Hi
Hey! How can I help you today?
Explain ABG interpretation in detail with using photos
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Searching the Web
ABG interpretation diagram flowchart pH PaCO2 HCO3 steps
I now have everything I need for a comprehensive, well-illustrated response. Let me compile it all.
Arterial Blood Gas (ABG) Interpretation
ABG analysis is one of the most essential skills in clinical medicine. It gives you real-time information about a patient's acid-base balance, ventilation, and oxygenation. Here is a complete, step-by-step guide.
Normal ABG Values
| Parameter | Normal Value | Normal Range |
|---|---|---|
| pH | 7.40 | 7.35 - 7.45 |
| PaCO₂ | 40 mmHg | 38 - 42 mmHg |
| PaO₂ | 100 mmHg | 75 - 100 mmHg |
| HCO₃⁻ | 24 mEq/L | 22 - 26 mEq/L |
| Base Excess | 0 | -4 to +4 |
Remember: pH and PaCO₂ are directly measured. HCO₃⁻ and base excess are calculated values (using the Henderson-Hasselbalch equation).
The Stepwise Approach

Step 1 - Evaluate the pH
Is the patient acidemic or alkalemic?
| pH | Interpretation |
|---|---|
| < 7.35 | Acidemia |
| 7.35 - 7.45 | Normal |
| > 7.45 | Alkalemia |
Step 2 - Evaluate the PaCO₂ (Respiratory Component)
PaCO₂ is controlled by ventilation - it is the respiratory variable.
- In respiratory disorders: pH and PaCO₂ move in opposite directions
- In metabolic disorders: pH and PaCO₂ move in the same direction
| pH | PaCO₂ | Interpretation |
|---|---|---|
| ↓ | ↑ | Respiratory acidosis |
| ↑ | ↓ | Respiratory alkalosis |
| ↓ | ↓ | Metabolic acidosis |
| ↑ | ↑ | Metabolic alkalosis |
Step 3 - Evaluate HCO₃⁻ (Metabolic Component)
Bicarbonate is the metabolic buffer:
- < 22 mEq/L = Metabolic acidosis
- > 26 mEq/L = Metabolic alkalosis
Step 4 - Assess Compensation
The body compensates for primary disorders using the opposite system. Use these formulas:
| Primary Disorder | Expected Compensation |
|---|---|
| Metabolic acidosis | PaCO₂ = 1.5 × [HCO₃⁻] + 8 ± 2 (Winter's Formula) |
| Metabolic alkalosis | PaCO₂ = 0.7 × [HCO₃⁻] + 20 ± 5 |
| Acute respiratory acidosis | ↑ HCO₃⁻ = ΔPaCO₂ / 10 |
| Chronic respiratory acidosis | ↑ HCO₃⁻ = 4 × (ΔPaCO₂ / 10) |
| Acute respiratory alkalosis | ↓ HCO₃⁻ = 2 × (ΔPaCO₂ / 10) |
| Chronic respiratory alkalosis | ↓ HCO₃⁻ = 4 × (ΔPaCO₂ / 10) |
If observed compensation matches the expected formula = simple (single) disorder with appropriate compensation.
If it does not match = suspect a mixed disorder.
Step 5 - Calculate the Anion Gap (AG)
Always calculate the anion gap, even if a metabolic acidosis is not initially obvious.
AG = Na⁺ − (Cl⁻ + HCO₃⁻)
Normal AG = < 12 mEq/L
Albumin correction: If albumin is low, correct AG by adding: 2.5 × (normal albumin − observed albumin)
Anion Gap Metabolic Acidosis - MUDPILES
| Letter | Cause |
|---|---|
| M | Methanol, Metformin, Muscle injury (rhabdomyolysis) |
| U | Uremia |
| D | DKA (diabetic ketoacidosis), other ketoacidosis |
| P | Propylene glycol, Paraldehyde |
| I | Isoniazid, Iron |
| L | Lactic acidosis |
| E | Ethanol, Ethylene glycol |
| S | Salicylates, Short gut |
Non-Anion Gap Metabolic Acidosis
Normal AG acidosis = bicarbonate loss or excess chloride. Causes: diarrhea, GI fistulas, NG suctioning, renal tubular acidosis (RTA), excess normal saline.
Urine Anion Gap helps differentiate:
Urine AG = Urine (Na⁺ + K⁺ − Cl⁻)
- Positive urine AG = GI HCO₃⁻ loss (e.g., diarrhea)
- Negative urine AG = Renal HCO₃⁻ loss (e.g., RTA)
Step 6 - Calculate the Delta-Delta Ratio (Δ/Δ)
If an elevated anion gap is present, calculate Δ/Δ to detect hidden mixed disorders:
Δ/Δ = (Observed AG − 12) / (24 − Observed HCO₃⁻)
| Δ/Δ Ratio | Interpretation |
|---|---|
| < 1.0 | Mixed anion gap + non-anion gap metabolic acidosis |
| 1.0 - 2.0 | Pure anion gap metabolic acidosis |
| > 2.0 | Anion gap acidosis + concurrent metabolic alkalosis (or compensated chronic respiratory acidosis) |
Step 7 - Evaluate PaO₂ (Oxygenation)
Oxygenation assessment is often overlooked but must not be:
| PaO₂ | Classification |
|---|---|
| 75 - 100 mmHg | Normal |
| 60 - 74 mmHg | Mild hypoxemia |
| 45 - 59 mmHg | Moderate hypoxemia |
| < 45 mmHg | Severe hypoxemia |
Also calculate the A-a gradient (alveolar-arterial oxygen difference) for more precise oxygenation assessment:
PAO₂ = (FiO₂ × 713) − (PaCO₂ / 0.8)
A-a gradient = PAO₂ − PaO₂
Normal A-a gradient = 5-15 mmHg (increases with age)
Quick Summary Diagram

The Four Primary Disorders at a Glance
| Disorder | pH | PaCO₂ | HCO₃⁻ | Compensation |
|---|---|---|---|---|
| Respiratory Acidosis | ↓ | ↑ | ↑ (compensatory) | Renal retention of HCO₃⁻ |
| Respiratory Alkalosis | ↑ | ↓ | ↓ (compensatory) | Renal excretion of HCO₃⁻ |
| Metabolic Acidosis | ↓ | ↓ (compensatory) | ↓ | Hyperventilation (Kussmaul breathing) |
| Metabolic Alkalosis | ↑ | ↑ (compensatory) | ↑ | Hypoventilation |
Worked Clinical Example
ABG results: pH 7.14 | PaCO₂ 73 mmHg | HCO₃⁻ 21 mEq/L | Na⁺ 138 | Cl⁻ 105
- pH 7.14 - Acidemia
- PaCO₂ 73 (elevated) - Primary respiratory acidosis; pH and PaCO₂ are moving in opposite directions
- HCO₃⁻ 21 - Slightly low, expected for acute respiratory acidosis (minimal time for renal compensation)
- Check compensation: Expected ↑HCO₃⁻ = ΔPaCO₂/10 = (73-40)/10 = 3.3 mEq/L → expected HCO₃⁻ ≈ 27.3 (acute). Observed is only 21 - this suggests a concurrent metabolic acidosis is also present (mixed disorder).
- AG = 138 − (105 + 21) = 12 - Normal
- Conclusion: Acute respiratory acidosis + non-anion gap metabolic acidosis (mixed disorder)
Key Memory Tricks
- ROME: Respiratory = Opposite, Metabolic = Equal (pH and PaCO₂ directions)
- MUDPILES: causes of anion gap metabolic acidosis
- Winter's formula: For metabolic acidosis, expected PaCO₂ = 1.5 × HCO₃⁻ + 8 ± 2
- Base deficit < -4 = acidosis; Base excess > +4 = alkalosis
Sources: Current Surgical Therapy 14e, p.1607-1609; Barash Clinical Anesthesia 9e, p.1158-1160; ATS ABG Interpretation Guide
How to give ntg in MI patient
Reading File
Finding Sources
Finding Sources
Searching the Web
nitroglycerin NTG administration protocol MI STEMI ACS dose contraindications 2024 guidelines
Finding Sources
Finding Sources
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC9278720
Reading File
Reading File
Loading Image
Finding Sources
I now have everything needed for a thorough, well-sourced answer. Let me compile it.
Nitroglycerin (NTG) in MI - Complete Guide
NTG (glyceryl trinitrate) is a first-line drug in ACS/MI. It works by releasing nitric oxide (NO), which relaxes vascular smooth muscle, causing venodilation (reduced preload) and arterial dilation (reduced afterload), ultimately decreasing myocardial oxygen demand and increasing coronary perfusion.
ACS Treatment Overview (Where NTG Fits)
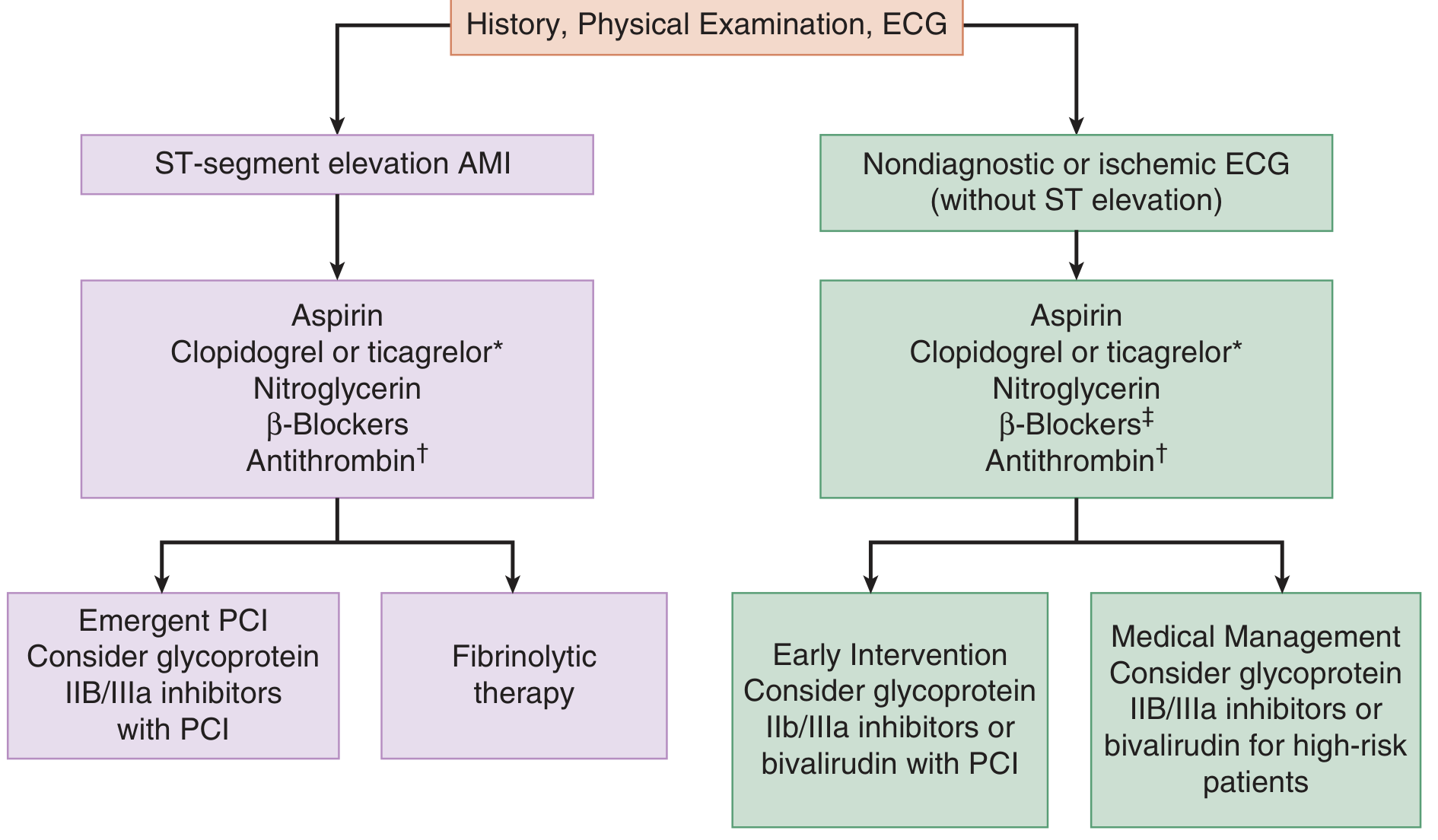
NTG is part of the initial treatment bundle in both STEMI and NSTE-ACS alongside aspirin, antiplatelet agents, and antithrombins.
Before Giving NTG - Mandatory Checklist
Always check these FIRST:
| Check | Threshold | Action |
|---|---|---|
| Systolic BP | < 90 mmHg OR > 30 mmHg drop from baseline | DO NOT GIVE |
| Heart rate | < 50 bpm (bradycardia) | DO NOT GIVE |
| Heart rate | > 100 bpm (tachycardia) | DO NOT GIVE |
| Right ventricular MI | Inferior STEMI (II, III, aVF) | Get right-sided ECG first; avoid NTG |
| PDE-5 inhibitors | Sildenafil/Vardenafil within 24 hours | ABSOLUTE contraindication |
| PDE-5 inhibitors | Tadalafil within 48 hours | ABSOLUTE contraindication |
| Raised ICP | Head injury, known ICP elevation | DO NOT GIVE |
Why RV infarction is critical: The right ventricle is completely preload-dependent. NTG causes venodilation and drops preload - in RV infarction this causes profound, life-threatening hypotension and cardiogenic shock. Always do a right-sided ECG (V4R) in inferior MI before giving NTG.
Why PDE-5 inhibitors matter: Both NTG and sildenafil/tadalafil increase cGMP, leading to additive vasodilation and potential fatal hypotension.
Routes & Dosing
1. Sublingual (SL) - First-line in the field/ED
| Form | Dose | Repeat |
|---|---|---|
| Tablet (0.3 or 0.4 mg) | 0.3-0.4 mg SL | Every 5 minutes, max 3 doses |
| Spray (0.4 mg/spray) | 0.4 mg SL | Every 5 minutes, max 3 doses |
- Onset: 1-3 minutes
- Peak effect: 5-10 minutes
- Duration: ~30 minutes
- Stop after 3 doses or if BP drops significantly
2. Intravenous (IV) - For persistent symptoms, hypertension, pulmonary edema
Used when sublingual NTG fails or continued infusion is needed (in-hospital).
| Step | Rate |
|---|---|
| Starting dose | 5-10 mcg/min |
| Titration | Increase by 5 mcg/min every 3-5 minutes |
| If no response at 20 mcg/min | Increase by 10-20 mcg/min increments |
| Maximum | Up to 400 mcg/min (titrate to effect) |
- Use non-PVC tubing (NTG absorbs into PVC; if PVC must be used, start at 25 mcg/min)
- Monitor BP continuously during IV infusion
- Target: symptom relief without dropping SBP below 90 mmHg
3. Topical/Transdermal - Less common in acute MI
- Nitro paste (2%): 1-2 inches applied to chest wall
- Transdermal patch: used more for chronic angina prevention, less in acute MI
Duration of NTG in MI
| Scenario | Duration |
|---|---|
| Acute chest pain relief | Until symptoms resolve (usually 3 SL doses max) |
| IV for ongoing ischemia | Up to 24-48 hours in stable patients |
| STEMI - routine use | Not recommended routinely (Fuster & Hurst's Heart, 15e) - only if ongoing symptoms, hypertension, or pulmonary edema |
| NSTEMI/UA | Continue for symptom control |
Important note: The routine (prophylactic) use of nitrates in the acute phase of STEMI has shown NO mortality benefit in clinical trials. NTG is used only for symptom relief (ongoing chest pain, hypertension, heart failure/pulmonary edema) - not routinely for all STEMI patients. - Fuster & Hurst's Heart, 15e
Monitoring During NTG
- BP every 5 minutes during SL dosing; continuous during IV
- Heart rate and rhythm
- Symptom relief (chest pain scale)
- Watch for: headache, dizziness, hypotension, syncope, reflex tachycardia
Key Contraindications Summary
STOP NTG if:
- SBP < 90 mmHg (or > 30 mmHg drop from baseline)
- Bradycardia < 50 bpm OR Tachycardia > 100 bpm
- Right ventricular infarction (inferior MI on ECG)
- Sildenafil/Vardenafil within 24 hrs
- Tadalafil (Cialis) within 48 hrs
- Hypertrophic obstructive cardiomyopathy
- Raised intracranial pressure
- Severe anemia
Side Effects
| Effect | Management |
|---|---|
| Headache ("nitrate headache") | Most common; reassure, can pre-treat with acetaminophen |
| Hypotension | Stop NTG, lay patient flat, IV fluids if needed |
| Reflex tachycardia | Usually self-limiting; may need beta-blocker |
| Dizziness/syncope | Keep patient lying down |
| Methemoglobinemia | Rare, more with high-dose IV; treat with methylene blue |
Quick Memory Rule
"HINT" - when to HOLD NTG:
- H - Hypotension (SBP < 90)
- I - Inferior MI (RV infarction risk)
- N - No pulse (bradycardia < 50)
- T - Took sildenafil/Tadalafil recently
Sources: Tintinalli's Emergency Medicine (Comprehensive Study), p.385; Fuster & Hurst's Heart 15e, p.1706; PMC: NTG in the ED; AHA/ACC STEMI & NSTEMI Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.