of Breathing" (dark blue header) Arrow down to: "Study of physical properties of LUNGS, AIRWAYS & CHEST WALL involved in physiology of respiration" Arrow down to: "MUSCLES OF RESPIRATION" (section header, green) Arrow down to: "MUSCLES OF INSPIRATION" (orange box) Two sub-points: "→ Causes expansion of chest" and "→ Elastic recoil makes intrapleural pressure more negative" Arrow down to: "PRIMARY MUSCLES OF INSPIRATION" (yellow box) Split into TWO branches: LEFT BRANCH: "DIAPHRAGM" (blue box) - Main muscle of inspiration - Innervated by Phrenic Nerve (C3-C5) - Contraction → moves down → lung inflation - Paralysis of phrenic N → diaphragm moves UP during inspiration (abnormal) RIGHT BRANCH: "EXT. INTERCOSTAL MUSCLES" (blue box) - Oriented obliquely between ribs (forward & downward) - Contraction has 2 effects: → Bucket Handle Effect → increases TRANSVERSE diameter → Pump Handle Effect → increases AP diameter of thorax All boxes with rounded corners, arrows connecting each level, clean white background, professional medical diagram style
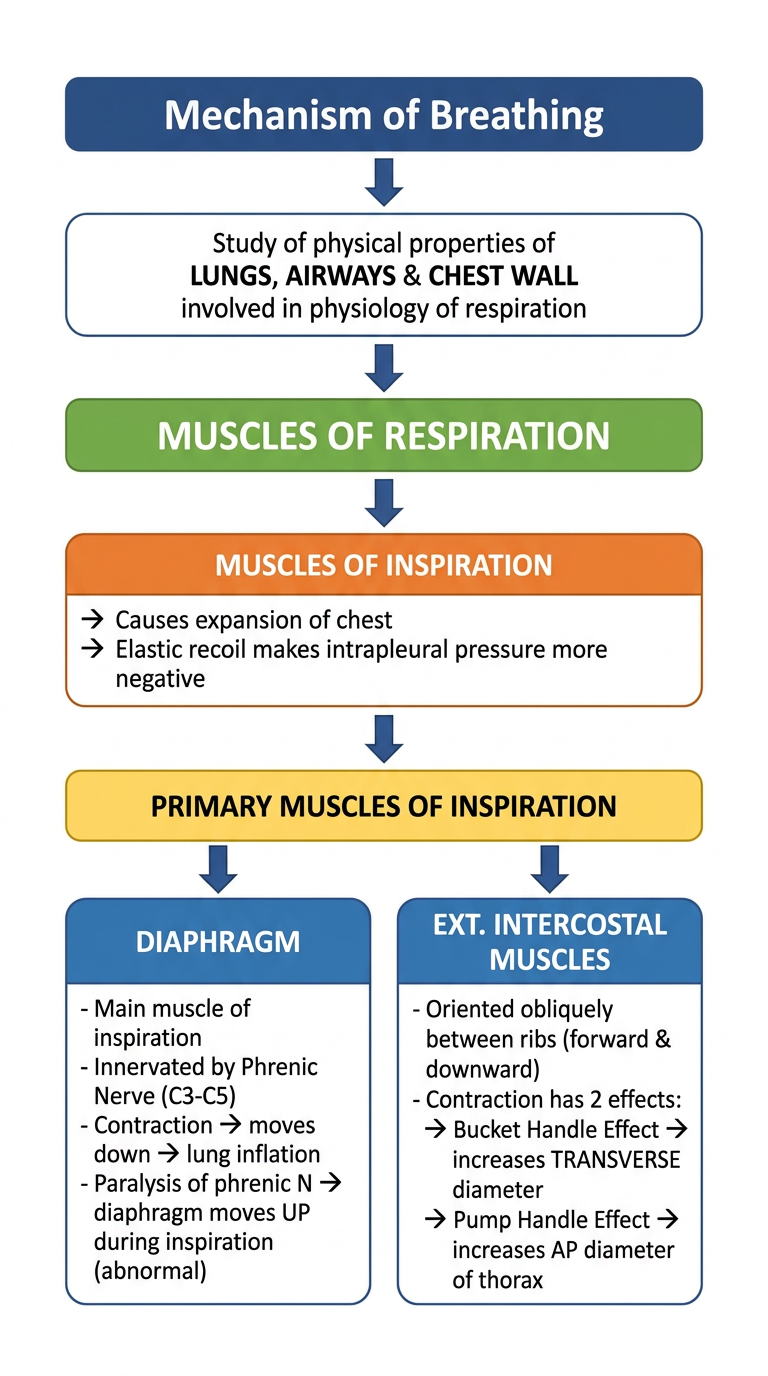
- Mechanism of Breathing - the overarching topic (study of physical properties of lungs, airways & chest wall)
- Muscles of Inspiration - causes chest expansion and makes intrapleural pressure more negative
- Two primary muscles branching out:
- Diaphragm - innervated by phrenic nerve (C3-C5); paralysis causes paradoxical upward movement during inspiration
- Ext. Intercostal Muscles - oblique orientation; contraction increases thoracic diameter via Bucket Handle (transverse) and Pump Handle (AP/vertical) effects
Mechanism of respiration Give answer in flow chart
A detailed medical flowchart titled "Mechanism of Respiration" with two parallel major branches: INSPIRATION and EXPIRATION. Clean white background, professional medical style, rounded boxes, color-coded sections. TITLE BOX (dark blue, top center): "MECHANISM OF RESPIRATION" Arrow down to: "AT REST" (grey box, center) - Alveolar pressure = Atmospheric pressure (0 cm H2O) - Intrapleural pressure = -5 cm H2O - No airflow (no pressure gradient) - Lung volume = FRC (Functional Residual Capacity) Then SPLITS into TWO columns: LEFT COLUMN - INSPIRATION (blue theme): Box 1: "TRIGGER" → Nerve impulse to respiratory muscles Box 2: "DIAPHRAGM CONTRACTS" + "External Intercostal Muscles Contract" → Thoracic cavity volume INCREASES Box 3: "Lung volume INCREASES" → Boyle's Law: P x V = constant Box 4: "Alveolar pressure FALLS" → becomes -1 cm H2O (below atmospheric) → Intrapleural pressure → -8 cm H2O Box 5: "Pressure gradient: Atmosphere > Alveoli" → AIR FLOWS INTO LUNGS Box 6: "End of Inspiration" → Alveolar pressure returns to 0 → Tidal Volume = ~0.5 L inspired → Lung volume = FRC + VT RIGHT COLUMN - EXPIRATION (orange/red theme): Box 1: "TRIGGER" → Diaphragm & intercostal muscles RELAX Box 2: "Elastic recoil of lungs" → Thoracic cavity volume DECREASES Box 3: "Lung volume DECREASES" → Boyle's Law: P x V = constant Box 4: "Alveolar pressure RISES" → becomes +1 cm H2O (above atmospheric) → PASSIVE process (no muscle contraction needed) Box 5: "Pressure gradient: Alveoli > Atmosphere" → AIR FLOWS OUT OF LUNGS Box 6: "End of Expiration" → Alveolar pressure returns to 0 → Tidal Volume = ~0.5 L expired → Lung volume returns to FRC BOTTOM BOX (green, center): "Cycle Repeats → Normal Breathing Rate: 12-20 breaths/min" Note at bottom: "Forced Expiration: uses expiratory muscles (abdominal + internal intercostals) → alveolar pressure becomes strongly positive" All boxes connected with clear arrows, well-spaced layout
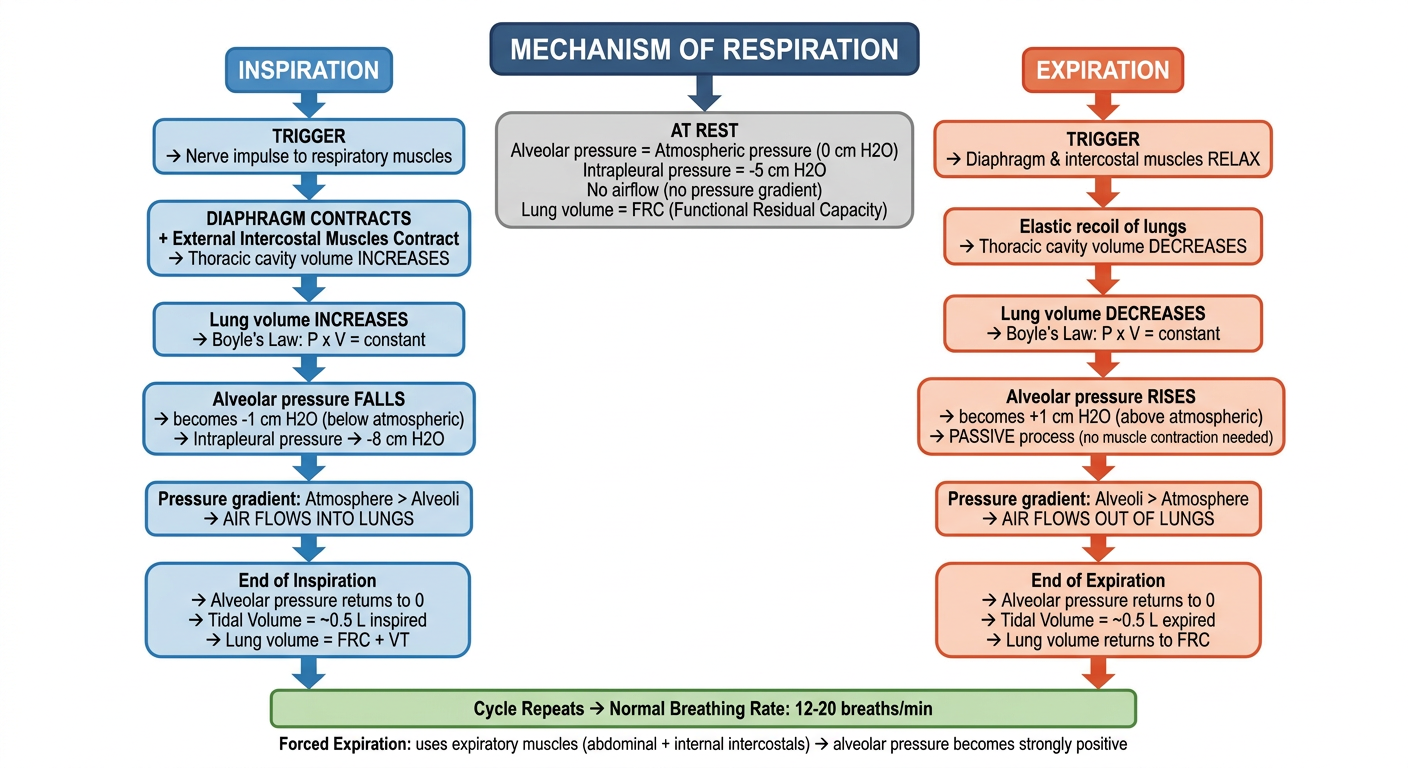
- Alveolar pressure = 0 (equal to atmospheric)
- Intrapleural pressure = -5 cm H2O
- Lung volume = FRC, no airflow
- Diaphragm + external intercostals contract
- Thoracic volume increases
- Lung volume increases → Alveolar pressure falls to -1 cm H2O (Boyle's Law)
- Pressure gradient: Atmosphere > Alveoli → air flows IN
- End of inspiration: alveolar pressure = 0, tidal volume (~0.5 L) entered
- Intrapleural pressure reaches -8 cm H2O
- Diaphragm + intercostals relax
- Elastic recoil of lungs → thoracic volume decreases
- Lung volume decreases → Alveolar pressure rises to +1 cm H2O
- Pressure gradient: Alveoli > Atmosphere → air flows OUT
- End of expiration: lung volume returns to FRC
Explain
🫁 Mechanism of Respiration
1. AT REST (Between Breaths)
| Parameter | Value |
|---|---|
| Alveolar pressure | 0 cm H2O (= atmospheric) |
| Intrapleural pressure | -5 cm H2O |
| Airflow | None |
| Lung volume | FRC (Functional Residual Capacity) |
- The lungs are held in a partially inflated state because two opposing forces balance each other:
- Lungs want to collapse inward (elastic recoil)
- Chest wall wants to spring outward
- This tug-of-war creates the negative intrapleural pressure (-5 cm H2O)
2. INSPIRATION (Active Process)
- The diaphragm contracts and moves downward (main driver - responsible for ~75% of inspiration at rest)
- External intercostal muscles contract, lifting the ribs upward and outward
- Both movements expand the chest cavity in all dimensions:
- Diaphragm descends → increases vertical diameter
- Ribs rise → increases AP and transverse diameter (pump handle + bucket handle effects)
- Since the lungs are attached to the chest wall via the pleura, they expand along with the chest
- Intrapleural pressure drops further to -8 cm H2O
- Increased lung volume → alveolar pressure drops to -1 cm H2O (below atmospheric)
- Atmosphere (0) > Alveoli (-1) → pressure gradient drives air INTO the lungs
- Air continues to flow in until alveolar pressure returns to 0
3. EXPIRATION (Passive Process - at rest)
- Diaphragm and external intercostals simply stop contracting
- No active muscle work needed during quiet breathing
- The stretched lungs naturally recoil back to their resting size (like a stretched rubber band)
- This compresses the air inside the alveoli
- Smaller lung volume → alveolar pressure rises to +1 cm H2O (above atmospheric)
- Alveoli (+1) > Atmosphere (0) → air is pushed OUT of the lungs
- Flow stops when alveolar pressure returns to 0
4. FORCED EXPIRATION (Active Process)
- Abdominal muscles and internal intercostal muscles actively contract
- This compresses the chest and drives alveolar pressure to very high positive values (e.g., +35 cm H2O)
- Expiration is rapid and forceful
Clinical relevance: In emphysema/COPD, loss of elastic tissue means alveolar pressure cannot build up enough. During forced expiration, intrapleural pressure can exceed airway pressure, causing dynamic airway collapse - this is why COPD patients have difficulty breathing out.
5. KEY PRESSURE SUMMARY TABLE
| Phase | Alveolar Pressure | Intrapleural Pressure | Airflow |
|---|---|---|---|
| Rest | 0 cm H2O | -5 cm H2O | None |
| Mid-Inspiration | -1 cm H2O | -6 to -8 cm H2O | Inward |
| End-Inspiration | 0 cm H2O | -8 cm H2O | Stops |
| Mid-Expiration | +1 cm H2O | -5 to -6 cm H2O | Outward |
| End-Expiration | 0 cm H2O | -5 cm H2O | Stops |
6. GOLDEN RULES TO REMEMBER
- Inspiration is always active (needs muscle work)
- Quiet expiration is always passive (elastic recoil only)
- Forced expiration is active (needs expiratory muscles)
- Air always flows from high pressure to low pressure
- The driving force is the pressure gradient, not the volume change itself