Lung abscess* - etiology* and morphology; clinical features 2. Lung Carcinoma* - histologic classification, clinical presentations, Small Cell Carcinoma - morphology 3. Pathogenesis of Emphysema*; Gross, Microscopic features 4. Bronchiectasis* - morphology, complications, gross, microscopic features 5. Lobar Pneumonia - stages, microscopy, gross of each stage 1. Lung Tumors - WHO classification, etiopathogenesis, morphology 2. Lobar Pneumonia - etiopathogenesis, gross, microscopic features, complications answer in detail covering imp points as welll in exaam point of view 2mbbs pathology refer harsh moham add diagrams as well cover required points for muhs
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive, exam-oriented answer covering all your topics for 2nd MBBS Pathology (MUHS), based on Robbins Pathology (the standard reference aligned with Harsh Mohan):
2nd MBBS Pathology - Respiratory System (MUHS Exam Notes)
PART 1: LUNG ABSCESS
Definition
A lung abscess is a localized area of suppuration within the pulmonary parenchyma resulting in the formation of one or more large cavities.
Etiology (IMPORTANT)
| Mechanism | Examples |
|---|---|
| Aspiration (most common) | Carious teeth, infected sinuses/tonsils; occurs during anesthesia, coma, alcoholic intoxication, debilitation |
| Aspiration of gastric contents | Plus oropharyngeal organisms |
| Complication of necrotizing pneumonia | S. aureus, Streptococcus pyogenes, K. pneumoniae, Pseudomonas, type 3 pneumococcus |
| Bronchial obstruction | Lung carcinoma (10-15% of abscesses) - obstruction, distal atelectasis |
| Septic embolism | From infective endocarditis of right heart, thrombophlebitis |
| Hematogenous spread | Staphylococcal bacteremia - multiple abscesses |
| Fungi/parasites mimicking abscess | Aspergillus, Cryptococcus, Histoplasma, TB, Entamoeba histolytica, Echinococcus |
| Primary cryptogenic | No identifiable cause |
Key exam point: Anaerobic bacteria are present in almost ALL lung abscesses, and are the exclusive isolates in 1/3 to 2/3 of cases. Most common anaerobes: Prevotella, Fusobacterium, Bacteroides, Peptostreptococcus.
Morphology
Gross:
- Abscesses range from few mm to 5-6 cm in diameter
- Location depends on cause:
- Aspiration-related: More common on the right side (more vertical right main bronchus), usually single; posterior segment RUL and apical segment of RLL
- Pneumonia/bronchiectasis-related: Multiple, basal, diffusely scattered
- Septic emboli: Multiple, any region
- As abscess enlarges, it ruptures into airways → partial drainage → air-fluid level on X-ray (pathognomonic)
- Chronic cases: Fibrous wall formation (fibrous capsule)
Microscopic:
- Suppurative (neutrophilic) destruction of lung parenchyma - central area of cavitation
- Central cavity filled with suppurative debris
- If communication with airway: air-containing cavity
- Superimposed saprophytic infections within necrotic debris
- Gangrene of the lung: Large, poorly demarcated, fetid, green-black, multilocular cavities
- Chronic abscess: Fibrous wall (fibroblastic proliferation)
Clinical Features
- Cough, fever, copious amounts of foul-smelling purulent/sanguineous sputum
- Chest pain, weight loss
- Clubbing of fingers and toes
- Diagnosis confirmed by radiology (air-fluid level on CXR/CT)
- Always rule out underlying carcinoma in older patients
Complications
- Extension into pleural cavity (empyema)
- Hemorrhage
- Brain abscess or meningitis (septic emboli)
- Secondary amyloidosis (type AA) - rare
PART 2: LUNG CARCINOMA
Histologic Classification (WHO)
LUNG CARCINOMA
├── NON-SMALL CELL LUNG CARCINOMA (NSCLC) ~85%
│ ├── Adenocarcinoma (most common, ~40%)
│ ├── Squamous Cell Carcinoma (~25-30%)
│ └── Large Cell Carcinoma (~10-15%)
└── SMALL CELL LUNG CARCINOMA (SCLC) ~15%
| Feature | Adenocarcinoma | Squamous Cell Ca | Small Cell Ca |
|---|---|---|---|
| Location | Peripheral | Central/hilar | Central |
| Smoking association | Less (also in non-smokers) | Strong | Very strong |
| Precursor | AAH, AIS, MIA | Squamous dysplasia/CIS | None well-defined |
| Mutations | EGFR, ALK, KRAS | TP53, SOX2 | TP53, RB |
| Hormone syndromes | - | PTHrP (hypercalcemia) | ACTH, ADH (SIADH) |
Etiopathogenesis
-
Tobacco Smoking (most important): ~80% of lung cancers occur in active/recent smokers. Risk is 60 times greater in heavy smokers (2 packs/day x 20 years). Only 10-15% of smokers develop lung cancer - suggesting genetic susceptibility.
-
Industrial Hazards: Asbestos (synergistic with smoking), arsenic, chromium, uranium, nickel, vinyl chloride, mustard gas, ionizing radiation
-
Air Pollution: Radon gas (radioactive decay product of radium) - particularly important in miners
-
Molecular Pathogenesis:
- Multiple genetic mutations required (multi-step carcinogenesis)
- Proto-oncogenes: KRAS, EGFR, MYC, ALK
- Tumor suppressor loss: TP53, RB, p16
- High mutation burden from tobacco carcinogens → tumor neoantigens → responsive to immune checkpoint inhibitors (PD-1/PD-L1)
-
Squamous metaplasia → dysplasia → carcinoma in situ → invasive cancer (best documented pathway, especially for SCC)
Clinical Presentations
- Local effects: Cough, hemoptysis, chest pain, wheezing (endobronchial lesion)
- Obstructive pneumonitis (post-obstructive pneumonia)
- Superior vena cava syndrome - SVC obstruction → facial edema, arm swelling
- Pancoast tumor (superior sulcus) - shoulder pain, Horner syndrome (ptosis, miosis, anhidrosis)
- Pleural effusion (malignant)
- Hoarseness - recurrent laryngeal nerve involvement
- Paraneoplastic syndromes (IMPORTANT for exams):
| Syndrome | Carcinoma Type |
|---|---|
| SIADH (hyponatremia) | Small Cell |
| Ectopic ACTH (Cushing's) | Small Cell |
| Hypercalcemia (PTHrP) | Squamous Cell |
| Lambert-Eaton myasthenic syndrome | Small Cell |
| Hypertrophic osteoarthropathy/clubbing | Adenocarcinoma |
Small Cell Carcinoma - Morphology
- Most aggressive lung cancer; almost always metastatic at presentation
- Arises centrally from bronchial mucosa
Gross:
- Central/perihilar mass, often with bulky lymph node involvement at diagnosis
- White-tan, soft, friable tumor
- Frequently causes compression of bronchi and vascular structures
Microscopic (KEY):
- Small cells (about the size of 2-3 lymphocytes)
- "Oat cell" appearance - scant cytoplasm, round-to-oval nuclei, finely granular chromatin ("salt and pepper"), absent/inconspicuous nucleoli
- Cells arranged in sheets, nests, ribbons
- Nuclear molding (nuclei indent each other)
- High mitotic rate, abundant necrosis, apoptotic debris ("nuclear streaming")
- Neuroendocrine differentiation - cells contain dense-core neurosecretory granules on electron microscopy
- IHC: Positive for CD56, synaptophysin, chromogranin, NSE (neuroendocrine markers)
- Strongly associated with TP53 and RB mutations
PART 3: PATHOGENESIS OF EMPHYSEMA
Definition
Irreversible enlargement of airspaces distal to the terminal bronchiole, accompanied by destruction of alveolar walls without significant fibrosis.
Types (Exam Diagram)
TERMINAL BRONCHIOLE
|
┌────────────┴────────────┐
│ │
RESPIRATORY BRONCHIOLE ALVEOLAR DUCT
│ │
ALVEOLI ALVEOLI
Centriacinar: Central/proximal part affected (respiratory bronchiole) - MOST COMMON
Panacinar: Entire acinus from respiratory bronchiole to alveolus - α1-AT deficiency
Paraseptal: Distal alveoli near pleura/septa - spontaneous pneumothorax in young
Irregular: Paracicatricial, near scars - clinically insignificant
Pathogenesis (PROTEASE-ANTIPROTEASE + OXIDATIVE STRESS)
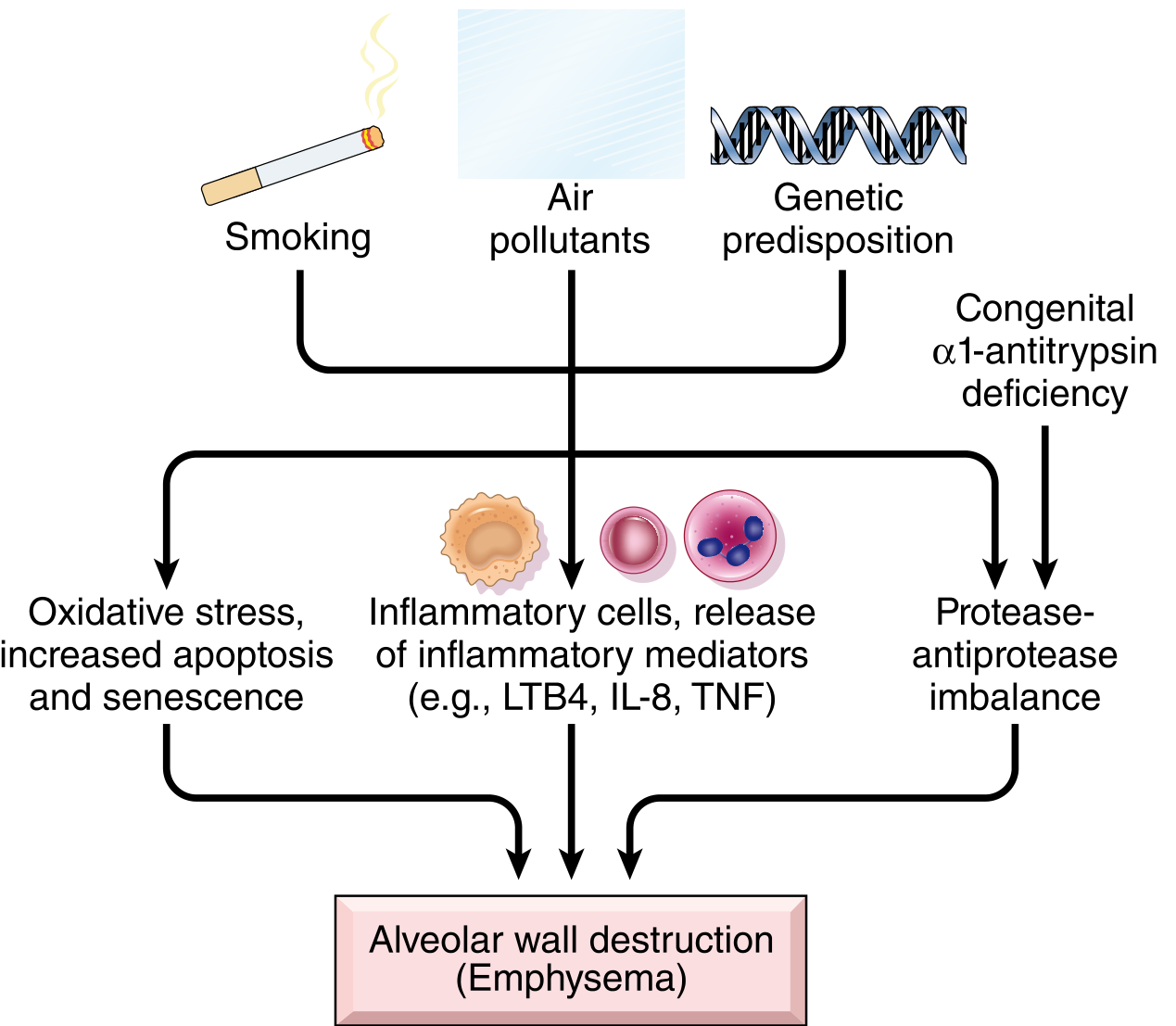
Three main mechanisms:
1. Protease-Antiprotease Imbalance
- Tobacco smoke stimulates macrophages and neutrophils in alveoli
- These inflammatory cells release elastase and other proteases (MMPs, cathepsins)
- Proteases break down elastin, collagen in alveolar walls
- Normally, α1-antitrypsin (α1-AT) inhibits neutrophil elastase
- In smokers: Oxidants from smoke inactivate α1-AT → relative deficiency
- Hereditary α1-AT deficiency (Pi locus, chromosome 14, ZZ phenotype) - causes panacinar emphysema at younger age; affects lower lobes
2. Oxidative Stress
- Cigarette smoke contains reactive oxygen species (ROS)
- ROS also released from activated macrophages/neutrophils
- Causes direct tissue damage, endothelial dysfunction, inflammation
- Inactivates antiproteases → compounds protease-antiprotease imbalance
- NRF2 normally protects cells from oxidant damage; genetic variants in NRF2 increase susceptibility
3. Inflammatory Mediators
- Mediators released: LTB4, IL-8, TNF
- Attract more inflammatory cells (perpetuating cycle)
- Lead to T and B cell accumulation in affected lung
4. Infection
- Not initiating, but bacterial/viral infections cause acute exacerbations
Gross Features of Emphysema
| Type | Gross Appearance |
|---|---|
| Panacinar | Pale, voluminous lungs; often obscure the heart at autopsy; lower zones predominantly affected |
| Centriacinar | Less impressive grossly; deeper pink, less voluminous; upper 2/3 more affected; only late stage shows gross changes |
| Bullous | Large subpleural blebs/bullae (>1 cm), especially near apex |
Microscopic Features
- Destruction of alveolar walls without fibrosis - key distinguishing feature
- Enlarged air spaces
- Reduced number of alveolar capillaries
- Deformed terminal/respiratory bronchioles (loss of supporting septa)
- Bronchiolar inflammation and submucosal fibrosis in advanced disease
- "Pink Puffer" presentation: Barrel chest, pursed-lip breathing, hyperinflated lungs on CXR, relatively normal blood gases
PART 4: BRONCHIECTASIS
Definition
Permanent, abnormal dilatation of the bronchi and bronchioles due to destruction of the muscle and elastic tissue of their walls, usually caused by or associated with chronic necrotizing infections.
Etiology/Pathogenesis
Obstructive causes:
- Tumors, foreign bodies, mucus impaction
Post-infectious (most common):
- Necrotizing/destructive infections: Bacterial (S. aureus, Klebsiella, anaerobes), TB, viral (adenovirus, influenza), fungal
Congenital/hereditary:
- Cystic fibrosis (most common cause in Western countries)
- Kartagener syndrome (immotile cilia/Primary Ciliary Dyskinesia) - bronchiectasis + situs inversus + sinusitis
- Williams-Campbell syndrome (bronchial cartilage deficiency)
- Mounier-Kuhn syndrome (tracheobronchomegaly)
Immunodeficiency states:
- Hypogammaglobulinemia, HIV, post-transplant
Inflammatory disorders:
- Rheumatoid arthritis, IBD, allergic bronchopulmonary aspergillosis (ABPA)
Morphology
Gross Features
- Most commonly involves the lower lobes bilaterally (dependent portions where secretions pool)
- Bronchi are dilated (up to 4x normal diameter), extend to within 1-2 cm of pleural surface
- Three patterns:
- Cylindrical (tubular) - uniform dilation, most common
- Varicose - irregular, bead-like dilation
- Saccular (cystic) - progressive cystic ballooning, most severe
- Cut surface: Dilated airways filled with purulent mucopurulent material
- Lung parenchyma around the bronchi shows fibrosis and consolidation
- Pleura may be thickened and adherent
Microscopic Features
- Inflammatory exudate in the bronchial lumen (neutrophils, pus)
- Destruction and replacement of all layers of bronchial wall with fibrous tissue
- Loss of bronchial mucous glands and cartilage
- Squamous metaplasia of bronchial epithelium
- Vascular changes: Enlargement of bronchial arteries, arteriovenous anastomoses (explains hemoptysis)
- Surrounding alveolar parenchyma: Fibrosis, organizing pneumonia
- Mucus gland hypertrophy
Clinical Features
- "Wet lung disease"
- Copious purulent sputum (3-layer if allowed to settle: frothy top, mucopurulent middle, pus sediment)
- Hemoptysis (due to enlarged bronchial vessels)
- Recurrent respiratory infections
- Dyspnea, cough
- Clubbing of fingers - classic finding
Complications
- Cor pulmonale (right heart failure due to pulmonary hypertension from hypoxia)
- Empyema and pyopneumothorax
- Metastatic brain abscess and meningitis
- Secondary amyloidosis (AA amyloidosis) - from chronic infection
- Right-sided heart failure (cor pulmonale)
- Respiratory failure
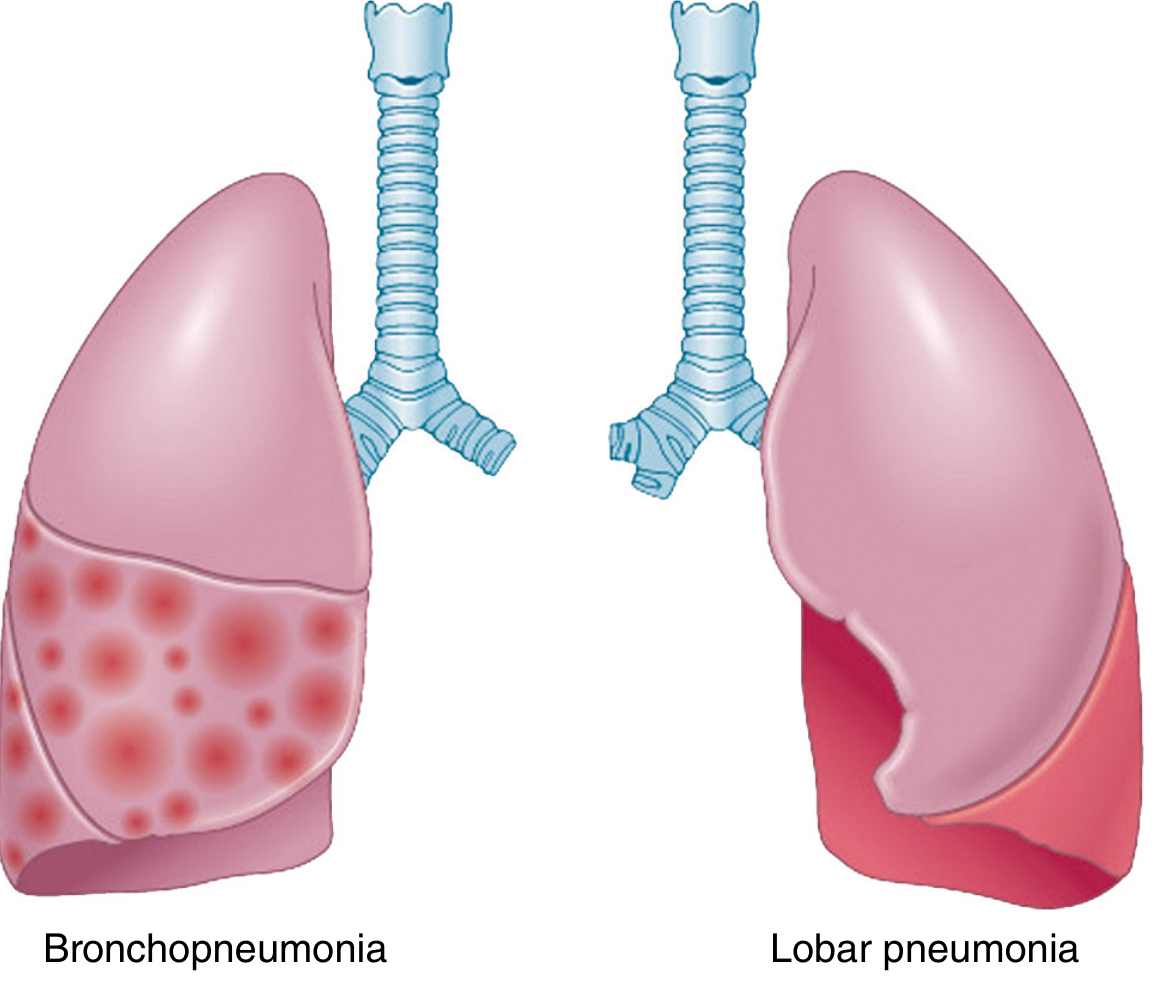
PART 5: LOBAR PNEUMONIA
Definition
Consolidation of all or most of an entire lobe of the lung.
Etiopathogenesis
Most common cause: Streptococcus pneumoniae (pneumococcus) (95% of cases)
- Gram-positive diplococci
- Other causes: Klebsiella pneumoniae (alcoholics - "currant jelly sputum"), S. aureus, Legionella, H. influenzae
Pathogenesis:
- Organisms reach alveoli via inhalation or aspiration
- Encounter alveolar macrophages (first defense)
- If overwhelmed - organisms multiply in alveoli
- Organism + complement activation → cytokine release (IL-1, TNF, IL-8)
- Outpouring of edema fluid into alveoli (Stage 1 - Congestion)
- Massive neutrophil influx (Stages 2 and 3)
- Resolution (macrophage clearance) - Stage 4
Stages of Lobar Pneumonia - Classic Four Stages
Stage 1: Congestion (Days 1-2)
Gross:
- Lung is heavy, wet, and red
- Increased weight, congested, boggy
Microscopic:
- Vascular engorgement - dilated, engorged capillaries
- Intra-alveolar serous/watery edema fluid (protein-rich exudate)
- Few neutrophils
- Numerous bacteria (numerous cocci visible in alveoli)
- Alveolar septa intact
Stage 2: Red Hepatization (Days 3-4)
Gross:
- Lobe is red, firm, and airless
- Cut surface resembles liver (hepatization = liver-like consistency)
- Pleural surface may show fibrinous exudate
Microscopic:
- Massive confluent exudation
- Alveoli packed with: Neutrophils + Red Blood Cells + Fibrin strands
- Fibrin strands pass through pores of Kohn between alveoli
- Alveolar capillaries compressed by exudate
- No air in alveoli
Stage 3: Gray Hepatization (Days 5-7)
Gross:
- Lobe is gray-brown, firm, dry (less congested than Stage 2)
- Still liver-like consistency but color changes to gray
Microscopic:
- Progressive disintegration/lysis of RBCs (hence gray color - less hemoglobin)
- Fibrinopurulent exudate persists - alveoli filled with fibrin and pus (neutrophils undergoing degeneration)
- Macrophages begin to appear
- Fibrin strands prominent
- Capillaries still compressed
Stage 4: Resolution (Days 7-10 onwards)
Gross:
- Lung returns toward normal appearance
- Softening and granular texture as exudate liquefies
Microscopic:
- Enzymatic digestion of the exudate by macrophages and enzymatic activity
- Production of granular, semifluid debris
- Debris is resorbed, ingested by macrophages, or expectorated
- Fibrinous exudate may be organized by fibroblasts (→ fibrous scar = "carnification" if resolution fails)
- Macrophages are the dominant cell
Key exam memory: "Congestion → Red → Gray → Resolution" (CGR mnemonic)
Clinical Features
- Abrupt onset of high fever, shaking chills
- Cough with rusty (rust-colored) sputum - characteristic of pneumococcal pneumonia (from RBC breakdown in alveoli)
- Pleuritic chest pain (pleuritis/friction rub when pneumonia reaches lung surface)
- Dyspnea, tachypnea
- Dullness to percussion over affected lobe
- Bronchial breathing, increased tactile fremitus
- Herpes labialis may appear
- Resolution with antibiotics in 8-10 days
Complications
- Abscess formation (tissue destruction/necrosis)
- Empyema - spread to pleural cavity (fibrinopurulent pleurisy)
- Bacteremia/sepsis - spread to heart valves (endocarditis), brain (meningitis, brain abscess), joints (septic arthritis), kidneys (abscess), spleen
- Organizing pneumonia (carnification) - failure of resolution → fibroblast invasion → fibrous scar in lung
- Fibrous pleuritis - fibrous thickening or permanent pleural adhesions
PART 6: LUNG TUMORS - WHO CLASSIFICATION & ETIOPATHOGENESIS
WHO Classification of Lung Tumors (2021)
MALIGNANT EPITHELIAL TUMORS
├── Adenocarcinoma
│ ├── Atypical Adenomatous Hyperplasia (AAH) - precursor
│ ├── Adenocarcinoma in Situ (AIS, ≤3cm)
│ ├── Minimally Invasive Adenocarcinoma (MIA)
│ └── Invasive Adenocarcinoma
│ ├── Lepidic predominant
│ ├── Acinar predominant
│ ├── Papillary predominant
│ ├── Micropapillary predominant
│ └── Solid predominant
├── Squamous Cell Carcinoma
│ ├── Keratinizing
│ ├── Non-keratinizing
│ └── Basaloid
├── Large Cell Carcinoma
├── Adenosquamous Carcinoma
├── Sarcomatoid Carcinomas
└── NEUROENDOCRINE TUMORS
├── Small Cell Carcinoma
├── Large Cell Neuroendocrine Carcinoma
├── Typical Carcinoid
└── Atypical Carcinoid
Etiopathogenesis
1. Tobacco Smoking:
- Most important carcinogen; ~80% of all lung cancers
- Risk: 60x higher in heavy smokers (2 packs/day x 20 years)
- Carcinogens in smoke include polycyclic hydrocarbons, nitrosamines, benzene
- Activated by P-450 monooxygenase system → reactive carcinogens → DNA damage
- Causes a stepwise progression: normal → basal cell hyperplasia → squamous metaplasia → dysplasia → CIS → invasive cancer
2. Environmental/Industrial:
- Asbestos (especially + smoking = synergistic effect; also causes mesothelioma)
- Radon gas, arsenic, chromium, nickel, uranium
3. Molecular Mutations (IMPORTANT):
| Mutation | Tumor Type | Clinical Significance |
|---|---|---|
| KRAS | Adenocarcinoma | Poor prognosis, no targeted therapy |
| EGFR | Adenocarcinoma (non-smokers, females, Asians) | Gefitinib/Erlotinib targeted therapy |
| ALK rearrangement | Adenocarcinoma (young non-smokers) | Crizotinib targeted therapy |
| TP53 | All types (especially SCLC, SCC) | Most common mutation in lung cancer |
| RB deletion | Small Cell Ca | Loss of cell cycle control |
| MYC amplification | Small Cell Ca | Drives rapid proliferation |
| PD-L1 expression | NSCLC | Immunotherapy target (pembrolizumab) |
Morphology of Major Types
Adenocarcinoma
- Peripheral subpleural location (most common location for adenocarcinoma)
- Gross: Grayish-white mass, may show central scar (desmoplasia); mucin production gives gelatinous areas
- Micro: Glandular/acinar/papillary architecture; mucin-secreting columnar cells; lepidic pattern = tumor cells growing along alveolar walls without invasion
- Bronchioloalveolar (lepidic) pattern: Distinct - pneumonia-like consolidation on imaging
Squamous Cell Carcinoma
- Central location - arises at or near the hilus from main/lobar bronchi
- Gross: Gray-white hilar mass with cavitation (central necrosis is common), firm
- Micro: Sheets of polygonal cells with: intercellular bridges, keratin pearls, individual cell keratinization; marked pleomorphism; dysplastic changes in adjacent epithelium
Large Cell Carcinoma
- Undifferentiated (no squamous/glandular/NE features)
- Peripheral location
- Micro: Large cells with prominent nucleoli, abundant cytoplasm; no differentiation markers
- Diagnosis of exclusion
SUMMARY TABLE - HIGH-YIELD EXAM POINTS
| Topic | Key Exam Points |
|---|---|
| Lung Abscess | Anaerobes present in ALL; right-sided aspiration abscesses; rule out carcinoma in elderly; foul-smelling sputum |
| Emphysema | Protease-antiprotease + oxidative stress; centriacinar = smokers; panacinar = α1-AT deficiency; no fibrosis on micro |
| Bronchiectasis | Permanent dilation; cylindrical > varicose > saccular; 3-layer sputum; complications = cor pulmonale, amyloidosis |
| Lobar Pneumonia | S. pneumoniae; 4 stages; rusty sputum; complications = empyema, abscess, bacteremia |
| Lung Ca | NSCLC 85% vs SCLC 15%; Adenocarcinoma = most common; SCC = central + cavitates + hypercalcemia; SCLC = oat cells + paraneoplastic |
MUHS Exam Tip: For morphology questions, always describe both gross AND microscopic. For lobar pneumonia, draw a table of the 4 stages. For emphysema, draw the protease-antiprotease diagram. For lung carcinoma, memorize the paraneoplastic syndromes table.
Sources: Robbins & Kumar Basic Pathology (10th ed.) and Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.) - content equivalent to Harsh Mohan Textbook of Pathology for 2nd MBBS curriculum.
This is a shared conversation. Sign in to Orris to start your own chat.