What happened when injury occurs on medulla
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
I now have comprehensive information to provide a detailed, well-organized answer. Let me compose it.
Injury to the Medulla Oblongata
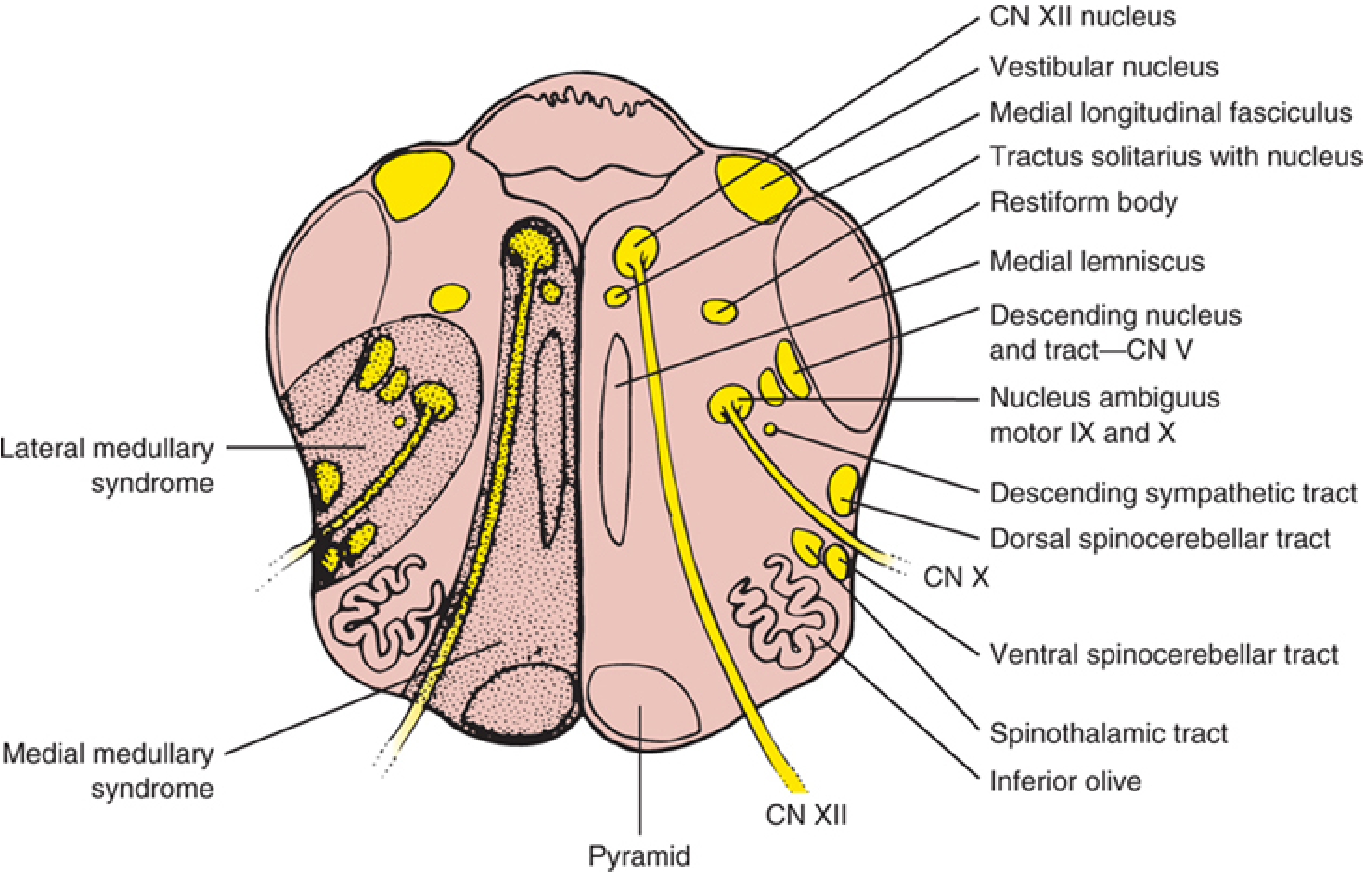
The medulla oblongata, the most caudal part of the brainstem, contains critical structures: cranial nerve nuclei (IX, X, XII), the corticospinal pyramids, medial lemniscus, spinothalamic tract, vestibular nuclei, nucleus ambiguus, descending sympathetic fibers, and the inferior cerebellar peduncle. Injury produces distinct clinical syndromes depending on whether the lateral or medial portion is affected.
1. Lateral Medullary Syndrome (Wallenberg Syndrome)
The most common medullary syndrome, caused most often by occlusion of the vertebral artery or posterior inferior cerebellar artery (PICA). It damages a wedge-shaped area of the lateral medulla and produces:
| Feature | Structure Damaged | Side |
|---|---|---|
| Facial pain/temperature loss | Spinal nucleus & tract of CN V | Ipsilateral |
| Body pain/temperature loss | Spinothalamic tract | Contralateral |
| Dysphagia, dysarthria, hoarseness | Nucleus ambiguus (CN IX, X) | Ipsilateral |
| Horner syndrome (ptosis, miosis, anhidrosis) | Descending sympathetic fibers | Ipsilateral |
| Cerebellar ataxia, falling toward lesion | Inferior cerebellar peduncle | Ipsilateral |
| Vertigo, nausea, vomiting, nystagmus | Vestibular nuclei | Present |
| Hiccups (singultus) | Dorsolateral medullary tegmentum | Variable |
The classic triad that clinically identifies lateral medullary infarction is: Horner syndrome + ipsilateral ataxia + contralateral hyalgesia (pain/temperature loss).
Key features of the sensory loss pattern:
- The ipsilateral face and contralateral body pattern (alternating/crossed hemianesthesia) is the hallmark - due to the facial pain fibers crossing at a different level than the body fibers.
- Motor power (corticospinal pyramids) and proprioception/vibration (medial lemniscus) are typically spared because those structures lie in the medial medulla.
2. Medial Medullary Syndrome (Dejerine Syndrome)
Less common, caused by occlusion of the anterior spinal artery, vertebral artery, or lower basilar artery, damaging the paramedian medulla (pyramid, medial lemniscus, CN XII nucleus and fascicles).
| Feature | Structure Damaged | Side |
|---|---|---|
| Tongue weakness/deviation (LMN type) | CN XII nucleus/fasciculus | Ipsilateral (tongue deviates toward lesion) |
| Hemiplegia (spares face) | Corticospinal pyramid | Contralateral |
| Loss of position sense and vibration | Medial lemniscus | Contralateral |
| Pain/temperature sensation | Spinothalamic tract (spared) | Usually intact |
| Upbeat nystagmus (occasional) | Medial longitudinal fasciculus extension | Variable |
Bilateral medial medullary infarction produces: flaccid quadriplegia with facial sparing, bilateral tongue LMN palsy, complete loss of position/vibration sense in all four limbs, and respiratory failure.
A rare variant is hemiplegia cruciata - ipsilateral arm paralysis with contralateral leg paralysis - from a low medullary lesion disrupting the decussating corticospinal fibers differently for the arm vs. leg.
3. Hemimedullary Syndrome (Babinski-Nageotte)
When both lateral and medial zones are simultaneously infarcted (from occlusion of the ipsilateral vertebral artery proximal to PICA and the anterior spinal artery), features of both syndromes combine:
- Ipsilateral CN XII palsy + contralateral hemiplegia (medial)
- Ipsilateral Horner + facial numbness + ataxia + crossed body sensory loss (lateral)
4. Medullary Hemorrhage
Primary medullary hemorrhage is rare; most are extensions from pontine hematomas. The clinical presentation typically includes:
- Ipsilateral hypoglossal nerve palsy (CN XII)
- Contralateral hemiparesis
These two features together help distinguish medullary hemorrhage from the classical Wallenberg syndrome (which is caused by infarction and typically spares motor and tongue function). - Bradley and Daroff's Neurology in Clinical Practice
5. Life-Threatening Consequences
The medulla also contains the vital centers for cardiorespiratory control:
- Respiratory rhythm centers (pre-Botzinger complex)
- Cardiovascular control centers
- Vomiting center
Extensive medullary damage (e.g., from herniation, hemorrhage, or bilateral infarction) can cause apnea, cardiac arrest, and death. This is why transtentorial or tonsillar herniation compressing the medulla is rapidly fatal.
Summary Table
| Zone | Syndrome | Key Ipsilateral | Key Contralateral |
|---|---|---|---|
| Lateral | Wallenberg | Facial numbness, Horner, ataxia, dysphagia | Body pain/temp loss |
| Medial | Dejerine | Tongue weakness (LMN) | Hemiplegia, vibration/position loss |
| Both | Hemimedullary | Combined above | Combined above |
| Bilateral medial | -- | Quadriplegia, respiratory failure | -- |
- Localization in Clinical Neurology, 8e, pp. 918-922
- Bradley and Daroff's Neurology in Clinical Practice, p. 1437
This is a shared conversation. Sign in to Orris to start your own chat.