What is pulmonary embolism
Reading File
Finding Sources
Searching PubMed
"pulmonary embolism"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive coverage across definition, pathophysiology, symptoms, vital signs, physical exam, diagnostics, risk stratification, and treatment. I can now deliver a thorough answer.
Pulmonary Embolism (PE)
Definition
Pulmonary embolism is a blockage of one or more pulmonary arteries, most commonly caused by a blood clot that has traveled from the deep veins of the lower extremities (deep vein thrombosis, or DVT). It is a life-threatening manifestation of venous thromboembolism (VTE) and a major cause of cardiovascular mortality. - Rosen's Emergency Medicine, 9e
Pathophysiology
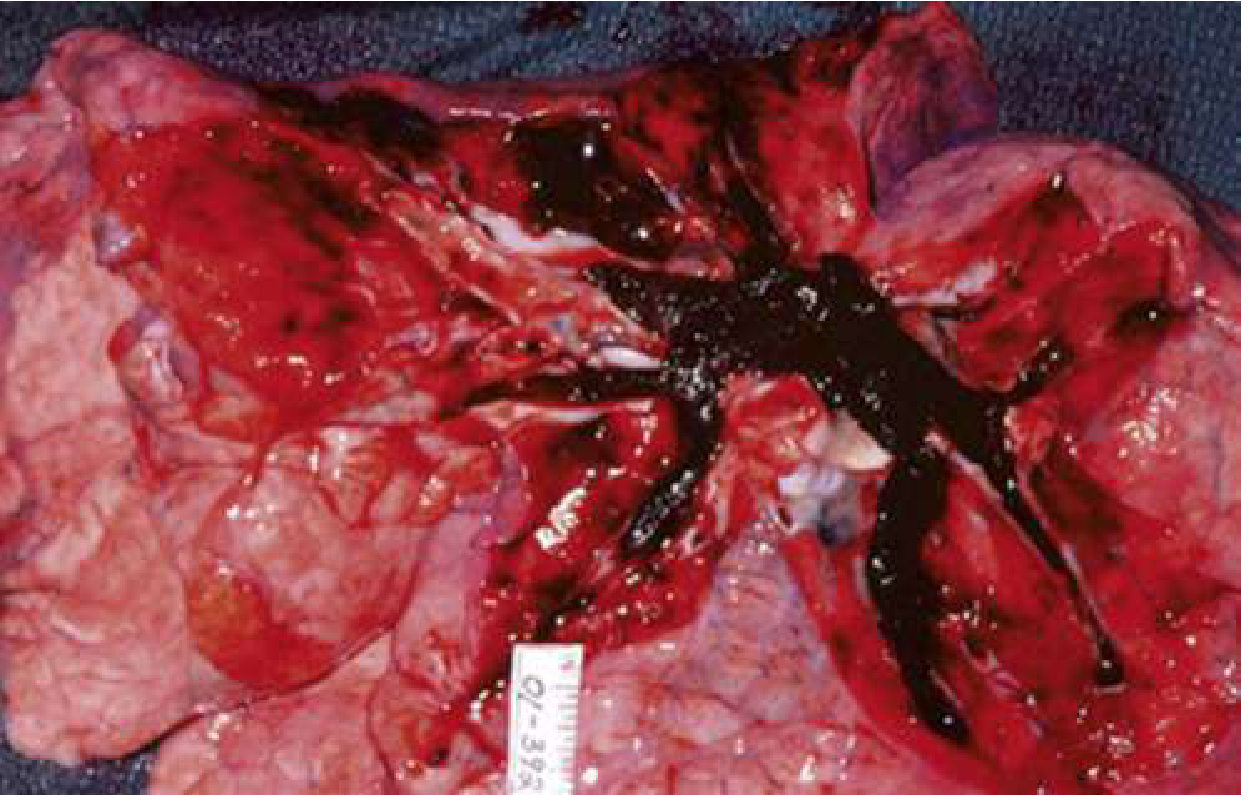
A clot from the deep venous system detaches and travels through the right side of the heart into the pulmonary circulation. This causes:
- Mechanical obstruction of blood flow, increasing right ventricular (RV) afterload
- RV pressure overload - the RV dilates and pushes the interventricular septum leftward, compressing the LV
- Reduced LV filling leading to decreased cardiac output, hypotension, and poor coronary perfusion - creating a spiral of cardiac failure
- Hypoxemia from ventilation-perfusion (V/Q) mismatch: areas of the lung are ventilated but not perfused
- In the most extreme cases, the entire right ventricular outflow system becomes occluded, causing cardiac arrest
Approximately 25% of sudden cardiac deaths are thought to be due to PE. - Rosen's Emergency Medicine, p.1202
Risk Factors (Virchow's Triad)
| Category | Examples |
|---|---|
| Hypercoagulability | Factor V Leiden, prothrombin G20210A, protein C/S/antithrombin deficiency, antiphospholipid syndrome, cancer, oral contraceptives |
| Venous stasis | Prolonged immobilization, long-distance travel, hospitalization, paralysis |
| Endothelial injury | Surgery (especially orthopedic/pelvic), trauma, indwelling catheters |
Additional high-risk conditions: obesity, pregnancy, age >35, prior VTE, malignancy.
Clinical Presentation
Symptoms
The presentation ranges from completely asymptomatic to sudden cardiovascular collapse.
- Dyspnea - most common symptom (75-80% of patients); can be constant, intermittent, or only with exertion. May be described as fatigue or "can't take a full breath"
- Chest pain - second most common; often pleuritic (sharp, worsens with breathing), but may be dull or vague. Absent in up to one-third of patients
- Hemoptysis - when PE causes pulmonary infarction
- Syncope - present in <5% of PE cases, but unexplained syncope in a patient with risk factors should raise suspicion
- Unilateral leg swelling - present in fewer than 30% of patients, but relatively specific when combined with dyspnea or chest pain
Important: No single symptom confirms or rules out PE. Even dyspnea - the most common symptom - is absent in nearly 1 in 4 patients with confirmed PE.
Vital Signs
| Finding | Frequency | Significance |
|---|---|---|
| Tachycardia (HR >100) | ~50% | Associated with more severe PE and worse prognosis |
| Elevated respiratory rate (>20) | ~50% | Non-specific |
| Hypotension (SBP <90 mmHg) | ~10% | Most important predictor of mortality - 4-fold increase in death risk |
| Hypoxemia (SpO2 <95%) | ~50% | A normal saturation does NOT rule out PE |
Rosen's Emergency Medicine, p.1202-1203
Physical Examination
Most patients have no obvious abnormality. The only finding that reliably increases PE probability is evidence of DVT (unilateral leg asymmetry, edema, or deep vein tenderness). Wheezing suggests bronchospasm (alternative diagnosis); bilateral rales suggest heart failure.
Diagnosis
Step 1: Pre-test Probability (PTP)
Clinical gestalt or validated scoring tools are used first.
Wells Score for PE:
| Clinical Feature | Points |
|---|---|
| Previous PE or DVT | 1.5 |
| Heart rate >100 bpm | 1.5 |
| Recent surgery or immobilization (within 4 weeks) | 1.5 |
| Clinical signs of DVT | 3 |
| Hemoptysis | 1 |
| Active cancer | 1 |
| Alternative diagnosis less likely than PE | 3 |
- Score <2 = Low probability
- Score 2-6 = Intermediate
- Score >6 = High probability
Rosen's Emergency Medicine, p.1204
Step 2: D-Dimer
- Sensitivity: 95-98%; Specificity: 40-55% - it is a good rule-out test but not a rule-in test
- In patients with non-high PTP (Wells <6), a negative D-dimer effectively excludes PE (NPV 99-100%)
- Age-adjusted threshold: Age × 10 ng/mL (for labs with standard 500 ng/mL cutoff) - increases the proportion of elderly patients who can skip imaging by 10-20%
- False positives occur with infection, malignancy, surgery, pregnancy, and many other conditions
- False negatives can occur with subacute/chronic PE, lipemia, or warfarin therapy
Step 3: Imaging
CT Pulmonary Angiography (CTPA) - gold standard, most widely used
- Visualizes clots directly in pulmonary arteries
- Also detects alternative diagnoses
- Preferred first-line imaging in most settings
Ventilation-Perfusion (V/Q) scan
- Preferred when CTPA is contraindicated (renal insufficiency, contrast allergy)
- Used in pregnancy (lower maternal radiation exposure vs. CTPA)
Bedside Ultrasound
- DVT on compression ultrasound = sufficient to initiate treatment without CTPA
- Point-of-care echo showing RV:LV ratio >1:1 increases suspicion for PE
ECG Findings:
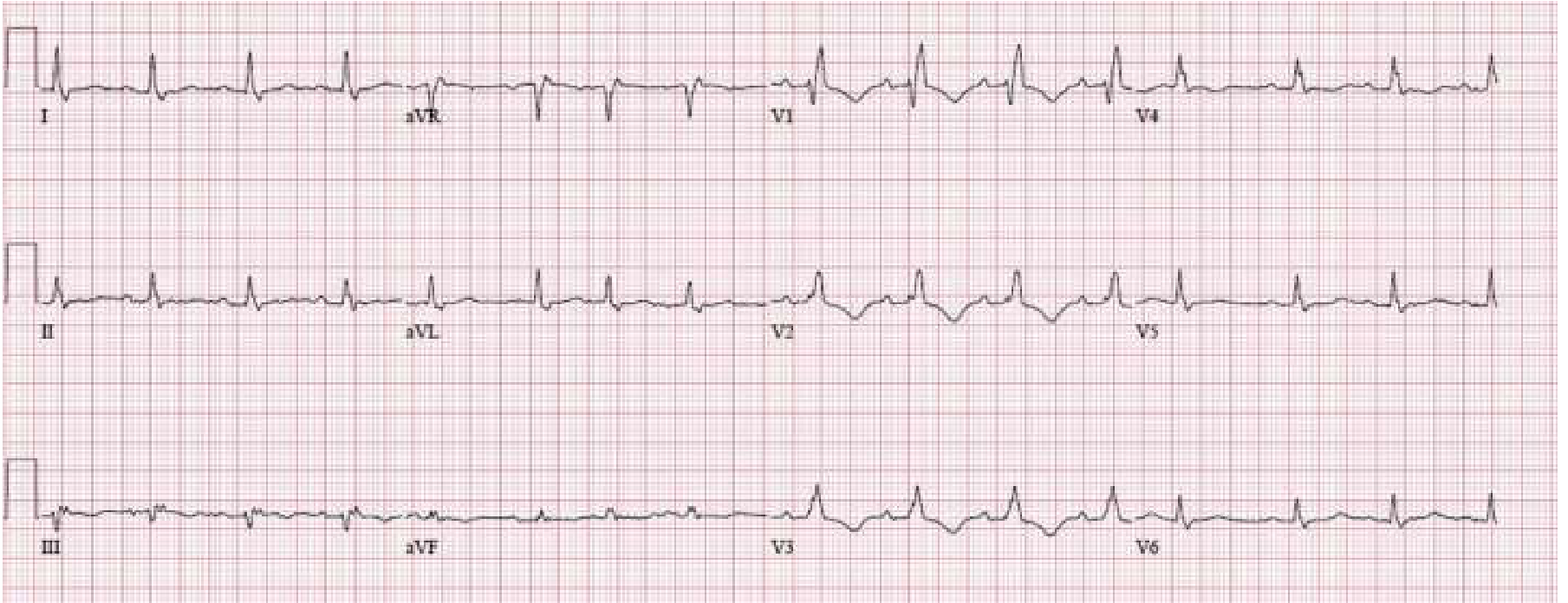
Classic ECG signs of RV strain in PE: S1Q3T3 pattern, T-wave inversions V1-V4, new right bundle branch block. However, the most common ECG finding in PE is simply sinus tachycardia.
Risk Stratification and Treatment
| Risk Category | Criteria | Mortality | Management |
|---|---|---|---|
| Low-risk | Hemodynamically stable, no RV dysfunction | <1-3% | Anticoagulation (DOAC preferred); may discharge home |
| Intermediate-risk | Stable but RV dysfunction on echo/CTPA and/or elevated troponin/BNP | 3-15% | Anticoagulation; monitored admission; consider PERT; thrombolysis in select cases |
| High-risk (Massive) | Hemodynamically unstable (SBP <90) | 15-50% | Heparin + systemic thrombolysis (tPA) or surgical/catheter-directed thromboembolectomy; ICU admission |
Rosen's Emergency Medicine, p.1208
Anticoagulation
- DOACs (Direct oral anticoagulants) - rivaroxaban or apixaban preferred for most patients (no parenteral bridging needed for apixaban/rivaroxaban in PE)
- Low-molecular-weight heparin (LMWH) - preferred in cancer-associated VTE and pregnancy
- Unfractionated heparin (UFH) - preferred if thrombolysis or surgery is planned (short half-life, reversible)
- Warfarin remains an option for patients who cannot take DOACs
Thrombolysis
- Used in high-risk (massive) PE with hemodynamic instability
- Agent: Alteplase (tPA) 100 mg IV over 2 hours
- Survival rate from PE cardiac arrest is only ~20% even with witnessed arrest and fibrinolysis
- Systemic thrombolysis is contraindicated in recent surgery, stroke, active bleeding
Advanced Therapies
- Catheter-directed thrombolysis (CDT) - delivers lower-dose thrombolytics directly into the clot
- Mechanical thrombectomy - catheter-based clot removal; a 2025 meta-analysis (Singh et al., PMID 40269600) compared mechanical thrombectomy vs. CDT, finding both are viable options for intermediate-high risk PE
- Surgical embolectomy - reserved for massive PE with contraindication to thrombolysis or failed fibrinolysis
- Pulmonary Embolism Response Teams (PERT) - multidisciplinary teams that rapidly coordinate advanced PE care
Airway/Hemodynamic Support
- Supplemental O2 to target SpO2 >90%
- Avoid intubation when possible (positive pressure ventilation reduces preload and can precipitate cardiac arrest)
- For hypotension: small fluid boluses (250-500 mL); avoid aggressive fluid loading which worsens RV distension
- Vasopressors (norepinephrine) for refractory hypotension
Special Populations
Pregnancy: PE is responsible for 15% of maternal deaths in the US. Risk is ~5x higher in pregnancy due to elevated clotting factors (V, VIII, X, vWF), decreased protein S, and venous stasis from uterine IVC compression. LMWH is the anticoagulant of choice throughout pregnancy. The diagnosis is challenging because dyspnea is normal in pregnancy and D-dimer is physiologically elevated. - Murray & Nadel's Respiratory Medicine
Summary
PE is a common, potentially fatal condition caused by clot obstruction of the pulmonary arteries. Its presentation is highly variable - from mild breathlessness to cardiac arrest. Diagnosis is built on pre-test probability assessment, D-dimer testing, and CTPA. Treatment is risk-stratified: anticoagulation for stable patients, thrombolysis or mechanical intervention for unstable patients.
This is a shared conversation. Sign in to Orris to start your own chat.