Ocular sonography in emergency room
Reading File
Finding Sources
Searching PubMed
ocular ultrasound emergency point-of-care
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive content from four major EM textbooks plus excellent images. Let me compile the full answer.
Ocular Sonography in the Emergency Room
Bedside (point-of-care) ocular ultrasound is one of the most valuable POCUS applications in emergency medicine. It is fast, non-invasive, requires no radiation, and can be performed even when the eye cannot be examined directly due to swelling, trauma, or an uncooperative patient.
Indications
Ocular US is appropriate for evaluation of:
- Altered or lost vision
- Ocular pain or trauma
- Suspected intraocular foreign body (FB)
- Headache or altered mental status (when elevated ICP is a concern)
- Head injury with facial swelling obscuring direct exam
Conditions reliably diagnosed include: retinal detachment, vitreous hemorrhage, posterior vitreous detachment, lens dislocation, intraocular foreign body, globe rupture, elevated intraocular pressure, and elevated intracranial pressure (via optic nerve sheath diameter, ONSD). Pupillary size and extraocular movements can also be assessed even with periorbital swelling.
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, p. 1484
- Rosen's Emergency Medicine, p. 3626
Contraindications
There are no absolute contraindications, but important caveats apply:
- Known or suspected open globe: Rosen's states ocular US is contraindicated with confirmed globe rupture. Roberts & Hedges' takes a more nuanced position: if globe rupture is possible but not obvious, a careful no-pressure technique is justified because the benefit of rapid diagnosis outweighs the risk. If physical exam obviously suggests open globe, the procedure is discouraged due to the risk of vitreous extrusion.
- Excessive orbital or periorbital emphysema will obscure images.
Equipment and Setup
-
Transducer: High-frequency linear array, 7.5-10 MHz or higher
-
Use the ocular machine preset to minimize thermal bioeffects
-
Place patient supine or semi-reclined
-
Instruct patient to keep eyes gently closed, looking straight ahead, without clenching
-
Apply a Tegaderm dressing over the closed eyelid (optional but helpful), then a copious amount of gel over the eyelid/dressing to form an acoustic window
-
Stabilize the probe by resting the hand on the patient's forehead, nose bridge, or maxilla
-
Use the no-pressure technique - barely touch the probe to the gel without compressing the eyelid
-
Roberts & Hedges', p. 1485
Scanning Technique
- Scan in orthogonal planes (transverse and longitudinal) with both low- and high-gain settings
- Adjust depth to visualize the full globe and ~1 cm of the optic nerve posteriorly
- Identify normal anatomy: anterior chamber, iris, lens (echogenic biconvex structure), vitreous (anechoic), retina, optic disc
- Use kinetic echography: ask the patient to move gaze side to side - this helps differentiate retinal detachment (moves with the eye) from vitreous hemorrhage (remains horizontal/settles)
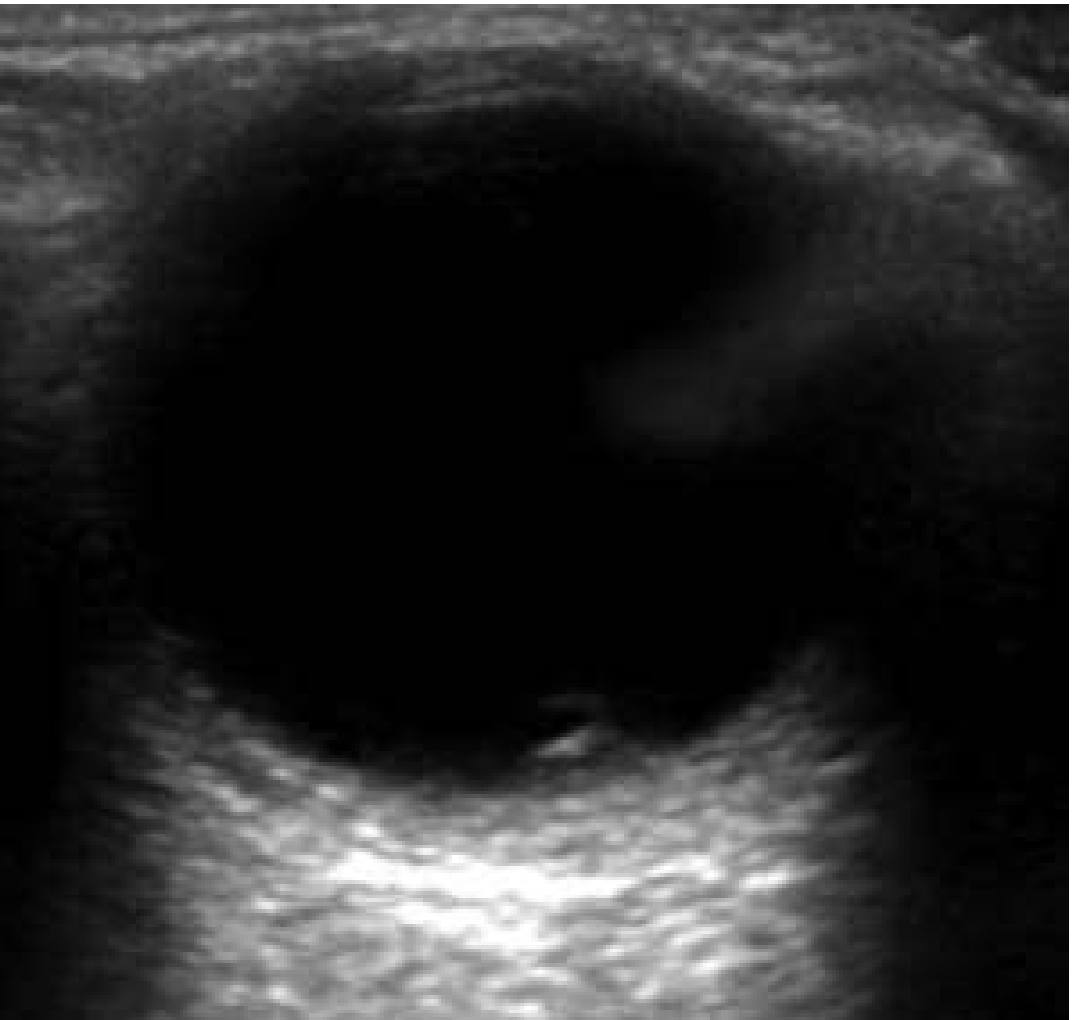
Normal eye appearance:

Pathological Findings
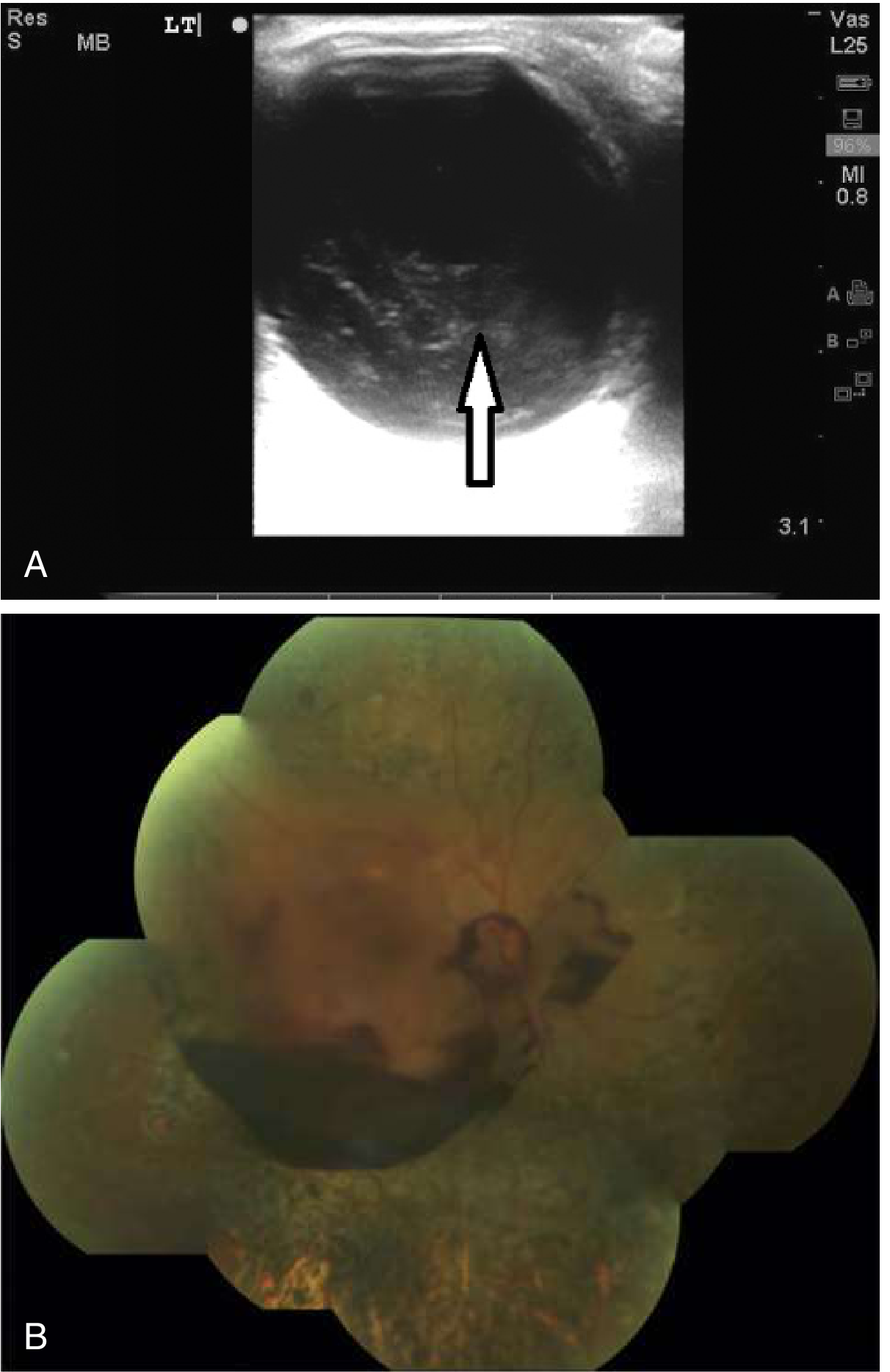
1. Retinal Detachment
The retina appears as a billowing, hyperechoic line in the posterior anechoic vitreous. Key features:
- Undulates with eye movement
- Tethered at the optic disc and ora serrata; the flap crosses the midline of the posterior pole (vs. vitreous detachment, which does not cross the optic nerve)
- Sensitivity ~92%, specificity ~91.4% when performed by emergency physicians
- False negatives occur when retinal detachment is mistaken for vitreous detachment or hemorrhage, often due to improper technique or insufficient gain
- Rosen's Emergency Medicine, p. 900
2. Vitreous Hemorrhage
- Appears as echogenic debris within the anechoic posterior chamber
- Mild: scattered echoes. Severe: diffuse echogenic fill
- Does not move with eye movement (settles horizontally) - key differentiator from retinal detachment
- Hemorrhage may be evenly distributed or focal ("boat-shaped" pre-retinal hemorrhage in the subhyaloid space)
- If afferent pupillary defect (APD) is present alongside vitreous hemorrhage, suspect an underlying retinal detachment
- Rosen's Emergency Medicine, p. 900; Tintinalli's Emergency Medicine, p. 1601
3. Retinal vs. Vitreous Detachment: Key Differentiators
| Feature | Retinal Detachment | Vitreous Hemorrhage/Detachment |
|---|---|---|
| Movement with gaze | Undulates, moves with eye | Remains horizontal, settles |
| Location | Posterior pole, near optic disc | Mid-posterior chamber |
| Echogenicity | Hyperechoic linear membrane | Echogenic debris |
| APD | Present if large | Usually absent |
| Optic nerve crossing | Crosses (attached at disc) | Does not cross disc |
4. Globe Rupture
- Look for loss of the normal spherical shape, collapse or deformity of the globe
- Associated findings: irregular contour, intraocular air, lens dislocation, posterior acoustic shadowing from intraocular FB
- US has 94% correlation with CT for orbital fractures
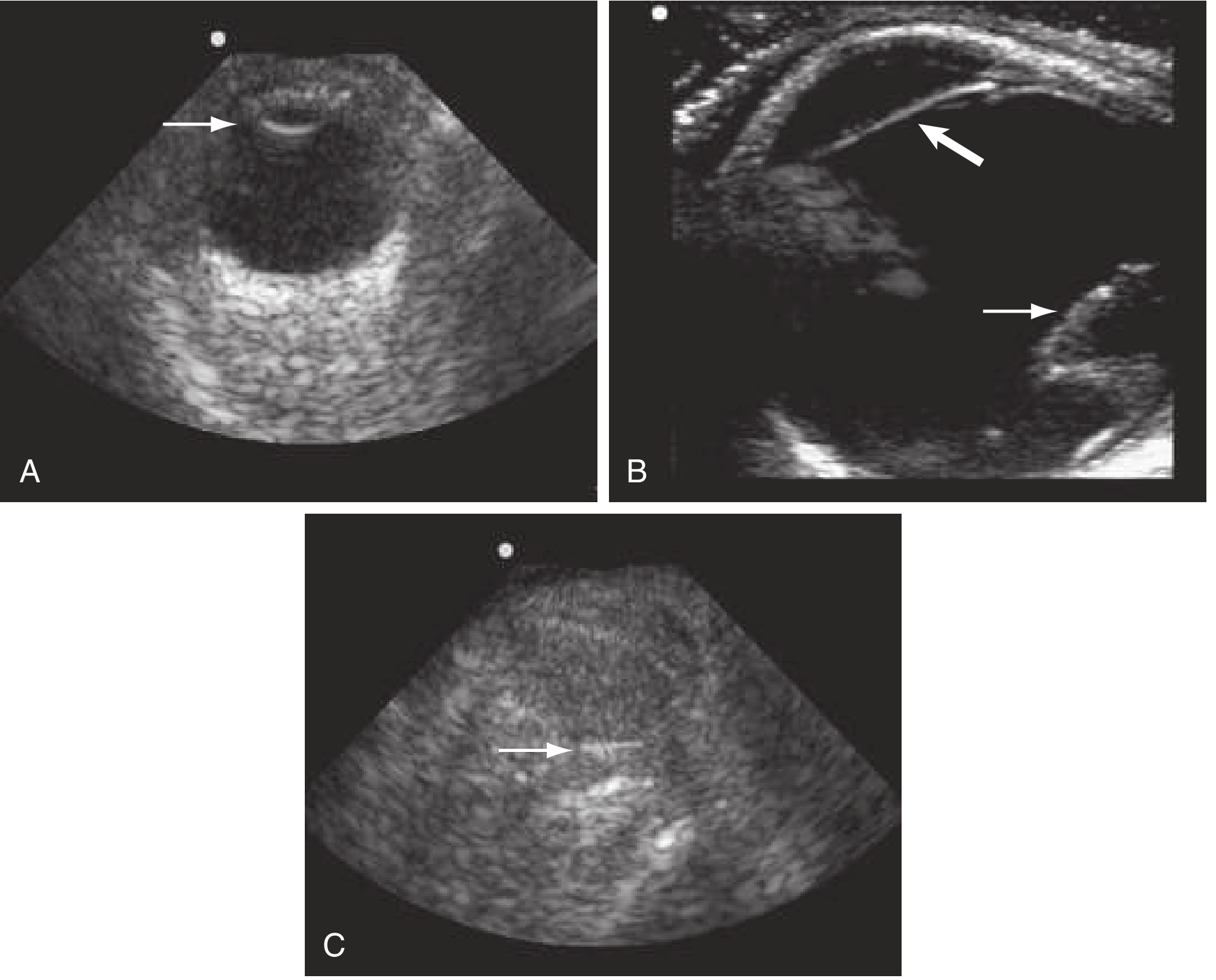
5. Intraocular Foreign Body
- Appears as a bright, hyperechoic focus with posterior acoustic shadowing or reverberation artifact
- Metallic FBs produce characteristic "comet tail" artifact
- Can be seen even when obscured on plain radiograph
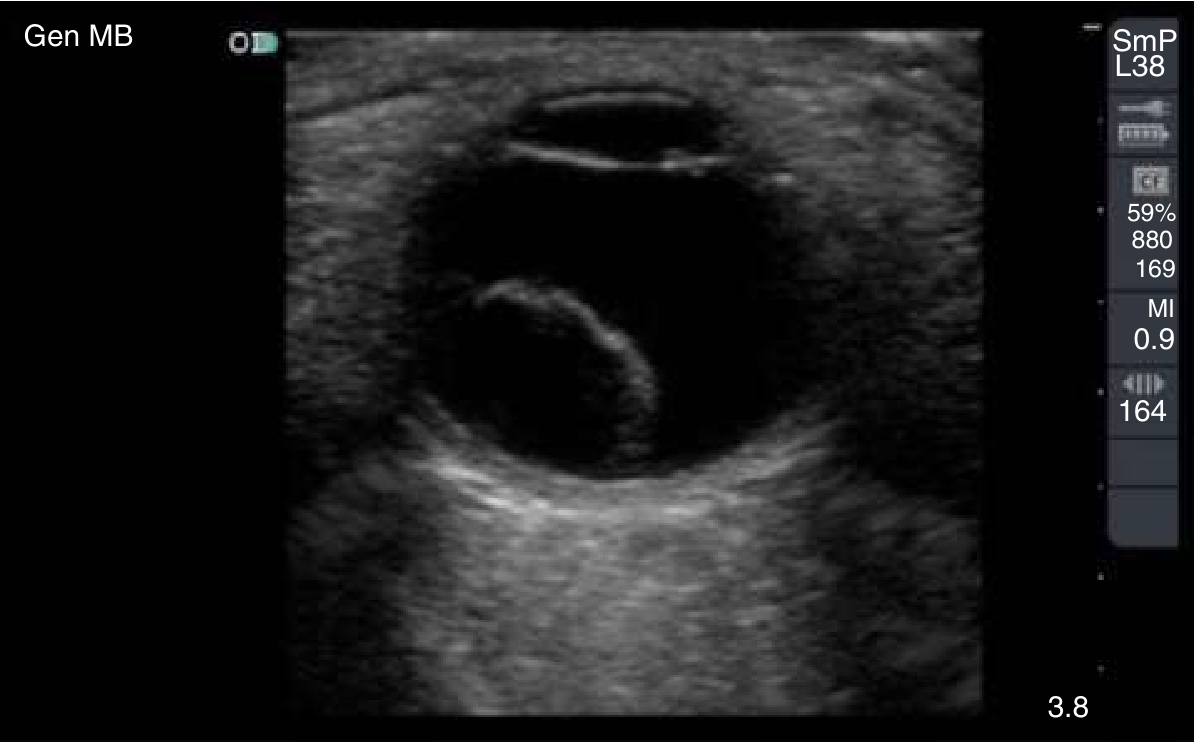
6. Lens Dislocation
- Normal lens is a biconvex, strongly echogenic structure in the anterior chamber
- Dislocation: lens absent from expected location, may be visible in the vitreous posteriorly
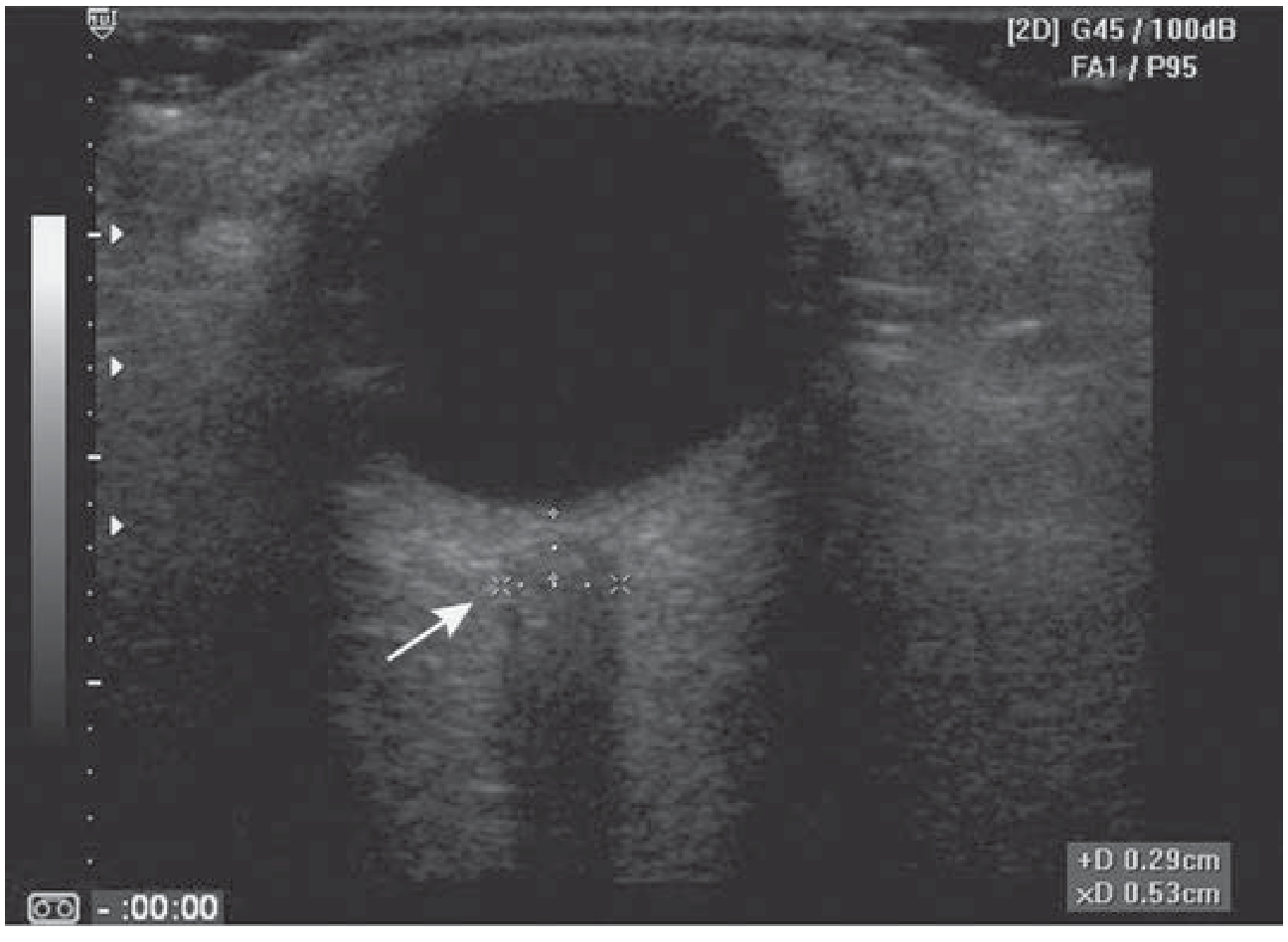
Optic Nerve Sheath Diameter (ONSD) for Elevated ICP
The optic nerve sheath communicates with the subarachnoid space and dilates when ICP rises. Measuring ONSD is a rapid, non-invasive surrogate for ICP.
Technique:
- Place linear probe over closed eyelid
- Ask patient to deviate gaze ~10 degrees laterally (aligns nerve with the beam, avoids false widening)
- Measure ONSD 3 mm posterior to the retina (best contrast and reproducibility at this point)
- Obtain at least 2-3 measurements and average them
- Measure both eyes
Thresholds:
| Population | Normal ONSD | Elevated ICP threshold |
|---|---|---|
| Adults | ≤ 5.0 mm | > 5.7-6.0 mm |
| Children | ≤ 4.5 mm | - |
| Infants | ≤ 4.0 mm | - |
- Sensitivity 87-95%, specificity 79-100% for ICP > 20 mmHg at cutoff of 5.7-6.0 mm
- Differential for elevated ONSD: elevated ICP, anterior orbital mass, optic neuritis, trauma, cavernous sinus mass
- Tintinalli's Emergency Medicine, p. 1601; Roberts & Hedges', p. 1485-1486; Rosen's Emergency Medicine
Complications
- Inadvertent pressure on a ruptured globe can worsen injury or cause vitreous extrusion
- Excessive scan time can exceed thermal exposure limits - use the ocular preset and minimize dwell time
Summary Table
| Condition | Ultrasound Finding |
|---|---|
| Retinal detachment | Hyperechoic linear membrane tethered at disc; moves with eye |
| Vitreous hemorrhage | Echogenic debris in posterior chamber; settles, doesn't cross disc |
| Globe rupture | Loss of spherical shape, deformity, collapsed globe |
| Lens dislocation | Absent lens from anterior chamber; may be in vitreous |
| Intraocular FB | Bright echogenic focus ± shadowing/reverberation |
| Elevated ICP | ONSD > 5.7-6.0 mm at 3 mm posterior to retina |
| Papilledema | Optic disc swelling visible at posterior pole |
Sources:
- Rosen's Emergency Medicine, Chapters 34 & 57 (ocular US, retinal detachment, vitreous hemorrhage)
- Roberts & Hedges' Clinical Procedures in Emergency Medicine, Chapter 62 (bedside ED ocular US)
- Tintinalli's Emergency Medicine, Chapter 241 (ocular US, ONSD measurement)
This is a shared conversation. Sign in to Orris to start your own chat.