Focal seizures
Reading File
Finding Sources
Searching PubMed
"focal seizures" classification management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
I now have comprehensive information to write a thorough answer. Let me compile it.
Focal Seizures
Definition
Focal seizures (formerly called partial seizures) arise from a neuronal network either discretely localized within one brain region or more broadly distributed but still within a cerebral hemisphere. The 2017 ILAE classification eliminated the old terms "simple partial" and "complex partial," replacing them with terminology centered on awareness and onset type.
ILAE 2017 Classification
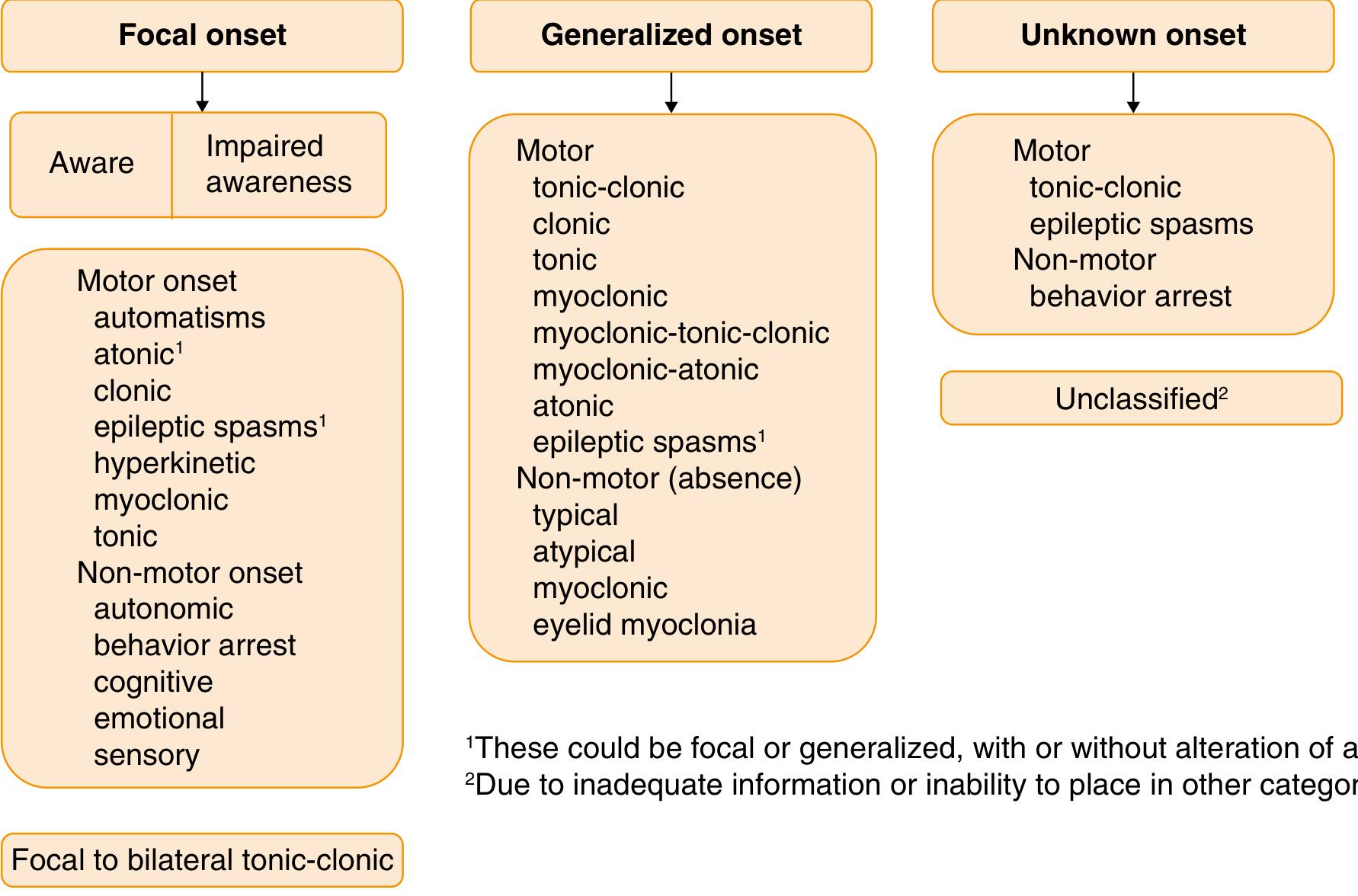
| Old Term (1981) | New Term (2017) |
|---|---|
| Simple partial seizure | Focal aware seizure (FAS) |
| Complex partial seizure | Focal impaired awareness seizure (FIAS) |
| Secondarily generalized | Focal to bilateral tonic-clonic |
Focal Onset Subtypes
1. Focal Aware Seizures (FAS)
- Awareness is fully intact throughout
- Often called an aura when purely subjective
- Manifestations depend on the brain region involved (see table below)
- Auras are typically brief (seconds to minutes); prolonged auras = aura continua (a form of focal nonconvulsive status epilepticus)
- Prodromes (lasting hours to days) must be distinguished from auras
2. Focal Impaired Awareness Seizures (FIAS)
- Characterized by altered awareness at any point during the seizure
- Impairment can be subtle (slight confusion, slowed responses) to complete amnesia
- Often originate from temporal lobe structures
- May begin with or without an aura
3. Focal to Bilateral Tonic-Clonic
- Focal seizure spreads to involve both hemispheres
- Frontal lobe origin is most common; can occur from any focus
- Bystanders often miss the focal onset and only report the bilateral convulsion
- Distinguished from primary generalized onset by careful history or EEG
Clinical Manifestations by Region
| Seizure Type | Brain Region | Clinical Expression |
|---|---|---|
| Clonic | Precentral (rolandic) | Contralateral rhythmic clonic jerking; may jacksonian march |
| Tonic/Dystonic | Supplementary sensorimotor | Unilateral/bilateral tonic posturing; classic fencing posture; speech arrest |
| Somatosensory | Postcentral/parietal | Contralateral tingling, numbness, heat/cold, electric shock sensation |
| Gustatory | Parietal, rolandic operculum, insula | Unpleasant taste (acidic, metallic, salty) |
| Olfactory | Mesial temporal, orbitofrontal | Unpleasant odors (often with gustatory symptoms) |
| Visual | Occipital | Contralateral static/moving lights, shapes; partial/complete vision loss |
| Formed hallucinations | Temporal, occipitotemporal | Formed visual scenes, faces, objects |
| Autonomic, Cognitive, Emotional | Limbic (amygdala, hippocampus, cingulate) | Rising epigastric sensation, nausea, fear, déjà vu, jamais vu, depersonalization, dreamlike state, flushing, piloerection, heart rate changes |
| Impaired Awareness | Bilateral limbic involvement | Automatisms (lip smacking, hand picking), unresponsiveness; formerly "complex partial" |
— Goldman-Cecil Medicine, Table 372-2
Jacksonian March
A distinctive propagation pattern: seizure activity "marches" from hand → arm → leg area along the motor cortex. After the clonic activity, Todd's paralysis (postictal weakness) may last minutes to 1–2 days.
Epilepsia Partialis Continua
Rare condition where the focal motor seizure continues for hours to days; often refractory to medication.
Pathophysiology
The neuronal discharge causing focal seizures may:
- Remain confined to the onset region → purely subjective symptoms (aura)
- Spread locally → progressive ipsilateral involvement (jacksonian march)
- Propagate to bilateral structures → impaired awareness or bilateral convulsion
The evolving EEG reflects this: an initial rhythmic localized discharge (4–7 Hz) becomes higher amplitude and lower frequency as the seizure progresses. Some frontal/association cortex seizures propagate so rapidly that the EEG may appear nonlocalizing on scalp recording; intracranial electrodes may be required.
Etiology
A new-onset focal seizure implies an underlying focal structural or functional brain abnormality until proven otherwise. Common causes:
- Structural: cortical dysplasia, hippocampal sclerosis, tumors (primary or metastatic), vascular malformations, prior stroke, traumatic brain injury, abscess
- Metabolic/Toxic: electrolyte disturbances, hypoglycemia, alcohol/drug withdrawal
- Infectious: encephalitis, meningitis
- Autoimmune: limbic encephalitis (anti-NMDAR, LGI1, CASPR2, etc.)
- Genetic: some focal epilepsy syndromes have genetic underpinnings (e.g., DEPDC5 mutations causing focal cortical dysplasia-related epilepsy)
- Unknown (formerly "cryptogenic")
Investigations
- EEG: Interictal EEG may be normal or show focal epileptiform discharges (spikes, sharp waves). Ictal EEG may be nonlocalizing for deep foci (mesial temporal, inferior frontal)
- MRI brain (high resolution, epilepsy protocol): essential to identify structural lesion; T2/FLAIR for hippocampal sclerosis, cortical dysplasia
- Blood tests: metabolic panel, glucose, electrolytes, CBC, toxicology screen
- LP: if infectious/autoimmune etiology suspected
- PET/SPECT/MEG: adjunctive for surgical planning
- Neuropsychological testing + Wada test: presurgical language/memory lateralization
Treatment
Antiseizure Medications (ASMs) — First-line for Focal Seizures
| Drug | Mechanism | Notes |
|---|---|---|
| Lamotrigine | Na⁺ channel blocker | Broad spectrum; well tolerated |
| Carbamazepine / Oxcarbazepine | Na⁺ channel blocker | Traditional first-line; can worsen generalized seizures |
| Levetiracetam | SV2A modulation | Broad spectrum; no drug interactions |
| Lacosamide | Slow inactivation of Na⁺ channels | Good adjunct |
| Zonisamide, Brivaracetam, Tiagabine, Gabapentin, Perampanel | Various | Adjunctive agents |
| Phenytoin | Na⁺ channel blocker | Oldest non-sedating ASM; still used but many interactions |
| Cenobamate | Novel; multiple targets | Approved for treatment-resistant focal epilepsy; significantly reduces seizures after ≥3 failed drugs |
| Phenobarbital | GABA-A positive allosteric modulator | Limited to refractory cases due to sedation/cognition effects |
— Harrison's Principles of Internal Medicine 22E, Table 436-9
Key principles:
- ~50% of patients achieve seizure freedom with the first ASM
- ~50% of patients with focal epilepsy do not respond to first drug → trial of additional agents
- Serum drug levels guide dosing but clinical response (seizure frequency, side effects) is the primary measure
- Monitoring free drug levels important in hypoalbuminemia (liver/renal disease)
Surgical Treatment (Refractory Focal Epilepsy)
- ~30% of epilepsy patients remain refractory despite adequate medical therapy
- Temporal lobectomy / amygdalohippocampectomy: most common; best results for mesial temporal lobe epilepsy with hippocampal sclerosis
- Lesionectomy: for extratemporal structural lesions
- Multiple subpial transection: when focus is in eloquent cortex
- Hemispherectomy: hemispheric dysplasia (e.g., hemimegalencephaly)
- Presurgical workup: video-EEG monitoring, MRI, PET/SPECT, MEG, neuropsychological testing, Wada test; invasive stereo-EEG if noninvasive insufficient
- Surgical complication rate <5%; seizure freedom achieved in ~60–70% with temporal lobe surgery
Neuromodulation (when surgery not possible)
- Vagus nerve stimulation (VNS)
- Responsive neurostimulation (RNS)
- Deep brain stimulation (DBS) — anterior thalamic nucleus
Important Distinctions
- A focal seizure that secondarily generalizes can be mistaken for a primary generalized tonic-clonic seizure — bystanders often miss the focal onset; EEG and careful history are essential since treatment differs significantly
- The range of potential behaviors linked to focal seizures is broad — bizarre or atypical paroxysmal stereotyped behaviors should raise seizure as a differential even if atypical
- Women of childbearing age: avoid valproic acid where possible given teratogenicity; levetiracetam or lamotrigine preferred
Sources: Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine; Bradley & Daroff's Neurology in Clinical Practice; Katzung's Basic and Clinical Pharmacology 16E; Adams & Victor's Principles of Neurology 12E
This is a shared conversation. Sign in to Orris to start your own chat.