Here is the complete, exam-focused answer for your MUHS 2nd MBBS Pathology preparation, covering all the starred topics from your question paper pattern. References are drawn from Goldman-Cecil Medicine, Harrison's Principles of Internal Medicine, and Frameworks for Internal Medicine.
ANAEMIA - Complete MUHS Exam Notes (2nd MBBS Pathology)
1. ANAEMIA - Definition and Classification
Definition (★★)
Anaemia is defined as a reduction in haemoglobin concentration, haematocrit, or red blood cell (RBC) count below the normal range for age and sex, resulting in decreased oxygen-carrying capacity of the blood.
Normal values (remember for exams):
- Hb: Males >13 g/dL, Females >12 g/dL, Children >11 g/dL
- PCV/Haematocrit: Males 42-50%, Females 36-45%
- RBC count: Males 4.5-5.5 million/µL
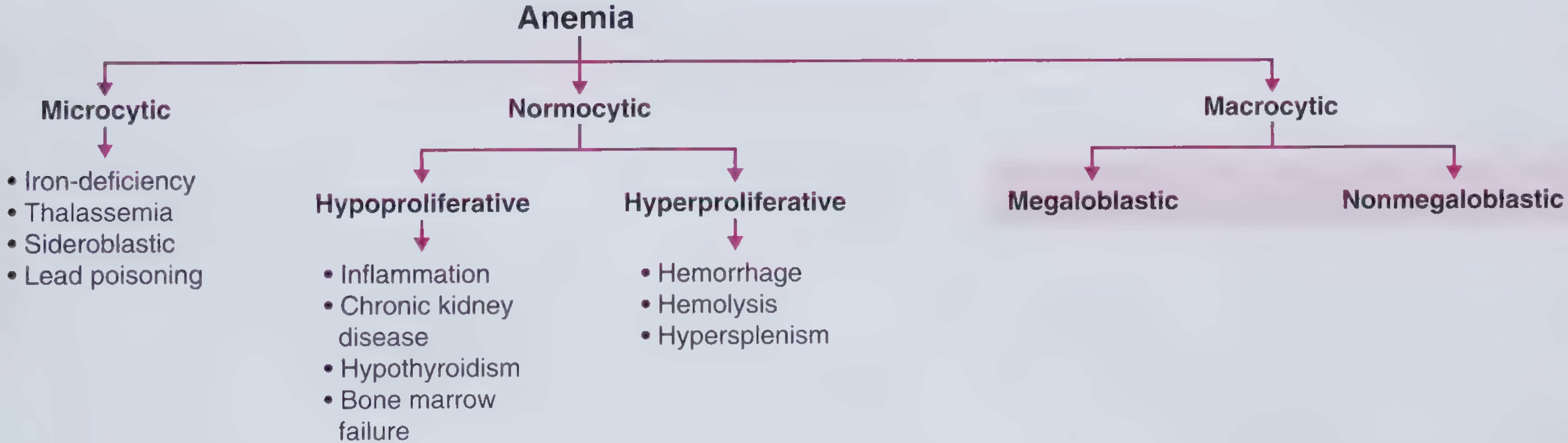
Morphological Classification of Anaemia (★★★★★★ - Most Important)
Based on MCV (Mean Corpuscular Volume) and MCH (Mean Corpuscular Haemoglobin):
| Type | MCV | MCH | Examples |
|---|
| Microcytic Hypochromic | <80 fL | <27 pg | Iron deficiency anaemia, Thalassaemia, Sideroblastic anaemia, Anaemia of chronic disease (late), Lead poisoning |
| Normocytic Normochromic | 80-100 fL | 27-32 pg | Haemolytic anaemia, Aplastic anaemia, Acute blood loss, Anaemia of chronic disease (early), Renal failure |
| Macrocytic (Megaloblastic) | >100 fL | Variable | Vitamin B12 deficiency, Folate deficiency, Drugs (methotrexate, hydroxyurea) |
| Macrocytic (Non-megaloblastic) | >100 fL | Variable | Liver disease, Alcoholism, Hypothyroidism, Reticulocytosis |
Pathophysiological Classification (also important):
- Hypoproliferative: Iron deficiency, Anaemia of chronic disease, Bone marrow failure (aplastic anaemia), Renal failure
- Hyperproliferative (Haemolytic): Haemolytic anaemias (inherited/acquired)
- Maturation defect: Megaloblastic anaemia (nuclear maturation defect), Thalassaemia (cytoplasmic defect)
2. MEGALOBLASTIC ANAEMIA (★★★★★★)
Definition
Megaloblastic anaemia is defined as anaemia or pancytopenia resulting from failure of DNA synthesis, causing an imbalance of maturation between the nucleus and the cellular cytoplasm. This results in large cells that are subject to maturation arrest and early destruction (ineffective erythropoiesis). (Goldman-Cecil Medicine)
The Megaloblast - What Is It?
A megaloblast is an abnormally large erythroid precursor with:
- Large cell size (3-4x normal normoblast)
- Open, lacy (fenestrated) chromatin - nucleus looks immature/"young-looking"
- Abundant, well-haemoglobinised cytoplasm - cytoplasm matures normally
- This creates the hallmark: nuclear-cytoplasmic dissociation (cytoplasm mature, nucleus immature)
Megaloblasts arise at all stages: promegaloblast → megaloblast → intermediate megaloblast → late megaloblast (instead of normal pronormoblast → basophilic → polychromatic → orthochromatic normoblast)
Causes of Megaloblastic Anaemia
A. Vitamin B12 (Cobalamin) Deficiency:
- Pernicious anaemia (autoimmune - anti-parietal cell antibodies, anti-intrinsic factor antibodies) - commonest cause
- Gastrectomy / gastric bypass (loss of parietal cells → ↓ intrinsic factor)
- Dietary deficiency (strict vegans/vegetarians)
- Ileal disease / resection (Crohn's disease, TB of terminal ileum)
- Fish tapeworm (Diphyllobothrium latum)
- Bacterial overgrowth (blind loop syndrome)
- Drugs: metformin, proton pump inhibitors, nitrous oxide
B. Folic Acid Deficiency:
- Poor dietary intake (alcoholics, elderly, poor diet lacking green leafy vegetables)
- Increased demand: pregnancy, haemolytic anaemia, rapid cell proliferation
- Malabsorption: coeliac disease, Crohn's disease, tropical sprue
- Drugs: methotrexate, trimethoprim, phenytoin, carbamazepine, sulfasalazine
C. Others (Not B12/Folate):
- Chemotherapy drugs: hydroxyurea, azathioprine, 5-FU
- Antiretrovirals: zidovudine
- Hereditary orotic aciduria, Lesch-Nyhan syndrome
Pathogenesis (Mechanism)
B12 Deficiency
↓
Methionine synthase blocked
↓
Methyl-THF cannot → THF (METHYLFOLATE TRAP)
↓
↓ 5,10-methylene THF
↓
Thymidylate synthase cannot convert dUMP → dTMP
↓
↓ Thymidine → Uracil misincorporated into DNA
↓
DNA synthesis impaired → MATURATION ARREST
↓
MEGALOBLASTIC CHANGE (all rapidly dividing cells affected)
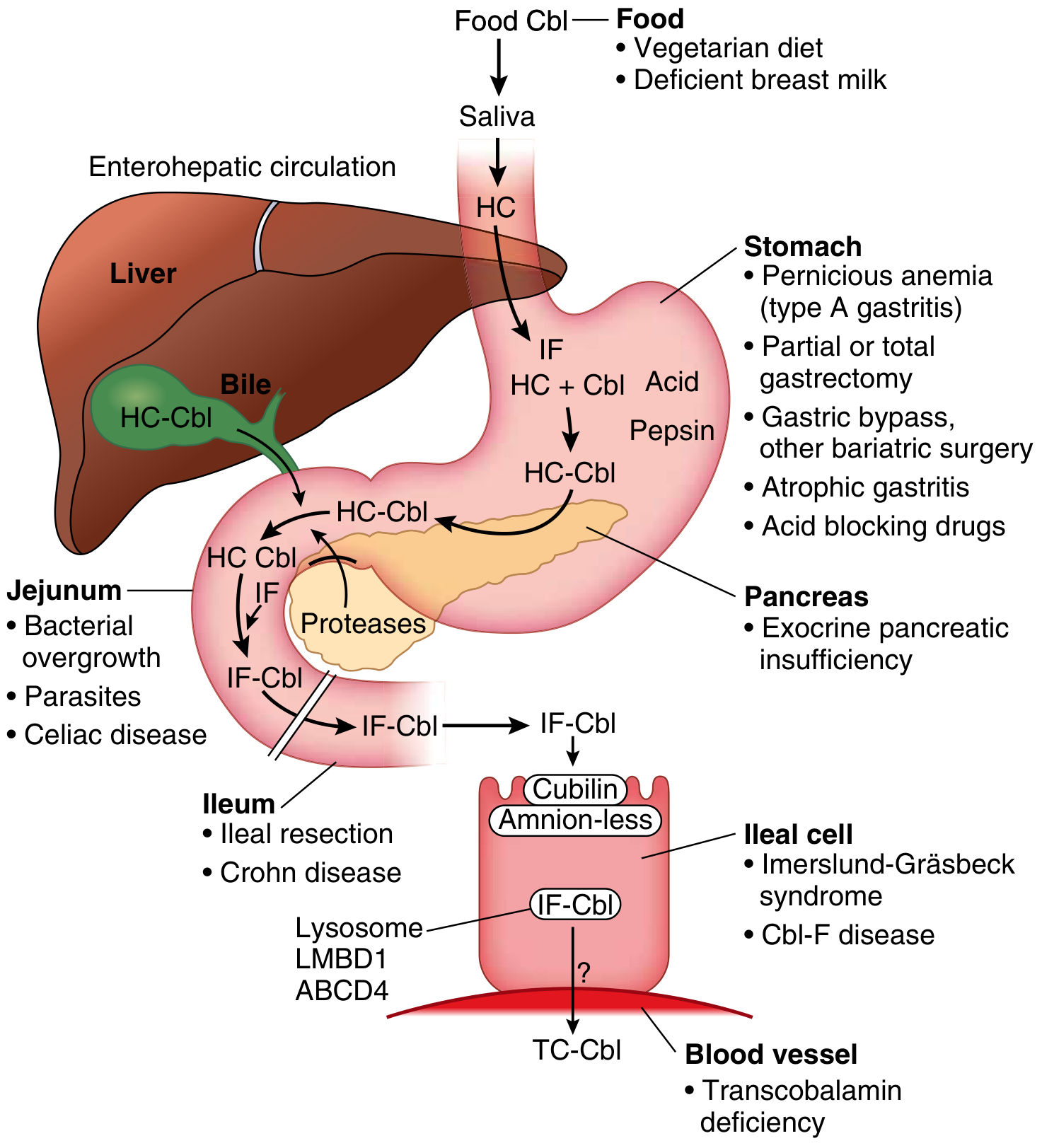
Key concept: B12 deficiency causes secondary folate deficiency via the "methylfolate trap." Both B12 and folate deficiency produce identical haematological changes - only B12 deficiency causes neurological damage (subacute combined degeneration of the cord).
The cobalamin-B12 absorption diagram (Goldman-Cecil):
Laboratory Investigations - Megaloblastic Anaemia (★★★★)
A. Complete Blood Count (CBC):
- Hb: decreased (may be severely low, <7 g/dL)
- MCV: markedly elevated (often >115 fL, may reach 130-140 fL)
- MCH: elevated (but MCHC normal - normochromic)
- WBC: decreased (leucopenia) - due to ineffective granulopoiesis
- Platelets: decreased (thrombocytopenia)
- Pancytopenia in severe cases (anaemia + leucopenia + thrombocytopenia)
- Reticulocyte count: decreased (reticulocytopenia - key differentiator from haemolytic anaemia)
- RDW: elevated (anisocytosis)
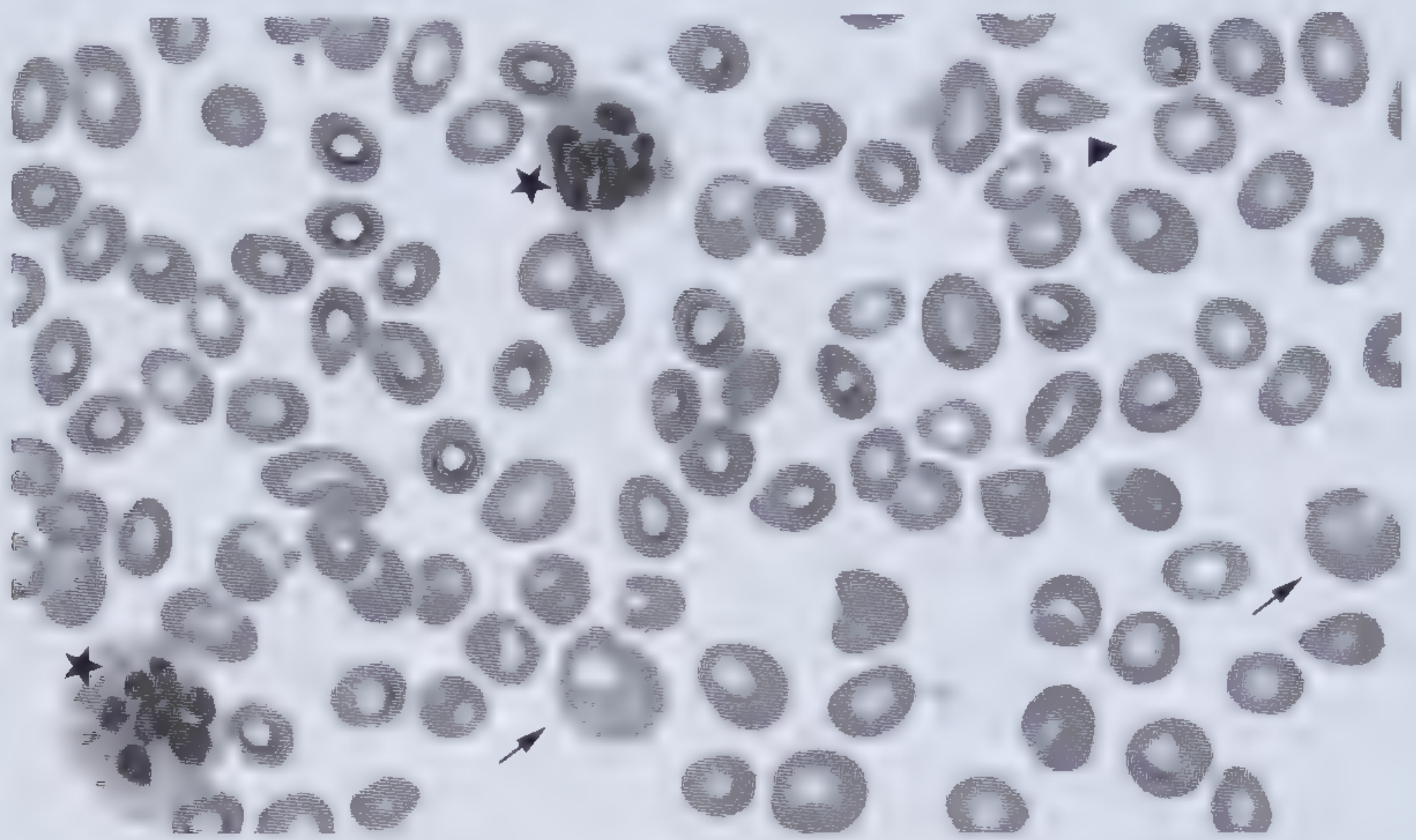
B. Peripheral Blood Smear (PBS) Findings (★★★):
Fig: PBS in megaloblastic anaemia - arrows = macro-ovalocytes; stars = hypersegmented neutrophil (6-lobed); arrowhead = teardrop RBC
| Finding | Details |
|---|
| Macro-ovalocytes | Large oval RBCs (MCV >115 fL); pathognomonic |
| Hypersegmented neutrophils | ≥5% neutrophils with ≥5 lobes, or any neutrophil with ≥6 lobes - EARLIEST and most sensitive sign |
| Anisocytosis | Variation in RBC size |
| Poikilocytosis | Teardrop cells (dacrocytes), fragmented cells |
| Basophilic stippling | Occasionally seen |
| Howell-Jolly bodies | Nuclear remnants in RBCs |
| Hypersegmented monocytes | Less commonly noted |
Exam tip: Hypersegmented neutrophils (5-lobed or 6-lobed) are the earliest peripheral smear finding. Macro-ovalocytes are the most characteristic RBC finding.
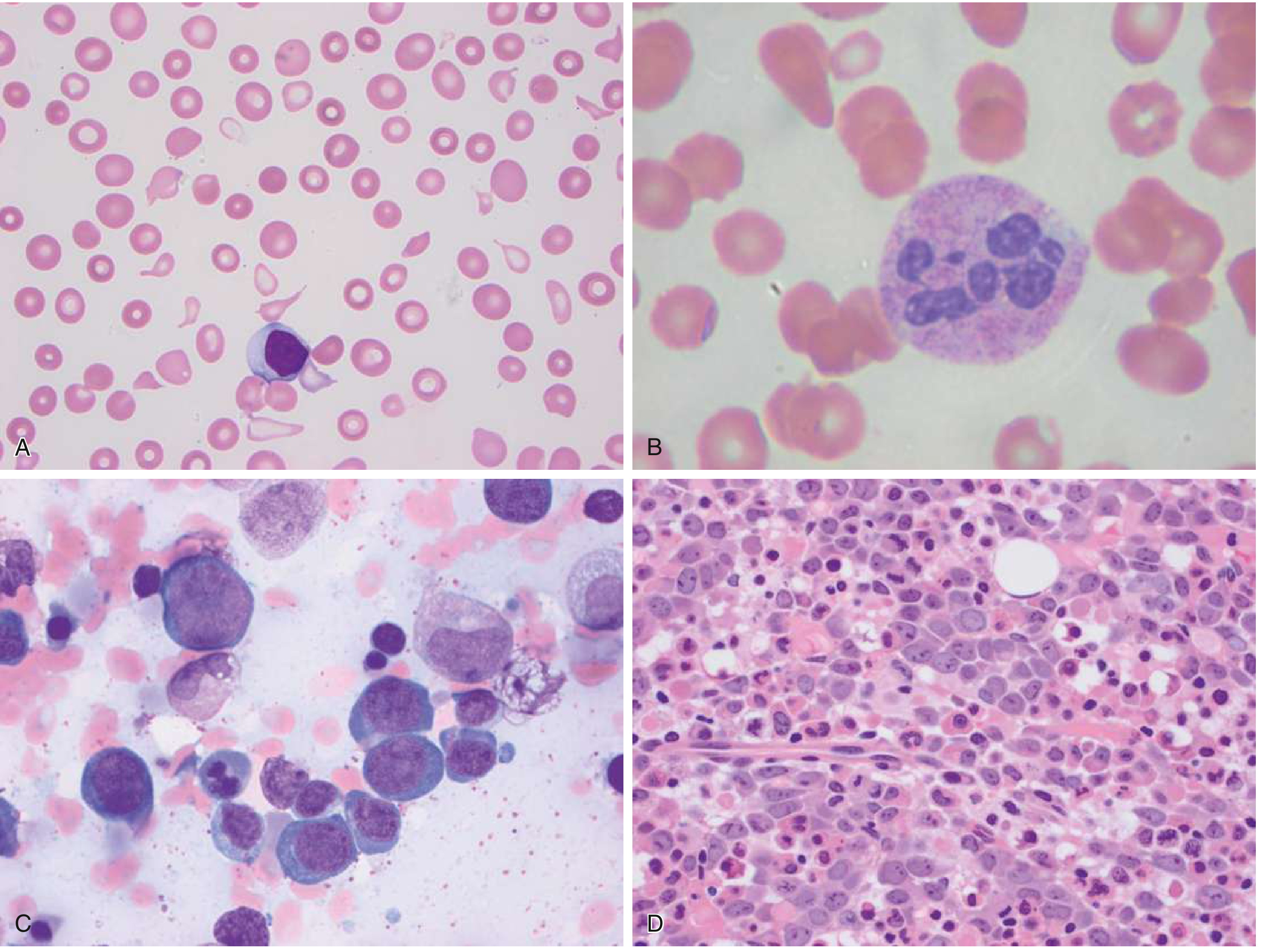
C. Bone Marrow Aspirate/Biopsy Findings (★★):
Fig: A = PBS with oval macrocytes and teardrop cells; B = Hypersegmented neutrophil (6 lobes); C = Bone marrow aspirate: megaloblastic erythroid precursors with open lacy chromatin; D = Bone marrow biopsy: hypercellular with erythroid hyperplasia (can mimic acute leukaemia)
| Finding | Details |
|---|
| Hypercellular marrow | Erythroid hyperplasia with ↓ M:E ratio |
| Megaloblasts | Large erythroblasts with open/lacy chromatin but mature (haemoglobinised) cytoplasm - nuclear-cytoplasmic dissociation |
| Giant metamyelocytes and band forms | Giant, horseshoe-shaped metamyelocytes - pathognomonic of megaloblastic marrow |
| Ineffective erythropoiesis | Apoptosis of megaloblasts within the marrow → intramedullary haemolysis |
| Erythroid dysplasia | Nuclear fragments, binucleation |
EXAM WARNING: Megaloblastic marrow can be mistaken for acute leukaemia by inexperienced examiners due to large cells with open chromatin. KEY differentiator: MCV is very high and clinical history + serum B12/folate levels resolve the diagnosis.
D. Biochemical Tests:
- Serum B12: decreased (<200 pg/mL)
- Serum folate: decreased (in folate deficiency)
- RBC folate: more reliable than serum folate
- Serum LDH: markedly elevated (due to intramedullary haemolysis)
- Indirect bilirubin: elevated (haemolysis)
- Serum haptoglobin: decreased
- Serum methylmalonic acid (MMA): elevated in B12 deficiency (most sensitive and specific)
- Serum homocysteine: elevated in both B12 AND folate deficiency
- Serum iron: elevated (ineffective erythropoiesis → iron not used → released back)
- Gastric analysis: achlorhydria in pernicious anaemia
- Anti-intrinsic factor antibodies: diagnostic of pernicious anaemia
- Anti-parietal cell antibodies: less specific (positive in 85-90%)
- Schilling test: historically used to diagnose pernicious anaemia
3. SICKLE CELL ANAEMIA (★)
Etiopathogenesis
Genetics:
- Autosomal recessive disorder
- Point mutation in beta-globin gene on chromosome 11
- GAG → GTG codon change
- Glutamic acid (position 6) → Valine (hydrophilic → hydrophobic substitution)
- Results in formation of Haemoglobin S (HbS) instead of HbA
- Homozygous (HbSS) = Sickle cell disease (severe)
- Heterozygous (HbAS) = Sickle cell trait (carrier, usually asymptomatic)
Mechanism of Sickling:
Deoxygenation (hypoxia, acidosis, cold, dehydration)
↓
HbS polymerises → forms long, rigid "tactoid" fibers/crystals
↓
RBC distorts → sickle/crescent shape
↓
Two consequences:
[1] HAEMOLYSIS: Sickled cells are rigid, osmotically fragile
→ trapped in spleen and microvessels → destroyed
→ CHRONIC HAEMOLYTIC ANAEMIA (Hb 6-8 g/dL)
[2] VASO-OCCLUSION: Sickled cells occlude microcirculation
→ ischaemia and infarction of organs
→ PAINFUL CRISES (bone, chest, abdomen, CNS)
Factors promoting sickling:
- Hypoxia (low O2 tension)
- Acidosis
- Dehydration (↑ MCHC)
- Cold/hypothermia
- Infection
- High concentration of HbS in cell
- Absence of HbF (HbF inhibits polymerisation - explains why disease manifests after 6 months when HbF falls)
Protective factors: High HbF concentration (hence neonates are protected; HU induces HbF production)
Pathological Changes in Organs:
- Spleen: Early - splenomegaly (congestion); Later - autosplenectomy (repeated infarctions → fibrosis/shrinkage → small, fibrotic spleen)
- Bone marrow: Erythroid hyperplasia → may expand medulla → "hair-on-end" appearance on X-ray
- Bones: Avascular necrosis (femoral/humeral head), Salmonella osteomyelitis
- Liver: Hepatomegaly, hepatic sequestration
- Kidney: Renal papillary necrosis, haematuria
- CNS: Stroke (children)
- Lung: Acute chest syndrome
- Skin: Leg ulcers (chronic)
Laboratory Investigations:
A. CBC:
- Hb: 6-8 g/dL (chronic haemolytic anaemia)
- Normocytic normochromic anaemia (MCV normal)
- Reticulocytosis: 10-25% (compensatory)
- WBC: elevated (leukocytosis)
- Platelets: elevated (thrombocytosis)
B. Peripheral Blood Smear (PBS):
| Finding | Significance |
|---|
| Sickle cells (drepanocytes) | Elongated, crescent-shaped cells; pathognomonic |
| Target cells (codocytes) | Thin RBCs with central density; thin cytoplasm |
| Polychromasia | Reticulocytes (increased red cell production) |
| Howell-Jolly bodies | Due to functional hyposplenism |
| Nucleated RBCs | Indicate marked erythroid stress |
| Anisocytosis, poikilocytosis | General finding |
C. Haemoglobin Electrophoresis:
- HbSS: HbS 85-95%, HbF 5-15%, NO HbA - DIAGNOSTIC
- HbAS (trait): HbA ~60%, HbS ~40%
- Cellulose acetate pH 8.4 or citrate agar pH 6.0
D. Other Tests:
- Sickling test: RBCs sickle when exposed to reducing agent (sodium metabisulphite) - screening test
- LDH: elevated
- Bilirubin (indirect): elevated
- Haptoglobin: decreased
- Serum iron: elevated
- Blood film: as above
E. Solubility Test (Sickledex): HbS is insoluble in deoxygenated buffer = turbid solution (screening)
4. IRON DEFICIENCY ANAEMIA (IDA) - Laboratory Diagnosis (★★★★)
Stages of Iron Deficiency:
| Stage | Iron Stores | Serum Ferritin | Serum Iron | Transferrin/TIBC | Transferrin Saturation | Hb | MCV |
|---|
| Stage 1: Iron depletion | Absent | ↓ (<30 µg/L) | Normal | ↑ | Normal | Normal | Normal |
| Stage 2: Iron-restricted erythropoiesis | Absent | ↓↓ | ↓ | ↑↑ | ↓ (<15%) | Normal/borderline | Normal |
| Stage 3: IDA | Absent | ↓↓ | ↓↓ | ↑↑↑ | ↓↓ (<15%) | ↓ | ↓ (<80 fL) |
Laboratory Diagnosis (★★★★)
A. CBC:
- Hb: decreased
- MCV: decreased (<80 fL) - microcytic
- MCH: decreased (<27 pg) - hypochromic
- MCHC: decreased (<32 g/dL)
- RDW: elevated (>14%) - anisocytosis (early finding, even before MCV falls)
- Platelet count: often elevated (thrombocytosis - reactive)
- Reticulocyte count: low/normal (hypoproliferative)
B. PBS Findings:
| Finding | Description |
|---|
| Microcytes | Small RBCs, MCV <80 fL |
| Hypochromia | Pale cells, central pallor >1/3 diameter |
| Pencil cells (cigar cells) | Elongated, thin RBCs - characteristic of IDA |
| Target cells | Occasionally |
| Anisocytosis, poikilocytosis | General |
C. Iron Studies (Most Important Tests):
| Test | IDA | Normal | Anaemia of Chronic Disease |
|---|
| Serum Ferritin | ↓ <30 µg/L | 12-300 µg/L | Normal/↑ |
| Serum Iron | ↓ | 60-170 µg/dL | ↓ |
| TIBC (Transferrin) | ↑ | 250-370 µg/dL | ↓/Normal |
| Transferrin Saturation | ↓ <15% | 20-50% | <15% |
| Serum hepcidin | ↓ | Variable | ↑ |
| sTfR (soluble transferrin receptor) | ↑ | - | Normal |
Exam key: Ferritin <30 µg/L has 92% sensitivity and 98% specificity for IDA. It is the single best non-invasive test for iron stores.
D. Bone Marrow (Gold Standard - rarely done):
- Absent stainable iron (Perl's Prussian blue stain negative)
- Erythroid hyperplasia
- Small, irregular erythroblasts
E. Other:
- Reticulocyte haemoglobin content (CHr): low
- % Hypochromic red cells: elevated
5. HAEMOLYTIC ANAEMIA - Laboratory Investigations (★)
Haemolytic anaemia results from premature destruction of RBCs (normal RBC life span 120 days is shortened).
Classified as:
- Intravascular haemolysis: RBCs destroyed within blood vessels (e.g., ABO incompatibility, PNH, G6PD deficiency)
- Extravascular haemolysis: RBCs destroyed by macrophages in spleen/liver (e.g., hereditary spherocytosis, autoimmune haemolytic anaemia)
Laboratory Investigations:
A. Evidence of Increased Erythropoiesis (Compensatory):
| Test | Finding |
|---|
| Reticulocyte count | ↑↑ (5-20% or more) - most important marker |
| PBS | Polychromasia (blue-staining reticulocytes) |
| Bone marrow | Erythroid hyperplasia ↓ M:E ratio |
| Hb | Decreased |
| MCV | Normal or ↑ (due to reticulocytosis) |
B. Evidence of Increased RBC Destruction:
| Test | Finding | Significance |
|---|
| Serum LDH | ↑↑↑ (especially LDH1 and LDH2) | Released from lysed RBCs |
| Indirect (unconjugated) bilirubin | ↑ | Haem catabolism |
| Serum haptoglobin | ↓↓ (may be undetectable) | Binds free Hb → cleared by liver |
| Urinary urobilinogen | ↑↑ | Excess bilirubin excreted as urobilinogen |
| Urine haemosiderin | +ve in intravascular | Iron from Hb absorbed by renal tubules |
| Plasma/serum Hb | ↑ in intravascular | Free Hb in plasma (haemoglobinaemia) |
| Haemoglobinuria | In intravascular | Red/brown urine |
| Plasma methemalbumin | +ve in intravascular | Haem bound to albumin |
C. PBS Findings (Depend on Type):
| Cell | Diagnosis Suggested |
|---|
| Spherocytes | Hereditary spherocytosis, AIHA |
| Sickle cells | Sickle cell anaemia |
| Schistocytes/helmet cells | Microangiopathic haemolytic anaemia (TTP, HUS, DIC) |
| Target cells | Thalassaemia, HbC disease |
| Elliptocytes | Hereditary elliptocytosis |
| Bite cells/blister cells | G6PD deficiency |
| Acanthocytes | Liver disease, abetalipoproteinaemia |
D. Specific Tests:
| Test | Purpose |
|---|
| Direct Coombs test (DAT) | Detects antibodies/complement on RBCs → +ve in AIHA |
| Indirect Coombs test (IAT) | Detects free antibodies in serum |
| Osmotic fragility test | ↑ in hereditary spherocytosis |
| Ham's test (Acidified serum) | +ve in PNH |
| G6PD assay | G6PD deficiency |
| Haemoglobin electrophoresis | Sickle cell, thalassaemia |
| Flow cytometry (CD55/CD59) | PNH |
6. MACROCYTIC ANAEMIA - Causes in Detail (★★)
Macrocytic anaemia = MCV >100 fL. Divided into MEGALOBLASTIC and NON-MEGALOBLASTIC.
A. Megaloblastic Causes (impaired DNA synthesis):
1. Vitamin B12 (Cobalamin) Deficiency:
- Pernicious anaemia (autoimmune - most common in adults)
- Dietary deficiency (strict veganism)
- Post-gastrectomy (loss of intrinsic factor)
- Ileal disease (TB, Crohn's, resection, radiation)
- Bacterial overgrowth / Blind loop syndrome
- Fish tapeworm (D. latum)
- Drugs: metformin, PPI, H2 blockers, nitrous oxide
- Transcobalamin II deficiency (rare)
2. Folic Acid Deficiency:
- Dietary insufficiency (alcoholics, elderly, poor dietary habits - green leafy vegetables lacking)
- Increased requirements: pregnancy (neural tube defects if deficient!), haemolytic anaemia, rapid cell turnover
- Malabsorption: coeliac disease, tropical sprue, Crohn's disease
- Antifolate drugs: methotrexate, trimethoprim, pyrimethamine, phenytoin, carbamazepine, sulfasalazine
- Renal dialysis (folate lost)
- Alcohol (interferes with absorption and increases excretion)
3. Drugs Directly Inhibiting DNA Synthesis:
- Hydroxyurea (ribonucleotide reductase inhibitor)
- Azathioprine, 6-mercaptopurine
- 5-fluorouracil
- Zidovudine and other antiretrovirals
- Cytosine arabinoside (Ara-C)
4. Rare Inherited Disorders:
- Hereditary orotic aciduria
- Lesch-Nyhan syndrome
- Thiamine-responsive megaloblastic anaemia (Rogers syndrome)
B. Non-Megaloblastic Causes (NO impaired DNA synthesis - round macrocytes):
| Cause | Mechanism |
|---|
| Liver disease / Alcoholism | Most common cause; lipid deposition on RBC membrane → ↑ surface area → round macrocytes; alcohol also directly toxic to marrow |
| Hypothyroidism | Slowed erythropoiesis; may also have B12 deficiency (associated autoimmune) |
| Reticulocytosis | Reticulocytes are larger than mature RBCs; any condition causing marked reticulocytosis (e.g., haemolysis, haemorrhage) raises MCV |
| Aplastic anaemia | Stress erythropoiesis → larger cells |
| Myelodysplastic syndrome | Dysplastic large RBCs (can also show megaloblastic-type changes) |
| Drugs: hydroxyurea, AZT | Can cause macrocytosis without frank megaloblastic change |
| Pregnancy | Relative macrocytosis; also at risk for folate deficiency |
| Chronic lung disease with hypoxaemia | Compensatory erythrocytosis; reticulocytosis |
| Cold agglutinins/paraproteinaemia | RBC agglutination → falsely elevated MCV on automated count |
| Splenectomy | Loss of "culling" function of spleen → target cells + macrocytes |
Distinguishing Megaloblastic vs Non-Megaloblastic Macrocytosis
| Feature | Megaloblastic | Non-Megaloblastic |
|---|
| RBC shape | Oval macrocytes (macro-ovalocytes) | Round macrocytes |
| Neutrophils | Hypersegmented (diagnostic) | Normal segmentation |
| Bone marrow | Megaloblasts, giant metamyelocytes | Normal precursors |
| B12/Folate | Low | Normal |
| LDH | Markedly elevated | Mildly elevated |
| Reticulocytes | Low | Normal/elevated |
| DNA synthesis | Impaired | Normal |
QUICK EXAM REVISION BOX
Pathognomonic Features to Remember:
| Condition | Hallmark Finding |
|---|
| Megaloblastic anaemia | Hypersegmented neutrophils + macro-ovalocytes (PBS); Giant metamyelocytes (BM) |
| Sickle cell anaemia | Sickle cells + HbSS on electrophoresis |
| IDA | Pencil cells + microcytic hypochromic PBS; ↓ ferritin |
| Haemolytic anaemia | ↑ LDH + ↓ haptoglobin + reticulocytosis + ↑ indirect bilirubin |
| Hereditary spherocytosis | Spherocytes + ↑ osmotic fragility + +ve family history |
Bone Marrow M:E Ratio (Normal = 3:1)
- ↓ M:E ratio (e.g., 1:3) = Erythroid hyperplasia → megaloblastic anaemia, haemolytic anaemia, IDA
- ↑ M:E ratio = Erythroid hypoplasia → aplastic anaemia, pure red cell aplasia
The "Ineffective Erythropoiesis" Concept:
In megaloblastic anaemia: cells made in marrow but die BEFORE reaching circulation → ↑ LDH + ↑ indirect bilirubin BUT low reticulocytes (key differentiator from haemolytic anaemia where reticulocytes are HIGH)
Sources: Goldman-Cecil Medicine International Edition; Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill); Frameworks for Internal Medicine (Wolters Kluwer); Park's Textbook of Preventive and Social Medicine; Robbins Pathologic Basis of Disease (StatPearls supplementary data)