Explain cardiac physiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive material to write a thorough, well-illustrated explanation of cardiac physiology. Let me compile the full answer.
Cardiac Physiology
Sources: Guyton and Hall Textbook of Medical Physiology; Costanzo Physiology 7th Edition; Braunwald's Heart Disease; Miller's Anesthesia
1. Structural Overview
The heart is a four-chambered muscular pump arranged as two serial circuits. The right side receives deoxygenated blood from the systemic veins and pumps it to the lungs (pulmonary circuit); the left side receives oxygenated blood from the lungs and pumps it to the body (systemic circuit).
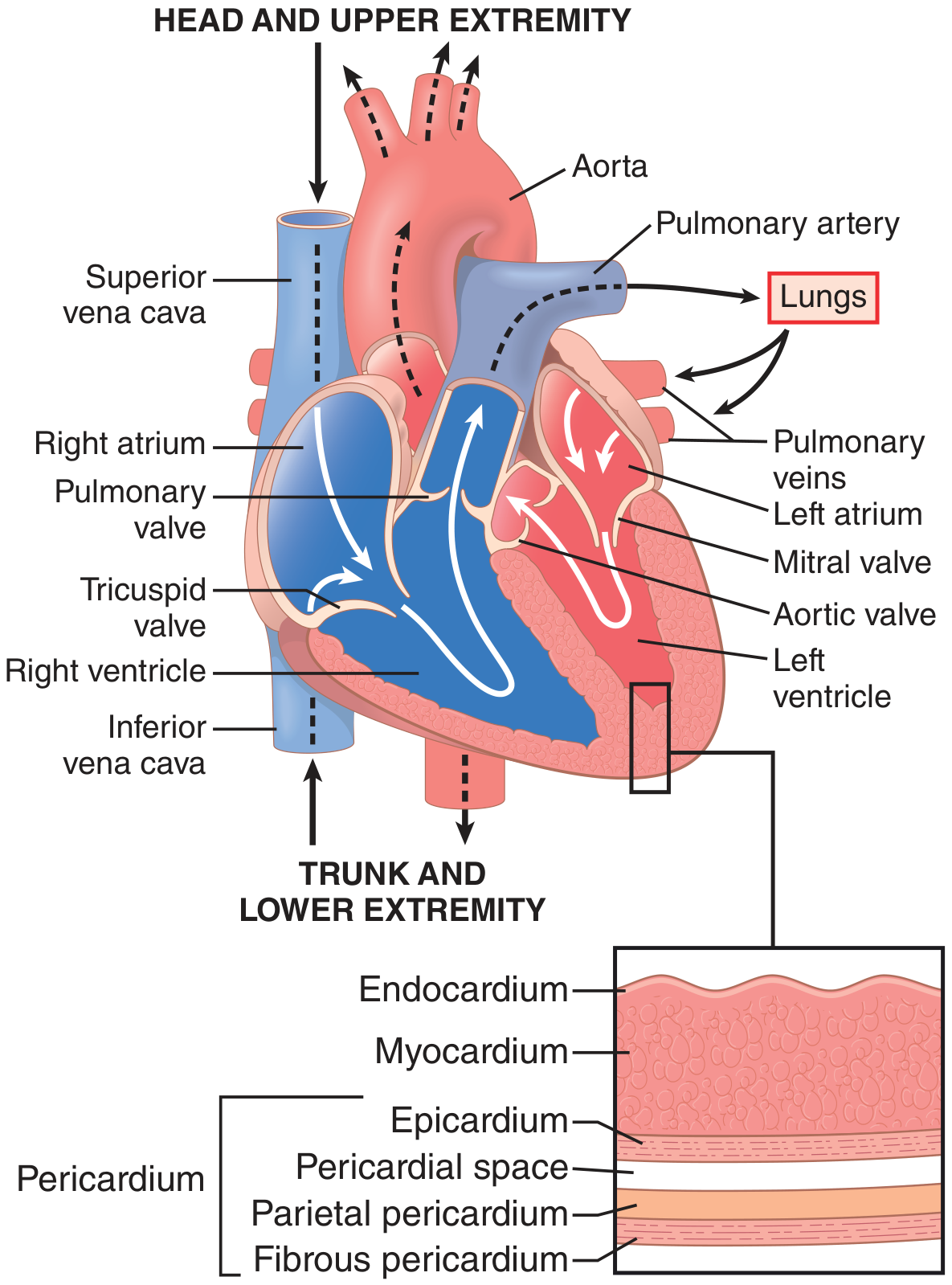
Heart structure showing chambers, valves, great vessels, and the three cardiac wall layers (endocardium, myocardium, epicardium). - Guyton and Hall Textbook of Medical Physiology
The wall itself has three layers:
- Endocardium - innermost smooth lining
- Myocardium - the contracting muscle mass
- Epicardium - outer visceral layer of the pericardium
2. Cardiac Muscle Histology and the Syncytium
Cardiac muscle fibers branch and interdigitate in a lattice pattern. They are striated like skeletal muscle (actin + myosin filaments), but differ in two key ways:
-
Intercalated discs - specialized cell junctions with gap junctions (low-resistance connections) that allow ions to move freely between cells. This makes the heart a functional syncytium: when one cell is excited, the action potential spreads rapidly to all connected cells, causing a coordinated "all-or-nothing" contraction.
-
There are actually two syncytia - the atrial syncytium and the ventricular syncytium - separated by fibrous tissue. The only normal electrical bridge between them is the AV bundle (Bundle of His). This ensures atria contract before ventricles.
Left ventricular torsion: The LV has subepicardial fibers spiraling left and subendocardial fibers spiraling right. During systole, the apex rotates counterclockwise and the base clockwise, creating a wringing motion that optimizes ejection. At end-systole, the LV "untwists" like a spring, aiding rapid diastolic filling. - Guyton and Hall, p. 122
3. Cardiac Action Potentials
3a. Ventricular / Atrial / Purkinje Cell (Fast-Response)
The resting membrane potential is approximately -85 mV. The action potential rises to about +20 mV, a total swing of ~105 mV, and has a characteristic plateau lasting ~200 ms - making cardiac contraction ~15x longer than skeletal muscle contraction.
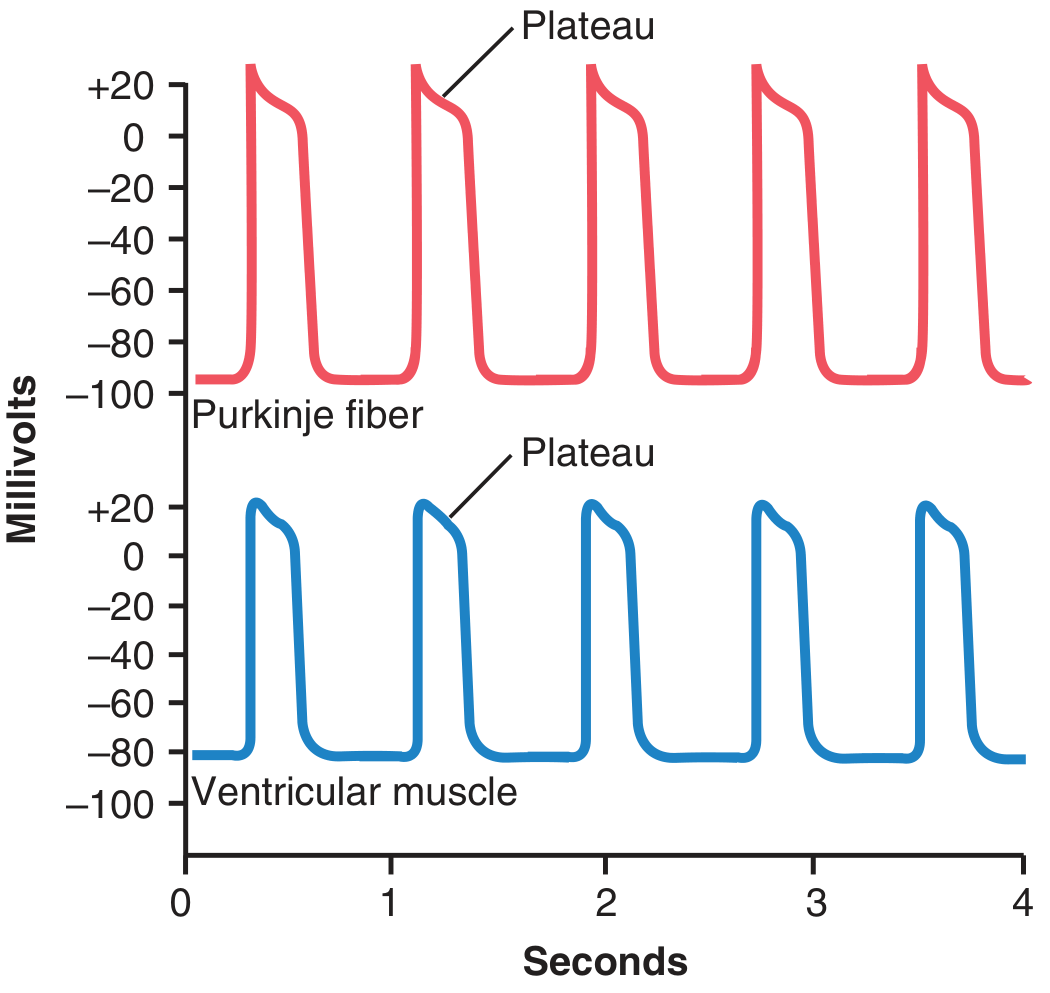
Purkinje fiber (top) and ventricular muscle (bottom) action potentials. Note the plateau in both. - Guyton and Hall
The five phases are:
| Phase | Name | Key Ion Current |
|---|---|---|
| 0 | Upstroke (rapid depolarization) | Rapid Na⁺ influx (INa) via fast Na⁺ channels; membrane goes from -85 to +20 mV |
| 1 | Early rapid repolarization | Inactivation of Na⁺ channels + transient K⁺ efflux (Ito) |
| 2 | Plateau | Slow Ca²⁺ influx (L-type Ca²⁺ channels) balanced against K⁺ efflux - this is unique to cardiac muscle and triggers contraction |
| 3 | Rapid repolarization | Ca²⁺ channels close, K⁺ efflux (IKr, IKs) repolarizes the cell back to -85 mV |
| 4 | Resting potential | -85 mV (maintained by K⁺ leak); stable in ventricular cells |
The plateau (Phase 2) is physiologically essential: it prolongs the refractory period, preventing tetanic (sustained) contractions that would be fatal for a pump. - Costanzo Physiology, p. 140
3b. SA Node (Slow-Response / Pacemaker)
SA node cells differ fundamentally:
- No stable resting potential - they undergo spontaneous diastolic depolarization (Phase 4 "funny current" If, a mixed Na⁺/K⁺ inward current)
- Upstroke is carried by Ca²⁺ (L-type channels), not Na⁺ - hence slower and smaller
- No defined Phase 1 or 2 plateau
This automaticity makes the SA node the natural pacemaker (intrinsic rate: ~60-100 bpm). The AV node fires at ~40-60 bpm and Purkinje fibers at ~15-40 bpm as escape rhythms.
4. The Conduction System
The action potential originates in the SA node (superior right atrium) at time zero and spreads:
- Through both atria (~50 ms) via internodal pathways - atria contract
- AV node - the impulse is delayed here for ~100 ms (AV delay) - this ensures ventricular filling before contraction begins
- Bundle of His → right and left bundle branches → Purkinje fibers → ventricular myocardium
Total activation time for both ventricles: ~220 ms
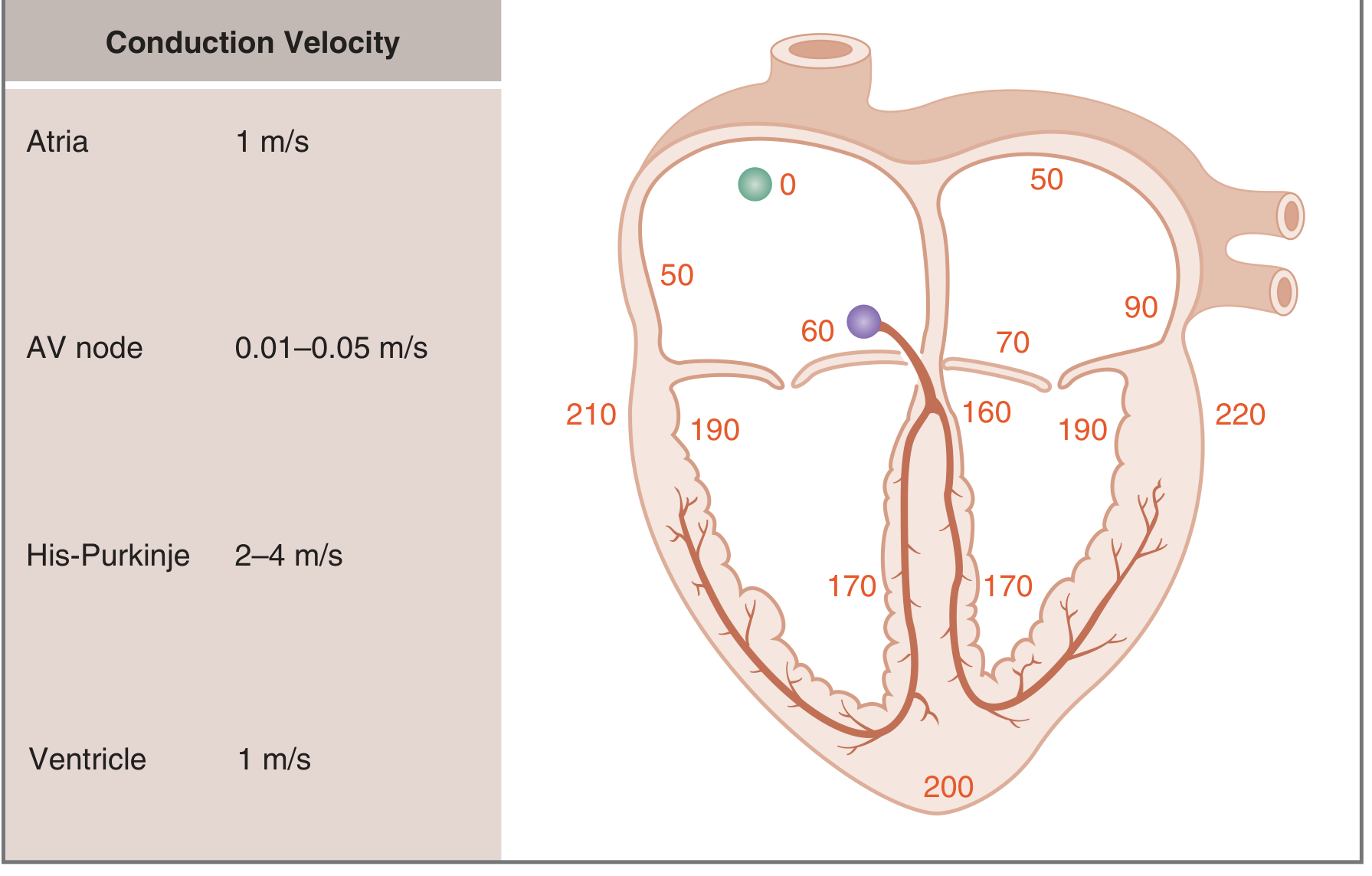
Numbers indicate time in milliseconds from SA node firing. Conduction is slowest at the AV node (0.01-0.05 m/s) and fastest in Purkinje fibers (2-4 m/s). - Costanzo Physiology
Why the AV delay matters: Slow conduction through the AV node (0.01-0.05 m/s) accounts for ~half the total activation time. It ensures the atria have finished contracting and the ventricles are full before ventricular systole begins. - Costanzo Physiology, p. 144
Why fast Purkinje conduction matters: The rapid His-Purkinje conduction (2-4 m/s) activates all parts of the ventricular wall nearly simultaneously, ensuring a coordinated squeeze rather than a peristaltic wave.
5. Excitation-Contraction Coupling
The plateau phase (Phase 2) opens L-type voltage-gated Ca²⁺ channels in the sarcolemma and T-tubules. This Ca²⁺ influx triggers a much larger Ca²⁺ release from the sarcoplasmic reticulum (SR) via ryanodine receptors - a process called calcium-induced calcium release (CICR).
The resulting rise in cytosolic Ca²⁺ (~10-fold increase):
- Binds troponin C on the thin filament
- Displaces tropomyosin, exposing actin binding sites
- Allows myosin cross-bridges to cycle → contraction
Relaxation occurs when Ca²⁺ is pumped back into the SR by SERCA2a (ATP-dependent) and extruded across the sarcolemma by the Na⁺/Ca²⁺ exchanger (NCX).
The heart cannot rely on extracellular Ca²⁺ alone (unlike skeletal muscle which uses mainly SR); it is dependent on transsarcolemmal Ca²⁺ entry to trigger each beat.
6. The Cardiac Cycle
A single cardiac cycle at 72 bpm lasts ~833 ms. It has seven distinct phases:
| Phase | Events | Valves | Heart Sound |
|---|---|---|---|
| A - Atrial systole | P wave on ECG; atrial contraction pushes final ~20% of blood into ventricle; a-wave on venous pulse | Mitral/tricuspid open | S4 (not normally audible) |
| B - Isovolumetric ventricular contraction | QRS; ventricular pressure rises rapidly; all valves closed; volume constant | Mitral closes | S1 (lub) |
| C - Rapid ventricular ejection | Ventricular pressure exceeds aortic; blood ejected rapidly; ST segment on ECG | Aortic valve opens | - |
| D - Reduced ventricular ejection | Slower ejection; T wave repolarization; volume reaches minimum (ESV) | - | - |
| E - Isovolumetric ventricular relaxation | Ventricular pressure falls; all valves closed; volume constant | Aortic valve closes | S2 (dub) |
| F - Rapid ventricular filling | Pressure in ventricle falls below atrial pressure; passive filling | Mitral valve opens | S3 (may be heard in HF) |
| G - Reduced ventricular filling | Slow filling continues; diastasis | - | - |
Key volumes:
- End-diastolic volume (EDV): ~120-130 mL
- End-systolic volume (ESV): ~50-60 mL
- Stroke volume (SV): EDV - ESV = ~70 mL
- Ejection fraction (EF): SV/EDV = ~55-65% (normal ≥55%)
Costanzo Physiology, p. 160
7. Determinants of Cardiac Output
Cardiac Output (CO) = Heart Rate (HR) × Stroke Volume (SV)
Normal CO at rest: ~5 L/min (can reach 20-25 L/min during maximal exercise)
Stroke volume is governed by three factors:
Preload
The stretch of ventricular muscle at end-diastole, determined mainly by EDV. Higher preload (more filling) → greater stretch → stronger contraction. Clinically represented by end-diastolic pressure or volume.
Frank-Starling Law
Increased venous return stretches the ventricular walls, increasing EDV. This stretches individual sarcomeres toward their optimal length, producing more overlap between actin and myosin and a stronger, more forceful contraction. Thus:
"The heart has a built-in mechanism that normally allows it to pump automatically the amount of blood that flows from the veins into the right atrium." - Guyton and Hall, p. 251
The Bainbridge reflex also plays a role: stretching of the right atrium directly stimulates the SA node and triggers sympathetic reflexes to increase heart rate by 10-15%.
Afterload
The resistance the ventricle must overcome to eject blood - determined primarily by aortic pressure (for the left ventricle) and pulmonary arterial pressure (for the right ventricle). Increased afterload decreases stroke volume unless compensated by increased contractility.
Contractility (Inotropy)
The intrinsic force of contraction at a given preload and afterload. Key modulators:
- Sympathetic stimulation (catecholamines, β₁ receptors) → increases heart rate (chronotropy) and contractility (inotropy) via cAMP/PKA-mediated phosphorylation of L-type Ca²⁺ channels and phospholamban (accelerates SR Ca²⁺ reuptake)
- Parasympathetic stimulation (vagus nerve, M2 receptors) → decreases heart rate (mainly) and contractility (less so)
- Digitalis → inhibits Na⁺/K⁺-ATPase → raises intracellular Na⁺ → reduces NCX Ca²⁺ extrusion → more Ca²⁺ available → positive inotropy
8. Coronary Circulation
The heart is perfused by the right and left coronary arteries arising from the aortic root. Important features:
- Left ventricle is perfused mainly in diastole: During systole, the contracting myocardium compresses intramural vessels, nearly stopping flow. This is why tachycardia (shortened diastole) reduces myocardial perfusion.
- Myocardial O₂ extraction is already ~70% at rest (compared to ~25% in skeletal muscle), so increased demand is met primarily by vasodilation and increased flow, not increased extraction.
- Autoregulation maintains flow across perfusion pressures of ~60-130 mmHg.
9. Regulation of Heart Rate
| Autonomic Input | Receptor | Effect |
|---|---|---|
| Sympathetic | β₁-adrenergic | ↑ HR (chronotropy), ↑ force (inotropy), ↑ conduction velocity (dromotropy), ↑ relaxation speed (lusitropy) |
| Parasympathetic (vagus) | M2 muscarinic | ↓ HR, ↓ AV conduction |
Other regulators:
- Temperature: fever increases heart rate (~10 bpm per 1°C rise)
- Electrolytes: hyper/hypokalemia, hypercalcemia alter action potential duration and conduction
- Hormones: epinephrine, thyroid hormone, atrial natriuretic peptide (ANP - secreted by atria when stretched, promotes natriuresis and vasodilation)
Summary
Cardiac physiology integrates cellular electrophysiology, mechanical function, and neurohumoral regulation into a system that can precisely match output to metabolic demand. The key principles are:
- The SA node drives automaticity; the AV node enforces a protective delay
- The plateau action potential prevents tetany and allows calcium-triggered contraction
- The cardiac cycle is an orchestrated sequence of pressure, volume, and valve events
- The Frank-Starling mechanism auto-regulates output based on venous return
- The autonomic nervous system fine-tunes rate and contractility moment-to-moment
This is a shared conversation. Sign in to Orris to start your own chat.