OPHALMOLOGY HISTORY TAKING
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Now I have comprehensive information from Kanski's Clinical Ophthalmology. Let me compile the full, structured response:
Ophthalmology History Taking
Source: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition
Overview
Before examining the patient, a thorough ophthalmic history must be taken. The depth of history depends on the presenting visual symptoms and suspected disease. A basic history is divided into the following categories:
1. Main Complaint (Chief Complaint)
For every symptom, characterize it using these five dimensions:
| Dimension | What to Ask |
|---|---|
| (a) Rapidity of onset | Sudden vs. gradual? Instantaneous (vascular) or over days/weeks (inflammatory/degenerative)? |
| (b) Circumstances of onset | What was the patient doing? Any trauma, systemic illness, or preceding event? |
| (c) Severity | How much does it affect function? Reading, driving, daily activities? |
| (d) Duration | How long have symptoms been present? |
| (e) Frequency | Constant vs. intermittent? Episodic (e.g., angle closure)? |
2. Characterizing Common Ophthalmic Symptoms
Vision Loss
- Monocular vs. binocular - critical for localization (monocular = pre-chiasmal; binocular = chiasmal or post-chiasmal)
- Central vs. peripheral field loss
- Transient vs. permanent (amaurosis fugax = TIA of the eye)
- Sudden painless - consider vascular (CRAO, CRVO, AION)
- Painful - consider acute angle-closure glaucoma, uveitis, optic neuritis
Floaters & Flashes
- New floaters/flashes = posterior vitreous detachment until proven otherwise; must rule out retinal tear or detachment
- Ask about a "curtain" or "shadow" in the visual field (retinal detachment)
Pain
- Sharp/aching - corneal, anterior segment
- Deep/periorbital - acute angle closure, orbital disease, optic neuritis (pain on eye movement)
- Foreign body sensation/grittiness - conjunctiva, cornea, dry eye
Redness
- Acute vs. chronic; unilateral vs. bilateral
- With or without discharge (purulent = bacterial; watery = viral/allergic)
- Ciliary flush (limbal injection) vs. conjunctival injection - ciliary flush indicates anterior segment inflammation
Diplopia
- Monocular (persists when one eye closed) = lens/corneal problem or functional
- Binocular (resolves when one eye closed) = extraocular muscle or cranial nerve pathology
- Constant vs. intermittent; direction of gaze that worsens it
Other Symptoms to Ask About
- Photophobia (uveitis, keratitis, migraine)
- Epiphora / watering (drainage failure vs. hypersecretion - drainage failure worsens in cold/wind)
- Distortion / metamorphopsia (macular disease)
- Halos around lights (corneal edema, acute angle closure)
- Colour vision changes (optic nerve disease)
- Night blindness / nyctalopia (retinitis pigmentosa, vitamin A deficiency)
- Photopsia (flashes of light - vitreoretinal traction)
3. Past Ocular History
- Previous ocular surgery (cataract, glaucoma, refractive surgery - note: refractive surgery affects IOP readings)
- Previous ocular inflammation (uveitis, keratitis)
- Trauma (blunt or penetrating)
- Refractive status - myopia increases risk of POAG and retinal detachment; hypermetropia increases risk of angle-closure glaucoma
- Previous ocular treatments (laser, injections)
- Use of spectacles or contact lenses; compliance and hygiene
4. Past Medical History
Key systemic conditions with ophthalmic relevance:
| Condition | Ophthalmic Relevance |
|---|---|
| Diabetes mellitus | Diabetic retinopathy, macular edema, rubeosis iridis |
| Hypertension | Hypertensive retinopathy, vascular occlusions |
| Cardiovascular disease | Retinal artery/vein occlusions |
| Asthma / heart failure / heart block / peripheral vascular disease | Contraindication to topical beta-blockers (e.g., timolol) |
| Thyroid disease | Thyroid eye disease (Graves' orbitopathy) |
| Autoimmune / connective tissue disorders | Uveitis, scleritis, keratoconjunctivitis sicca |
| Head injury / intracranial pathology / stroke | Optic atrophy, visual field defects |
| Migraine / Raynaud's phenomenon | Vasospasm; implicated in NTG |
| Multiple sclerosis | Optic neuritis, internuclear ophthalmoplegia |
| HIV / immunocompromise | CMV retinitis, toxoplasma, opportunistic infections |
| Oral contraceptive pill (long-term) | May increase risk of glaucoma and CRVO |
5. Systemic Medications
Ask specifically about:
- Corticosteroids (topical, inhaled, oral, skin creams) - steroid-induced glaucoma and cataract
- Tamsulosin (alpha-blocker for BPH) - intraoperative floppy iris syndrome (IFIS) during cataract surgery
- Oral beta-blockers - may lower IOP and mask glaucoma
- Chloroquine / hydroxychloroquine - bull's eye maculopathy (retinal toxicity)
- Ethambutol - optic neuropathy
- Amiodarone - corneal microdeposits, optic neuropathy
- Vigabatrin - peripheral visual field constriction
- Bisphosphonates - scleritis, uveitis (rare)
- Sildenafil (PDE5 inhibitors) - non-arteritic anterior ischaemic optic neuropathy (NAION)
- Isotretinoin - dry eye, blepharitis
- Topical glaucoma medications - note compliance and side effects
6. Allergies
- Drug allergies - especially to:
- Antibiotics (topical or systemic)
- Topical glaucoma medications (e.g., brimonidine causing allergic follicular conjunctivitis)
- Acetazolamide is contraindicated in sulfonamide allergy
- Contact lens solutions
- Preservatives in eye drops (e.g., benzalkonium chloride)
7. Family History
- Glaucoma (primary open-angle glaucoma - strong hereditary component)
- Macular degeneration (AMD has genetic risk factors)
- Inherited retinal dystrophies (retinitis pigmentosa, Stargardt's, Best disease)
- Strabismus and amblyopia
- Refractive errors (myopia especially)
- Systemic conditions with ocular manifestations (Marfan syndrome, NF1/2)
8. Social History
- Occupation - computer use (dry eye), occupational hazards (trauma risk), visual requirements for work (drivers, pilots)
- Hobbies - contact sports, DIY (foreign body risk)
- Driving - legally required vision standards
- Smoking - significantly increases risk of AMD and is a risk factor for CRVO
- Alcohol intake - toxic/nutritional optic neuropathy (suspect if combined with poor nutrition or tobacco)
- Living alone / social support - important for low vision planning
9. Review of Systems (Selected)
Always ask about neurological symptoms alongside ophthalmic complaints:
- Headache (raised ICP, giant cell arteritis, migraine)
- Jaw claudication, scalp tenderness, temporal artery tenderness - giant cell arteritis (emergency in patients >50 with sudden visual loss)
- Facial pain (trigeminal)
- Limb weakness, sensory changes (MS, stroke)
- Skin rashes (sarcoid, herpes zoster)
Summary Framework
HISTORY OF PRESENTING COMPLAINT
→ Onset, Duration, Severity, Frequency, Progression
→ Character of visual/ocular symptom (see above)
PAST OCULAR HISTORY
→ Surgery, Trauma, Inflammation, Refractive status
PAST MEDICAL HISTORY
→ Diabetes, HTN, CVS, Autoimmune, Neurological
DRUG HISTORY
→ Steroids, Tamsulosin, Antimalarials, Topical drops
ALLERGIES
→ Drug, preservative, contact lens solution
FAMILY HISTORY
→ Glaucoma, AMD, Retinal dystrophy
SOCIAL HISTORY
→ Occupation, Driving, Smoking, Alcohol
Based on Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition - the gold standard ophthalmic reference. All key categories (main complaint, past ocular history, past medical history, systemic medications, allergies, family history, occupation and hobbies) are taken directly from the textbook's Ophthalmic History framework.
Vision defect
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive material to compile a thorough and well-illustrated response on vision defects.
Vision Defects
Vision defects can be broadly divided into two major categories:
- Refractive errors - defects in the optical focusing system of the eye
- Visual field defects - loss of specific areas of vision due to pathology along the visual pathway
Part 1: Refractive Errors
Refractive errors occur when the eye cannot focus light precisely on the retina, resulting in blurred vision.
| Type | Mechanism | Far/Near Vision | Correction |
|---|---|---|---|
| Myopia (short-sightedness) | Eyeball too long / cornea too curved; light focuses in front of retina | Far vision blurred, near clear | Concave (diverging) lens |
| Hypermetropia (long-sightedness) | Eyeball too short / cornea too flat; light focuses behind retina | Near blurred, far may be clear | Convex (converging) lens |
| Astigmatism | Irregular curvature of cornea or lens; different focal points in different meridians | Both near and far blurred/distorted | Cylindrical lens |
| Presbyopia | Age-related loss of accommodation (lens stiffening); reduced near focus | Near vision lost after ~45 years | Reading glasses / bifocals |
| Anisometropia | Significant difference in refractive error between the two eyes | Unequal blur; risk of amblyopia | Glasses / contact lenses |
Clinical notes:
- Myopia is a risk factor for primary open-angle glaucoma (POAG) and retinal detachment
- Hypermetropia is a risk factor for primary angle-closure glaucoma (PACG) and accommodative esotropia in children
- Refractive surgery (LASIK, PRK) alters corneal curvature and can affect IOP readings - always document in history
Part 2: Visual Field Defects - Classification by Anatomy
The visual pathway runs: Retina → Optic nerve → Optic chiasm → Optic tract → Lateral Geniculate Nucleus (LGN) → Optic radiations → Primary visual cortex (V1, occipital lobe)
The anatomical site of any lesion determines the pattern of visual field loss. The key principle:
- Pre-chiasmal lesions = monocular defects (one eye only)
- Chiasmal lesions = bitemporal defects
- Post-chiasmal (retrochiasmal) lesions = homonymous (same-sided) defects in both eyes
Visual Pathway Diagram
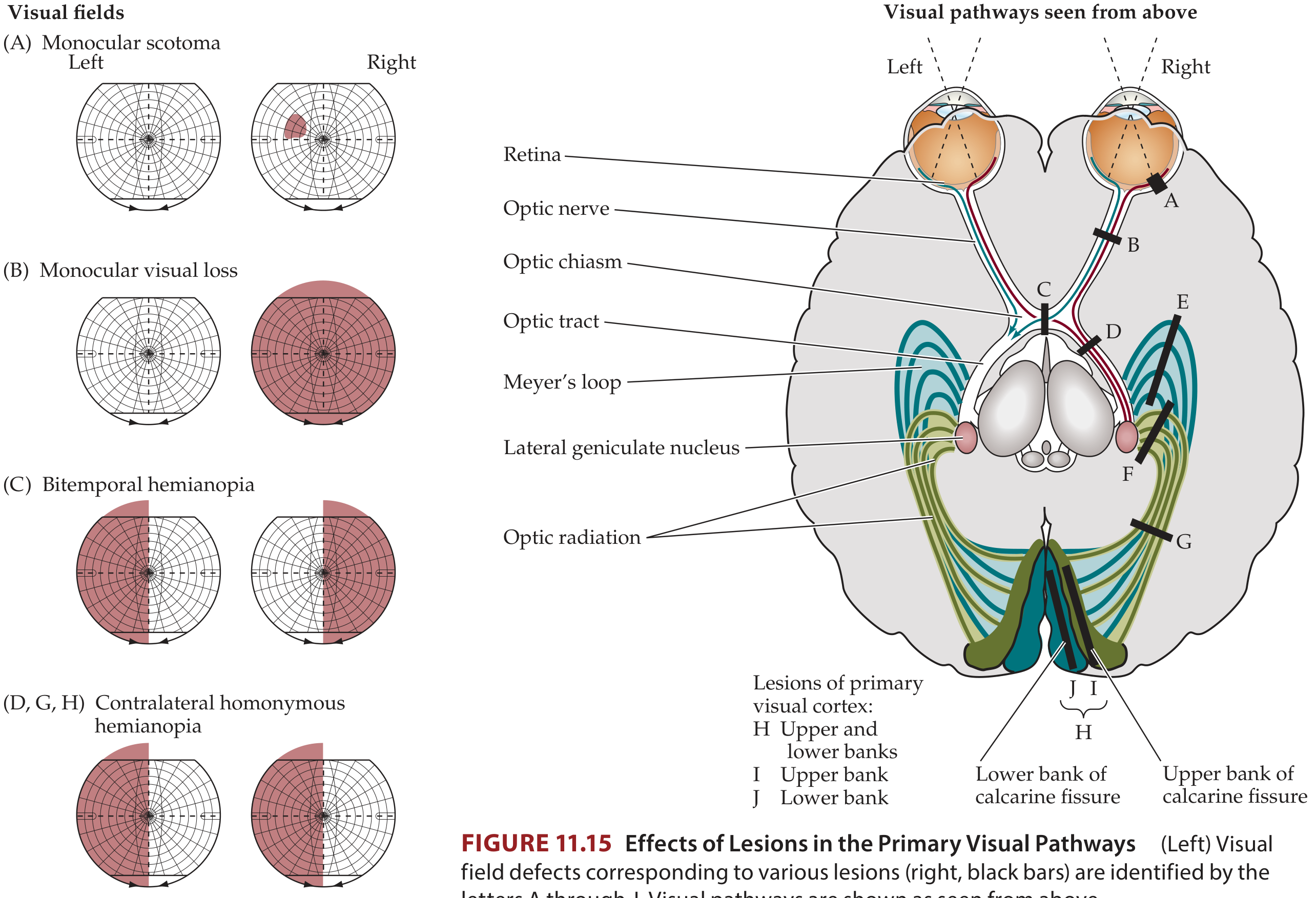
Fig. 11.15 - Effects of lesions at each level of the visual pathway and the corresponding field defects (Neuroanatomy through Clinical Cases, 3rd Ed.)
Lesion-by-Lesion Summary
A. Retina
- Causes monocular scotoma - a localized blind spot in one eye only
- Shape corresponds to the retinal area affected
- Almost always accompanied by ophthalmoscopic abnormalities (can be seen on fundoscopy)
- Patients may also complain of metamorphopsia (distortion), micropsia, or photopsias
- Common causes: retinal infarct, retinal detachment, haemorrhage, degeneration, infection
B. Optic Nerve (complete)
- Causes total monocular visual loss (blindness in one eye)
- Relative afferent pupillary defect (RAPD) is present
- Common causes: glaucoma, optic neuritis, anterior ischaemic optic neuropathy (AION), optic glioma, meningioma, trauma, raised intracranial pressure
C. Optic Chiasm
- Causes bitemporal hemianopia - loss of the outer (temporal) halves of both visual fields
- Often asymmetric in practice
- The nasal fibres from each eye cross here - compression disrupts them, leaving only temporal field from each eye
- Common causes: pituitary adenoma (most common), craniopharyngioma, meningioma, hypothalamic glioma
D. Optic Tract / LGN
- Causes contralateral homonymous hemianopia (incongruous - fields not perfectly matched)
- At the LGN, unusual sectoranopias ("keyhole" pattern) can occur
- Common causes: tumour, infarct, demyelination; toxoplasmosis / infection (LGN)
E. Temporal Lobe (Meyer's Loop)
- The lower optic radiations loop through the temporal lobe
- Lesion causes contralateral superior quadrantanopia ("pie in the sky")
- Common causes: MCA inferior division infarct, temporal lobe tumour, abscess, surgery (temporal lobectomy)
F. Parietal Lobe
- The upper optic radiations pass through the parietal lobe
- Lesion causes contralateral inferior quadrantanopia ("pie on the floor")
- Common causes: MCA superior division infarct, parietal tumour
G. Entire Optic Radiation
- Complete damage causes contralateral homonymous hemianopia (similar to optic tract lesion but more congruous)
H/I/J. Primary Visual Cortex (Occipital Lobe - PCA territory)
- Upper bank of calcarine fissure → contralateral inferior quadrantanopia
- Lower bank → contralateral superior quadrantanopia
- Both banks (entire cortex) → contralateral homonymous hemianopia, often with macular sparing
- Common causes: PCA infarct, tumour, haemorrhage, occipital trauma
Macular sparing - seen in cortical lesions; the foveal representation may receive collateral blood supply from both PCA and MCA, so central vision is preserved even when peripheral homonymous hemianopia is present.
Types of Scotomas (Localized Field Defects)
| Scotoma Type | Description | Common Causes |
|---|---|---|
| Central scotoma | Loss at the point of fixation | Optic neuritis, macular disease, toxic optic neuropathy |
| Cecocentral scotoma | Extends from blind spot to central fixation | Papillomacular bundle damage; toxic/hereditary optic neuropathy (e.g., Leber's, alcohol-tobacco amblyopia) |
| Paracentral scotoma | Small depression near fixation | Early glaucoma (especially NTG), early macular disease |
| Arcuate (Bjerrum) scotoma | Arc-shaped defect from blind spot, following nerve fibre bundles | Glaucoma, AION, optic nerve drusen |
| Nasal step | Sensitivity difference above/below horizontal in nasal field | Glaucoma |
| Altitudinal defect | Upper or lower half of field lost | AION (anterior ischaemic optic neuropathy), branch retinal artery occlusion |
| Ring scotoma | Preserved central + peripheral vision, loss in between | Retinitis pigmentosa, advanced glaucoma (arcuates merge) |
| Enlarged blind spot | Extension of the physiological blind spot | Papilloedema (raised ICP), peripapillary disease |
| Tunnel vision | Only a small central island remains | Advanced glaucoma, retinitis pigmentosa |
Glaucomatous Visual Field Progression (Kanski)
A classic and clinically important sequence:
- Increased response variability (earliest sign)
- Paracentral depressions (especially superonasal) - more common in NTG
- Nasal step (horizontal midline boundary in nasal field)
- Arcuate scotoma - coalescence of paracentral scotomas, extending from blind spot (10-20° from fixation)
- Ring scotoma - superior and inferior arcuates merge
- End-stage - small central island + temporal island of vision
- Kanski's Clinical Ophthalmology, 10th Ed.
Quick Localization Reference
MONOCULAR defect
→ Retina or Optic nerve (pre-chiasmal)
BITEMPORAL hemianopia
→ Optic chiasm (pituitary region)
HOMONYMOUS hemianopia (same side, both eyes)
→ Optic tract / LGN / optic radiation / cortex (post-chiasmal)
→ Incongruous = more anterior (tract/LGN)
→ Congruous + macular sparing = cortical (occipital)
SUPERIOR quadrantanopia ("pie in sky")
→ Temporal lobe (Meyer's loop)
INFERIOR quadrantanopia ("pie on floor")
→ Parietal lobe or upper calcarine bank
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach 10th Ed.; Neuroanatomy through Clinical Cases 3rd Ed.; Localization in Clinical Neurology 8th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.