Tracheo oesophageal fistula for md exams 10 marks answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full MD exam answer:
Tracheo-Oesophageal Fistula (TOF) - MD Exam Answer
Definition
Tracheo-oesophageal fistula (TOF) is an abnormal communication between the trachea and the oesophagus. It is most commonly associated with oesophageal atresia (OA) and is one of the most frequent congenital anomalies encountered by neonatal surgeons.
Incidence: 1 in 2000-4500 live births. Males are more commonly affected.
Embryology
During the 4th week of embryonic development, the foregut normally divides into a ventral respiratory component and a dorsal GI component, separated by the tracheo-oesophageal septum formed by fusion of lateral mesodermal ridges.
- Failure of complete division of the cranial foregut results in a defective tracheo-oesophageal septum, producing a TOF.
- Incomplete separation of the developing oesophagus and trachea by the lateral mesodermal ridges results in an isolated TOF.
- The embryologic origin of OA + TOF combined is less clearly understood.
Classification (Gross Classification)
The most widely used classification is Gross's, with 5 types:
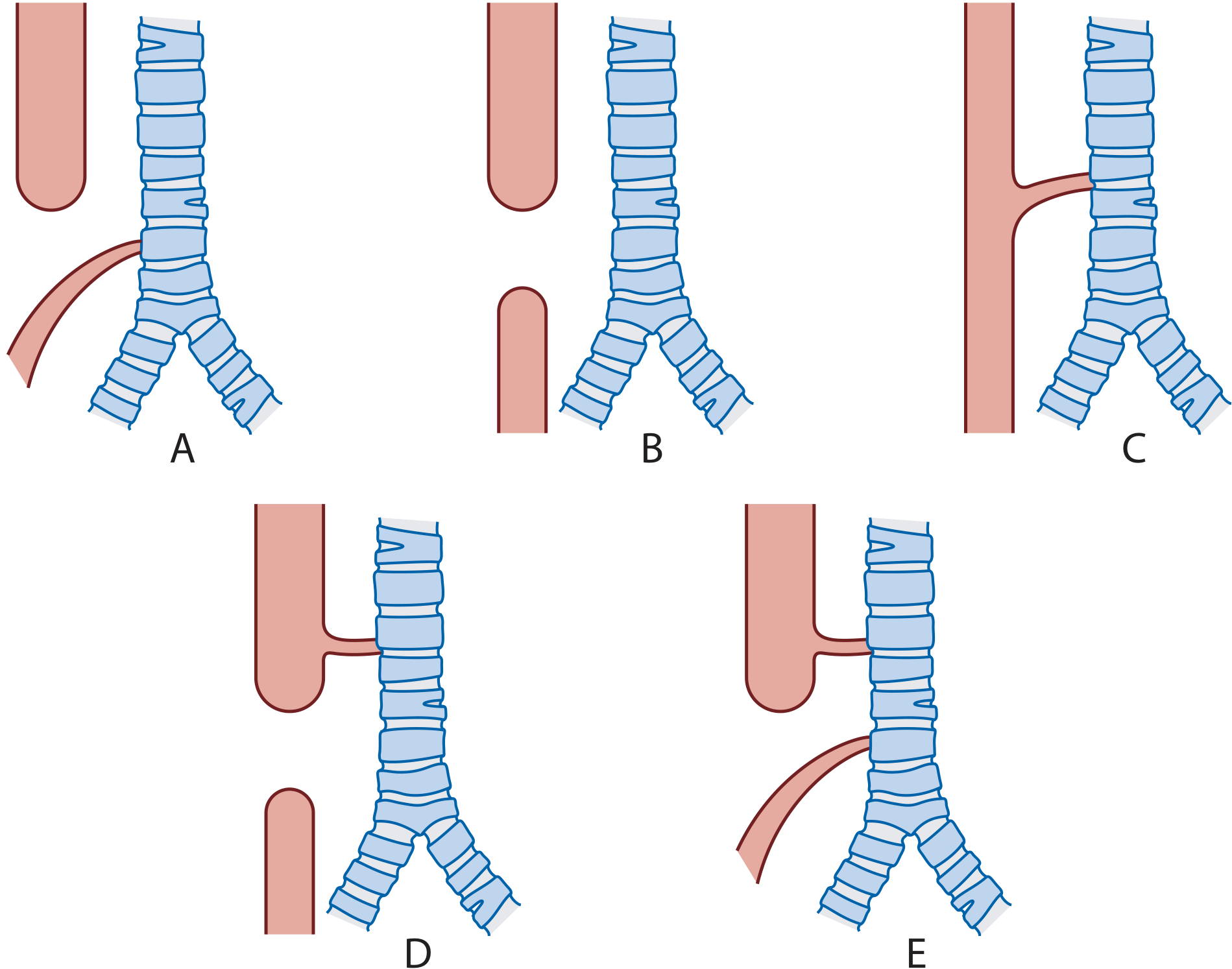
Types and incidences (Scott-Brown's Otorhinolaryngology, Vol 2)
| Type | Description | Incidence |
|---|---|---|
| A | OA with distal TOF (blind proximal pouch + fistula to distal oesophagus from trachea/carina) | ~82-85% |
| B | Isolated OA (no fistula) | 8-10% |
| C | Isolated H/N-type TOF (no atresia; patent oesophagus with fistula) | 4-6% |
| D | OA with proximal TOF | 1-2% |
| E | OA with both proximal and distal TOF | <1% |
Type A is by far the most common (>80% of cases).
The H-type (Type C) fistula is clinically distinct - it presents later in infancy or childhood with recurrent chest infections and respiratory symptoms, rather than at birth.
Associated Anomalies - VACTERL Association
More than 50% of TOF cases have associated anomalies, grouped as the VACTERL association:
- V - Vertebral anomalies
- A - Anorectal malformations
- C - Cardiac defects (most common associated anomaly)
- TE - Tracheo-Oesophageal fistula
- E - Oesophageal atresia
- R - Renal anomalies
- L - Limb defects (especially radial ray)
Other associations: duodenal atresia, small bowel malrotation/volvulus, Down syndrome.
Clinical Features
Antenatal
- Polyhydramnios (in ~50% of OA cases) - due to inability of amniotic fluid to pass through the GI tract for absorption
- Absent stomach bubble on antenatal ultrasound after 20 weeks
- Dilated and blind-ending upper oesophageal pouch on fetal MRI
Postnatal (OA/TOF - the common type)
The classic triad is:
- Frothing/drooling at the mouth (excess saliva, unable to swallow)
- Choking and cyanosis - especially on feeding
- Respiratory distress and aspiration
- Feeds precipitate severe choking and aspiration
- Gas in the abdomen due to air passing through the distal fistula into the stomach
- Gastric contents may reflux back through the fistula causing aspiration pneumonitis
H-type TOF (late presentation)
- Recurrent chest infections, chronic respiratory disease, bronchospasm
- Often investigated for cystic fibrosis before diagnosis
- May present in the ENT clinic
Diagnosis
Bedside Test
- Inability to pass an orogastric/nasogastric tube - virtually diagnostic of OA. A 10Fr or larger tube must be used (thin tubes may coil in the upper pouch giving a false negative appearance)
Radiological Investigations
-
Chest X-ray (with the NG tube in situ):
- Tube coiled in the upper oesophageal pouch confirms OA
- Gas in the abdomen = associated distal TOF present
- Gasless abdomen = isolated OA (no fistula) or rare proximal fistula only
- Associated vertebral and rib anomalies visible
-
Contrast oesophagogram (tube/pull-back oesophagogram):
- Method of choice for H-type fistula
- Patient prone/left lateral; contrast injected under pressure while NG tube withdrawn under fluoroscopy in lateral view
- Risk of aspiration; resuscitation must be available
- Negative result does not exclude H-type TOF
-
Tracheobronchoscopy:
- Gold standard for identifying fistula position before surgery
- Identifies upper pouch fistulae
- Allows the anaesthetist to position the ETT distal to the fistula
- Mandatory if tube oesophagogram is negative but clinical suspicion remains high
-
Echocardiography - essential preoperatively to exclude congenital heart disease and locate the aortic arch (right-sided in 2% - makes surgery more challenging)
-
Renal ultrasound - to exclude renal anomalies
Pre-operative Management
- Nil by mouth immediately
- Replogle (Sump) tube in the upper oesophageal pouch on continuous suction - prevents aspiration of secretions (must be flushed regularly with air to prevent blockage)
- Prone head-up positioning - reduces aspiration risk
- Avoid endotracheal intubation and positive pressure ventilation (PPV) if possible - PPV forces air through the fistula into the stomach, causing gaseous distension, impaired ventilation, hypoxia, hypercapnia, and risk of GI perforation
- Broad-spectrum antibiotics if aspiration pneumonia present
- Correct metabolic/electrolyte abnormalities
- Full VACTERL workup before surgery
Anaesthetic Considerations
- Inhalational induction preferred; spontaneous ventilation maintained until fistula is ligated
- Bronchoscopy performed after induction to assess fistula size and location
- ETT placed distal to the fistula (may require intentional right main bronchus intubation then careful pullback until equal air entry)
- A balloon embolectomy catheter can be placed in the fistula to occlude it
- Invasive arterial BP monitoring recommended
- Pre-ductal and post-ductal SpO2 monitoring for intracardiac shunts
Surgical Management
Timing
- Surgery is urgent but not an emergency in most cases; performed within the first few days of life
- Pre-operative stabilisation is essential
Approach
- Open extrapleural right posterolateral thoracotomy (standard approach)
- Thoracoscopic (minimally invasive) repair is now widely performed
Procedure
- Fistula identified and dissected from surrounding structures
- Fistula divided and sutured closed flush with the trachea
- End-to-end oesophageal anastomosis (single-layer all-coats) over a trans-anastomotic feeding tube
- Bronchoscopy beforehand guides ETT placement and confirms fistula position
Long-Gap OA (when primary repair is impossible)
- Ligation of TOF + feeding gastrostomy created first
- Upper pouch kept on continuous sump suction
- Delayed primary anastomosis after allowing growth/stretching (weeks to months)
- Open oesophagostomy (spit fistula) may be created as a last resort - but almost always precludes later primary repair
- Oesophageal substitution using gastric pull-up, colonic or jejunal interposition if primary repair is impossible
Post-operative Complications
Early (Days to Weeks)
- Anastomotic leak - occurs in 5-20%; higher in long-gap OA; tension pneumothorax may be the presentation
- Recurrent TOF - due to incomplete ligation or breakdown
- Anastomotic stricture - most common long-term complication; requires oesophageal dilatation
- Pneumonia/respiratory complications
Medium to Long-Term
- Gastro-oesophageal reflux (GERD) - very common; may require Nissen fundoplication
- Tracheomalacia - causes "TOF cough" (barking cough); severe cases may need aortopexy
- Oesophageal dysmotility - lifelong, leads to dysphagia
- Recurrent chest infections
- Barrett's oesophagus (long term)
Prognosis
Using the Waterston Classification (or modern Spitz Classification), prognosis depends on:
- Birth weight
- Presence of pneumonia
- Severity of associated congenital anomalies
Spitz classification:
- Group I (birth weight >1500g, no major cardiac defect): survival >97%
- Group II (birth weight <1500g OR major cardiac defect): survival ~59%
- Group III (birth weight <1500g AND major cardiac defect): survival ~22%
Overall survival with modern neonatal surgery is >90% in well-resourced settings.
Key Points for MD Exams
- Most common type is OA with distal TOF (Type A/Gross C) - ~85%
- H-type (N-type) TOF has no atresia - presents late with recurrent chest infections
- Polyhydramnios antenatally + inability to pass NG tube postnatally = cardinal diagnostic features
- Gas in abdomen on CXR = distal TOF present; gasless abdomen = isolated OA
- VACTERL association - always screen
- Avoid positive pressure ventilation before fistula ligation
- Surgery: fistula ligation + end-to-end oesophageal anastomosis via right extrapleural thoracotomy
- Most common long-term complication = anastomotic stricture + GERD + tracheomalacia
Sources: Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol 2; Grainger & Allison's Diagnostic Radiology; The Developing Human - Clinically Oriented Embryology (Moore); Miller's Anesthesia 10e
This is a shared conversation. Sign in to Orris to start your own chat.