Hematuria pediatrics
Reading File
Finding Sources
Searching PubMed
hematuria children evaluation management
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
pediatric hematuria evaluation algorithm approach children
Finding Sources
Loading Image
Here is a comprehensive overview of pediatric hematuria:
Hematuria in Children
Definition
- Gross hematuria: red blood cells visible to the naked eye, confirmed by urine dipstick for blood.
- Microscopic hematuria: clear yellow urine with a positive urine dipstick, confirmed as >5 RBCs/high-power field on a freshly spun specimen. For microscopic hematuria to be considered significant, it should be found on >2 separate occasions.
Epidemiology
- Isolated microscopic hematuria occurs in approximately 1% of school-age children.
- < 25% of these children will have hematuria on repeated testing; most resolve spontaneously within 1 year.
- Gross hematuria is rarer, accounting for ~0.1–0.13% of pediatric emergency visits.
- A definitive diagnosis is established in < 30% of isolated microscopic hematuria cases.
Causes
BOX: Causes of Hematuria in Children (Campbell Walsh Wein Urology)
| Macroscopic | Microscopic |
|---|---|
| Transient | Transient |
| Hypercalciuria / nephrolithiasis | Hypercalciuria / nephrolithiasis |
| Glomerulonephritis (all types) | Glomerulonephritis (all types) |
| Cystitis | Cystitis / pyelonephritis |
| Exercise | Exercise |
| Congenital anomalies of the urinary tract | Congenital anomalies of the urinary tract |
| Benign urethrorrhagia | Thin basement membrane disease |
| Wilms tumor / bladder tumor | Drugs |
| Bleeding dyscrasia | Interstitial nephritis |
| Renal vein thrombosis | Sickle cell disease/trait |
| Papillary necrosis | |
| Nutcracker syndrome |
Most Common Diagnoses in Gross Hematuria (pediatric ED):
- UTI (26%)
- Perineal irritation (11%)
- Trauma (7%)
- Meatal stenosis with ulceration (7%)
- Coagulation abnormalities (3%)
- Nephrolithiasis (2%)
- Less common: sickle cell disease/trait, glomerular disease, malignancy, benign idiopathic urethrorrhagia
Initial Evaluation
History
Key points to elicit:
- Painless vs. painful, intermittent vs. persistent, gross vs. microscopic
- Associated symptoms: trauma, abdominal pain, fever, dysuria, voiding dysfunction, rash, joint pain, weight gain/edema, headaches, visual changes
- Family history: hematuria, bleeding disorders, hearing loss, urolithiasis, sickle cell disease, renal disease
Physical Examination
- Blood pressure (hypertension suggests glomerular disease)
- Rashes, joint abnormalities, edema
- Abdominal/flank tenderness or masses
- Perineal abnormalities
Urine Examination — Critical First Step
| Urine color | Interpretation |
|---|---|
| Red/grossly bloody | Nonglomerular bleeding |
| Brown / "tea-colored" | Glomerular origin |
| Positive dipstick, no RBCs on microscopy | Hemoglobinuria or myoglobinuria |
- Dysmorphic / "crenated" RBCs → glomerular disease
- Normal RBC morphology → lower urinary tract bleeding
- RBC casts → defines glomerulonephritis
- Crystals → urolithiasis
- WBCs/bacteria → UTI
Evaluation Framework
Isolated Microscopic Hematuria (asymptomatic, no proteinuria, unremarkable family history)
- Test parents for hematuria
- Measure urinary calcium excretion (spot urine Ca/Cr ratio)
- Renal ultrasound yield is low; do only if hematuria persists for several months with relevant clinical findings
- Voiding cystourethrogram and cystoscopy are NOT indicated
- Observe and retest in 6–12 months
Microscopic Hematuria with Positive History/Abnormal Findings
- CBC, serum electrolytes, creatinine, albumin
- C3, C4 (complement levels)
- ASO titer / anti-DNase B (post-streptococcal GN)
- ANA (lupus nephritis)
- Quantitative urine protein (protein/creatinine ratio)
- Individualized: hearing screen (Alport syndrome), hemoglobin electrophoresis (sickle cell), imaging, genetic testing
Glomerular Disease Suspected (proteinuria + hypertension + edema)
- Baseline renal function, electrolytes, CBC, albumin, C3/C4, ASO
- Refer to pediatric nephrologist
Gross Hematuria
- Thorough history + exam
- Urinalysis + urine culture
- Renal sonogram
- If persistent with no identifiable cause → cystoscopy with retrograde pyelograms
- If cause still not apparent (especially with proteinuria) → refer to pediatric nephrologist
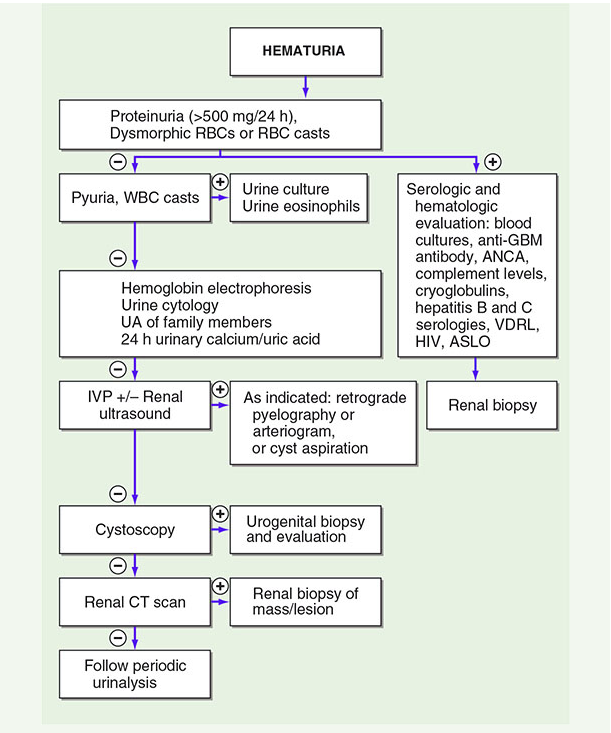
Diagnostic Flowchart
Specific Conditions
IgA Nephropathy (Berger Disease)
- Most common glomerulonephritis worldwide
- Occurs most commonly in children and young adults, male predominance
- Classic: gross hematuria 1–2 days after upper respiratory infection ("synpharyngitic hematuria")
- Normal complement levels; diagnosis by biopsy (mesangial IgA deposits)
Post-Streptococcal Glomerulonephritis (PSGN)
- UA shows hematuria ± RBC casts + proteinuria ± pyuria
- Low C3, normal C4
- ASO titer elevated
Alport Syndrome
- X-linked hereditary nephritis; think of it with family history of progressive renal disease + hearing loss + ocular abnormalities
- Thin GBM on biopsy
Hypercalciuria
- A common cause of isolated hematuria; spot urine Ca/Cr > 0.2 mg/mg is abnormal
- Predisposes to nephrolithiasis
Benign Idiopathic Urethrorrhagia
- Bloody spotting of underwear in prepubertal/pubertal boys
- Mean age ~10 years; up to one-third have concomitant dysuria
- Urine culture and renal US uniformly normal
- Management: watchful waiting — >90% resolve within 2 years
- If persists beyond 2 years: retrograde urethrography or cystoscopy (evaluate for urethral stricture)
- Note: these boys are at increased risk for urethral stricture — minimize instrumentation
Nutcracker Syndrome
- Compression of the left renal vein between the aorta and superior mesenteric artery → gross hematuria
- Diagnosed by Doppler ultrasound or CT angiography
Wilms Tumor
- Should be considered in a child with gross hematuria + abdominal mass
- Renal ultrasound or CT for evaluation
Indications for Renal Biopsy
- Persistent hematuria + significant proteinuria
- Hematuria + hypertension
- Hematuria + decreased GFR
- Hematuria + systemic disease features (rash, arthritis, complement abnormalities)
- Family history of progressive renal disease
Key Points Summary
- Isolated microscopic hematuria → ~1% of school-age children; mostly benign, resolves in 1 year
- "Tea-colored" urine + RBC casts → glomerular origin; refer to pediatric nephrology
- Gross hematuria + no RBCs on microscopy + positive dipstick → think hemoglobinuria/myoglobinuria
- UTI is the most common cause of gross hematuria in children
- Cystoscopy and VCUG are not routine for isolated microscopic hematuria
- Supratherapeutic anticoagulation can cause hematuria; therapeutic levels do not
Sources: Campbell Walsh Wein Urology (3-Volume Set), p. 457–521; Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.