Epidemiological triad
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from Park's Textbook. Here is the full, well-structured answer:
Epidemiological Triad
Background and Origin
The germ theory of disease had a key limitation: not everyone exposed to a pathogen develops disease. For example, not everyone exposed to Mycobacterium tuberculosis develops TB - an undernourished or immunocompromised host is far more vulnerable. Similarly, not all exposed to beta-haemolytic streptococci develop acute rheumatic fever. This demanded a broader framework, which synthesized the three fundamental causative factors: Agent, Host, and Environment.
- Park's Textbook of Preventive and Social Medicine, p. 44
The Classic Triad
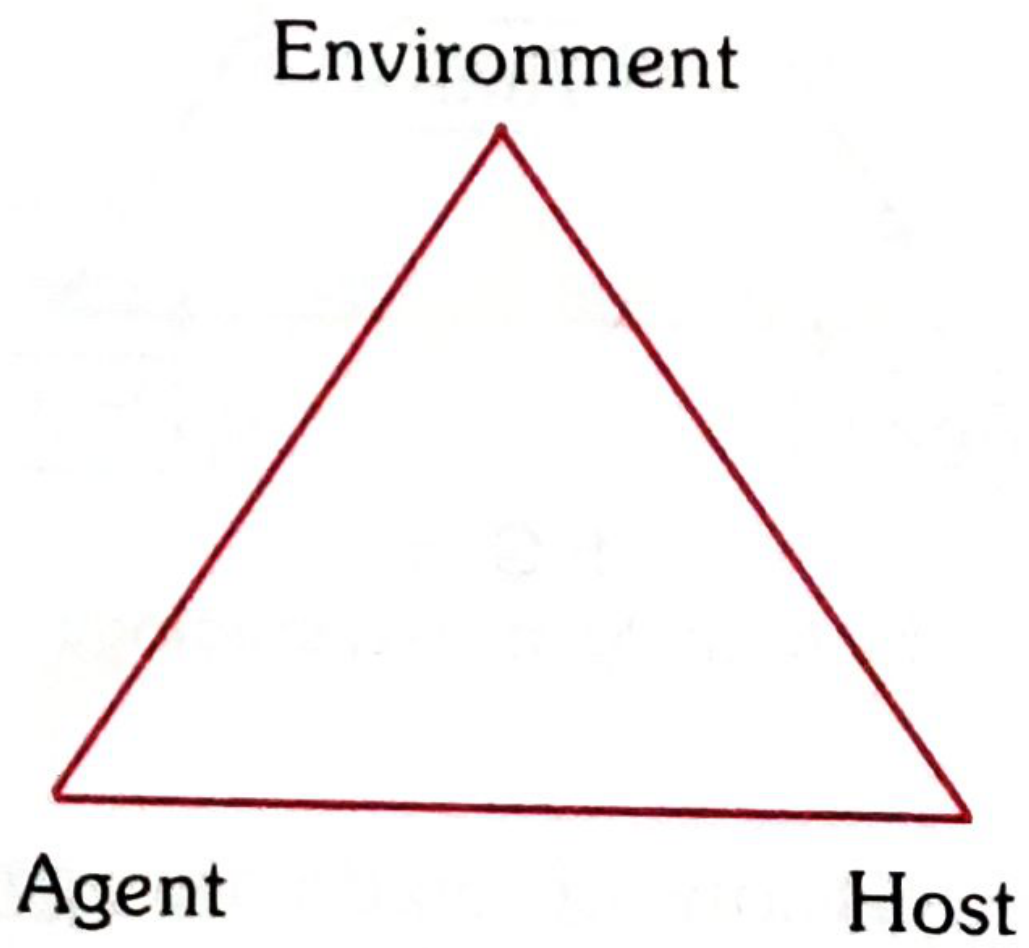
The three vertices of the triangle represent three interacting classes of factors. Disease results when the balance among them is disturbed.
The Triangle of Epidemiology (with Time)
The traditional triangle model adds Time as a central element within the triad:
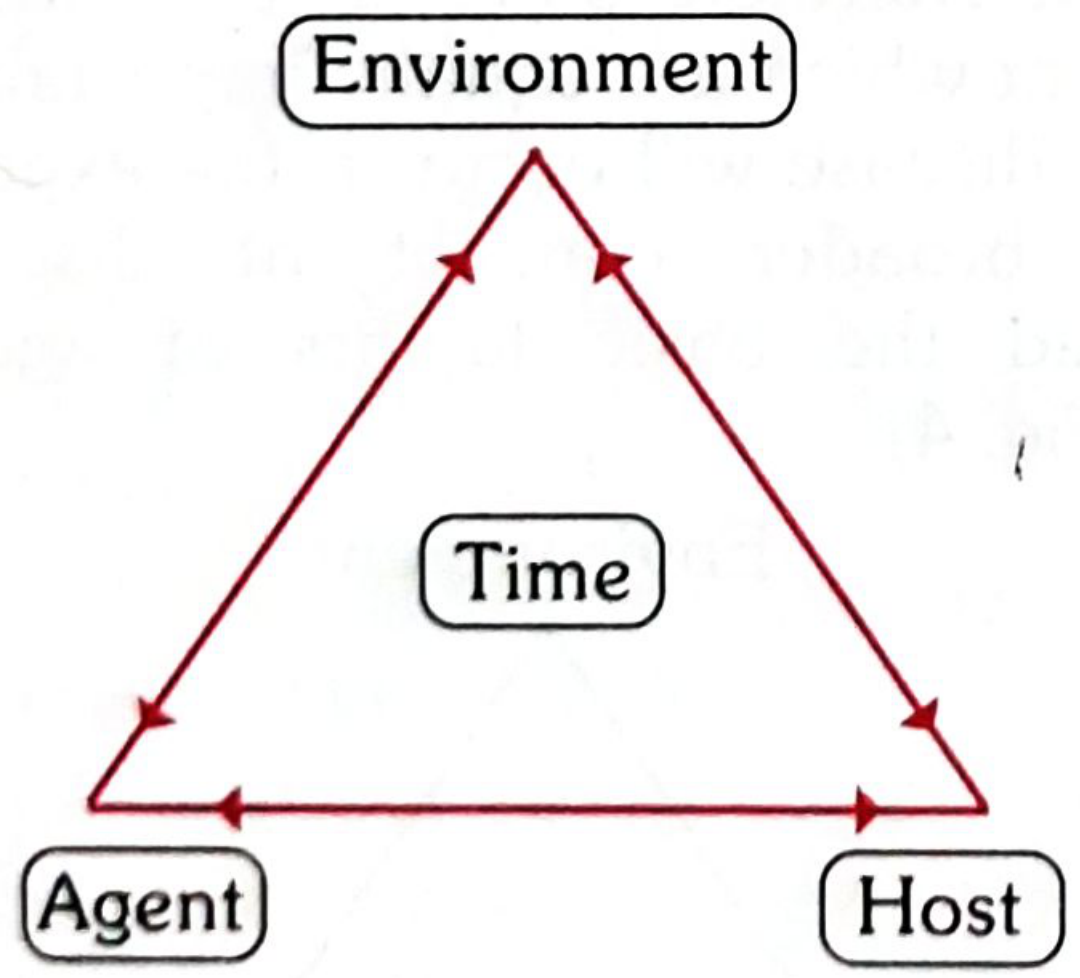
- Agent = cause of disease
- Host = the organism harbouring the disease
- Environment = surroundings/conditions external to the host that cause or permit disease transmission
- Time = accounts for incubation periods, life expectancy of pathogen/host, and duration of illness
The primary mission of epidemiology is to break one of the legs of the triangle, thereby disrupting the connection and stopping an outbreak.
Epidemiologic Concept of Interaction (Venn Diagram)
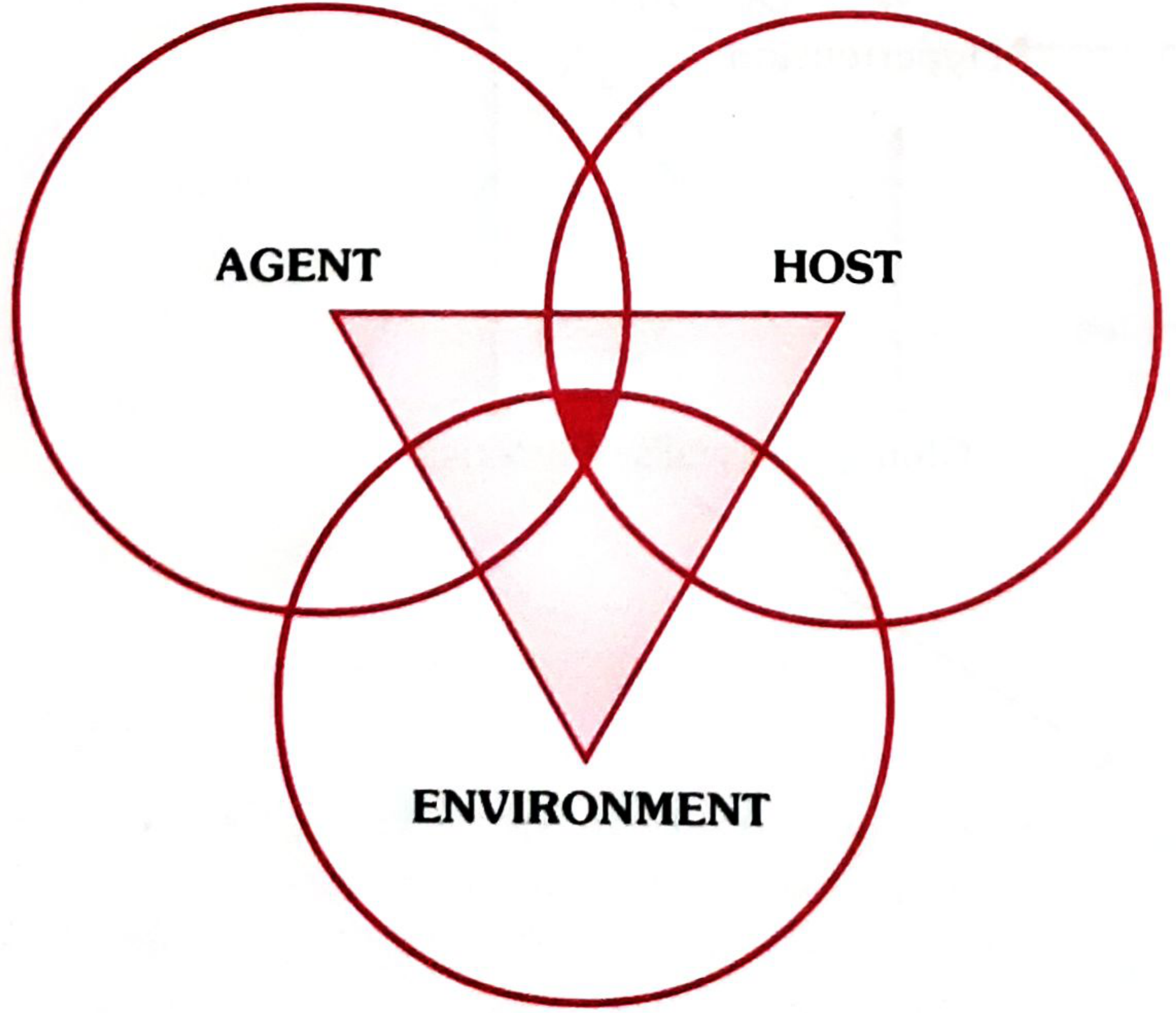
The mere presence of agent, host, and favourable environmental factors is not sufficient to start disease. What is required is an interaction of all three factors. Their combined operation determines:
- The onset of disease (single case to epidemic)
- The distribution of disease in the community
The darkened central area (overlap of all three circles) represents the disease process itself.
1. AGENT FACTORS
The disease agent is defined as "a substance, living or non-living, or a force, tangible or intangible, the excessive presence or relative lack of which may initiate or perpetuate a disease process."
| Category | Examples |
|---|---|
| Biological | Viruses, bacteria, rickettsiae, fungi, protozoa, metazoa |
| Nutrient | Proteins, fats, carbohydrates, vitamins, minerals, water (excess or deficiency) |
| Physical | Heat, cold, humidity, pressure, radiation, electricity, sound |
| Chemical (endogenous) | Urea (uraemia), bilirubin (jaundice), uric acid (gout), ketones |
| Chemical (exogenous) | Allergens, metals, fumes, dust, gases, insecticides |
| Mechanical | Chronic friction, crushing, tearing forces |
| Absence/excess of a factor | Hormones (insulin), enzymes, chromosomal factors (Down syndrome), immunological factors |
| Social agents | Poverty, smoking, drug/alcohol abuse, unhealthy lifestyle, social isolation |
Key properties of biological agents:
- Infectivity - ability to invade and multiply in a host
- Pathogenicity - ability to induce clinically apparent illness
- Virulence - proportion of clinical cases resulting in severe manifestations (measured by case fatality rate)
2. HOST FACTORS (Intrinsic)
The human host is referred to as "soil" and the agent as "seed" in epidemiological terminology.
| Category | Factors |
|---|---|
| Demographic | Age, sex, ethnicity |
| Biological | Genetic makeup, blood groups, blood cholesterol, immunological status, organ function |
| Social & Economic | Socioeconomic status, education, occupation, stress, marital status, housing |
| Lifestyle | Personality, nutrition, physical activity, alcohol, smoking, behavioral patterns |
The host's reaction to an agent is not always predictable - infection may be clinical or subclinical, typical or atypical, and the host may become a carrier (as in diphtheria and hepatitis B).
3. ENVIRONMENTAL FACTORS (Extrinsic)
Defined as "all that which is external to the individual human host, living and non-living, and with which he is in constant interaction."
a. Physical Environment
Non-living things and physical factors: air, water, soil, housing, climate, geography, heat, light, noise, radiation. Man has altered his physical environment to his advantage but in doing so has created new hazards - air pollution, water pollution, noise pollution, radiation hazards.
b. Biological Environment
The universe of living things surrounding man: viruses, microbial agents, insects, rodents, animals, plants. These act as disease-producing agents, reservoirs, intermediate hosts, or vectors. Disruption of the normal harmonious inter-relationship results in ill-health.
c. Psychosocial Environment
Cultural values, customs, habits, beliefs, attitudes, morals, religion, education, lifestyles, community life, health services. Psychosocial stress (poverty, unemployment, bereavement, migration) can lead to psychosomatic disorders including duodenal ulcer, bronchial asthma, hypertension, and coronary heart disease.
Prepathogenesis vs. Pathogenesis
| Phase | Description |
|---|---|
| Prepathogenesis | Agent has not yet entered the host; all three triad factors are present but interacting in the environment. The host is "exposed to the risk of disease." |
| Pathogenesis | Begins with entry of the agent into the susceptible host; agent multiplies, induces tissue/physiological changes; progresses through incubation, then early and late pathogenesis; ends in recovery, disability, or death. |
Limitations and Evolution
The epidemiological triad worked well for infectious diseases but was insufficient for chronic diseases (coronary heart disease, cancer) where:
- A single agent is often not identifiable
- Multiple factors interact in complex ways
- Social, genetic, behavioral, and lifestyle factors are paramount
This led to two updated models:
-
Web of Causation (MacMahon & Pugh) - considers all predisposing factors and their complex interrelationships; best illustrated by the causal web of myocardial infarction.
-
Advanced Triangle - replaces "Agent" with "Causative factors" and adds behaviour, lifestyle, ecologic elements, and chronic disease considerations.
The core public health implication remains the same: breaking even one leg of the triangle can disrupt disease transmission and stop an outbreak.
Source: Park's Textbook of Preventive and Social Medicine, pp. 44-49
This is a shared conversation. Sign in to Orris to start your own chat.