How ppi work in our body
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Here is a complete, textbook-sourced explanation of how PPIs work in the body.
How Proton Pump Inhibitors (PPIs) Work
What Are PPIs?
PPIs include omeprazole, esomeprazole, lansoprazole, pantoprazole, rabeprazole, and dexlansoprazole. They are the most potent acid-suppressing drugs available, reducing both basal and stimulated gastric acid secretion by more than 90% at standard doses.
Step 1 - They Are Prodrugs (Inactive Until Activated)
PPIs are not active when you swallow them. They are weak bases (pKa ~4-5) with an enteric coating that protects them from stomach acid. The coating dissolves in the alkaline duodenum, and the prodrug is absorbed into the bloodstream.
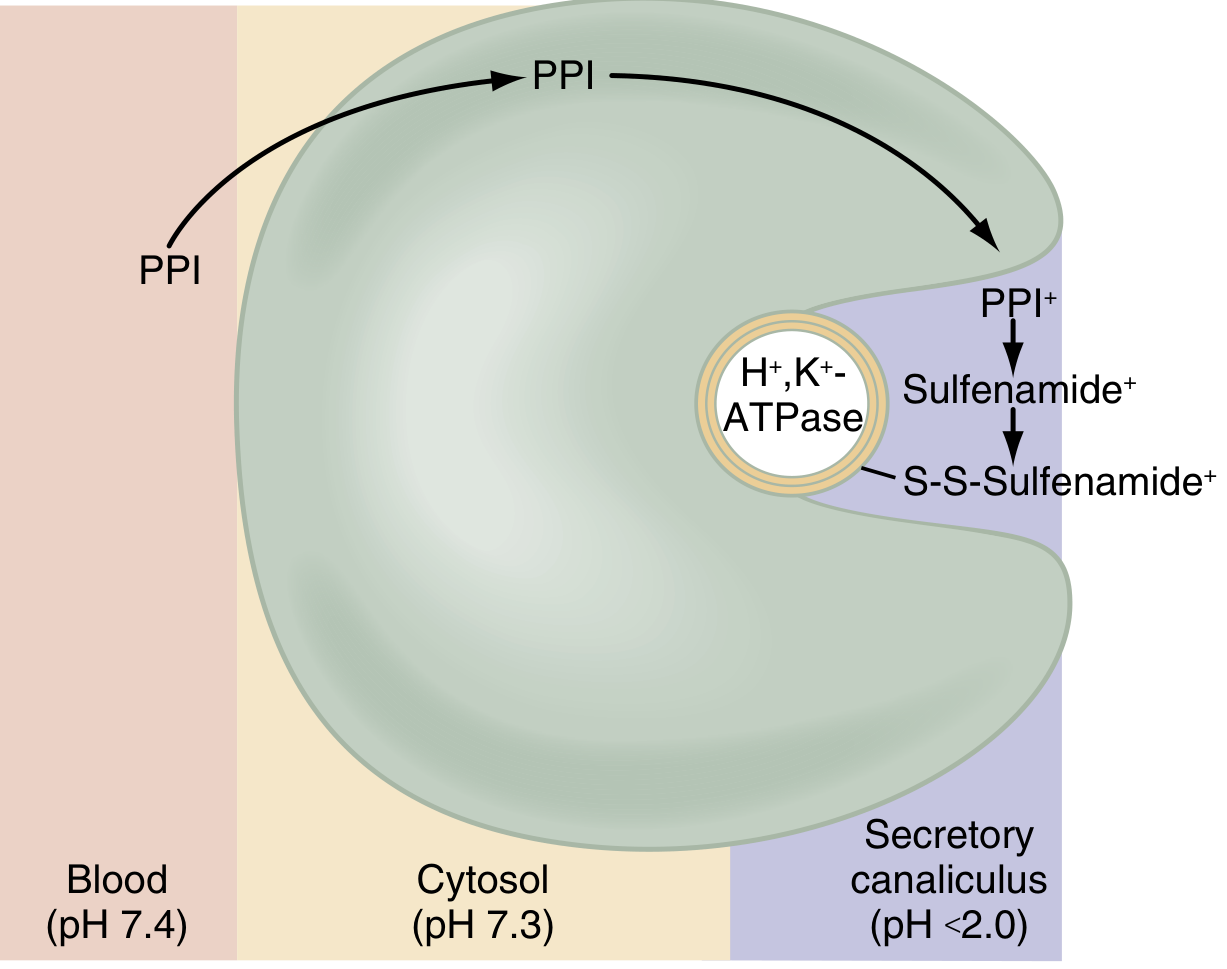
At blood pH 7.4, PPIs are mostly in their non-protonated (uncharged) form - this makes them membrane-permeable and allows them to travel freely through the bloodstream and into cells.
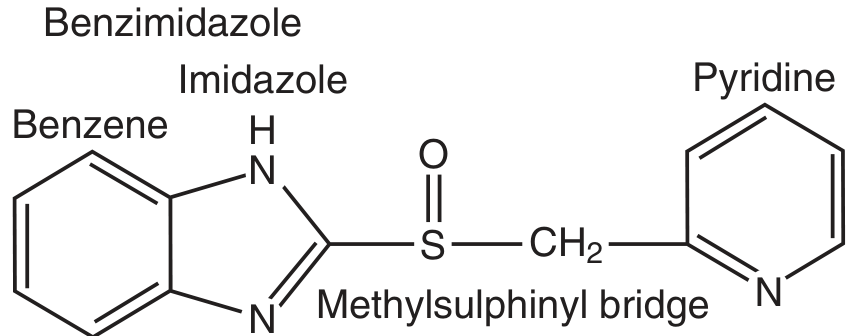
Chemical structure: Each PPI consists of two heterocyclic rings - a benzimidazole and a pyridine - connected by a methylsulfinyl bridge:
Step 2 - Selective Concentration in the Parietal Cell
The PPI travels from blood into the parietal cells of the stomach lining. These cells contain a specialized compartment called the secretory canaliculus, where acid is actively being pumped and the pH drops below 2.0.
Because PPIs are weak bases, they become protonated and "ion trapped" in this extremely acidic environment. The concentration of PPIs in the secretory canaliculus reaches 100,000 to 10,000,000 times higher than in the surrounding blood - this is why they are so selective for parietal cells.
Step 3 - Activation and Covalent Binding
Once trapped in the acidic canaliculus, the PPI undergoes chemical conversion:
- PPI (prodrug) is protonated (PPI⁺)
- It becomes a sulfenic acid, then dehydrates to a sulfenamide
- The sulfenamide reacts with specific cysteine residues on the alpha-subunit of the H⁺/K⁺-ATPase enzyme, forming a covalent disulfide bond
This is shown in the diagram below:
Different PPIs bind to slightly different cysteine residues: all bind to Cys-813, but omeprazole also binds Cys-822, lansoprazole binds Cys-321, and pantoprazole binds Cys-892.
Step 4 - Irreversible Blockade of the Proton Pump
The H⁺/K⁺-ATPase (proton pump) is the final enzyme in the pathway of gastric acid secretion. It exchanges hydrogen ions (H⁺) for potassium ions (K⁺) across the canalicular membrane, effectively pumping acid into the stomach.
Because PPIs bind covalently and irreversibly, they permanently disable any pump they attach to. Acid secretion only recovers when the stomach synthesizes new pump protein - which takes roughly 18 hours (and longer in humans). This is why the acid-suppressing effect of PPIs far outlasts their short plasma half-life of just a few hours.
Why You Should Take PPIs Before a Meal
PPIs only activate pumps that are actively secreting acid (i.e., inserted in the canalicular membrane). During fasting, most pumps are not active - so a PPI taken on an empty stomach reaches few active targets and is quickly cleared. Taking a PPI 30-60 minutes before the first meal ensures maximum pump activity at the time the drug arrives. (Exception: dexlansoprazole's dual delayed-release formulation can be taken without regard to food.)
What Happens After Long-Term Use
Because PPIs suppress acid production, gastrin levels rise (hypergastrinemia) as a feedback response. This stimulates parietal cell and enterochromaffin-like (ECL) cell hyperplasia, which can persist for up to 3 months after stopping the drug. When PPIs are discontinued after long-term use, this hyperplasia causes a rebound in acid secretion, which can worsen GERD or dyspepsia symptoms transiently.
Clinical Uses
| Condition | Role of PPIs |
|---|---|
| GERD / reflux | First-line acid suppression |
| Peptic ulcer disease | Healing and prevention |
| Zollinger-Ellison syndrome | Control of massive acid hypersecretion |
| NSAID-induced ulcers | Prevention and treatment |
| H. pylori eradication | Used alongside antibiotics |
| Stress ulcer prophylaxis | ICU / high-risk patients |
Key Side Effects
- Fracture risk - increased with use of 1 year or more
- Vitamin B12 deficiency - acid is needed to release B12 from food
- Calcium malabsorption - elevated pH impairs calcium carbonate absorption (calcium citrate is preferred in PPI users)
- C. difficile colitis and diarrhea
- Rebound acid hypersecretion on discontinuation
Sources: Lippincott Illustrated Reviews: Pharmacology, Ch. 42; Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Ch. 51; Katzung's Basic & Clinical Pharmacology, 16th ed.
What are the side effects of long-term PPI use?
Finding Sources
Searching PubMed
proton pump inhibitor long-term adverse effects
Reading File
Reading File
Searching PubMed
proton pump inhibitor kidney dementia fracture risk
Reading File
Reading Article
PMID: 35830032
Reading Article
PMID: 37060552
Here is a thorough, evidence-based breakdown of long-term PPI side effects, graded by how strong the evidence actually is.
Side Effects of Long-Term PPI Use
Important context: Up to 70% of long-term PPI prescriptions may be unwarranted. The vast majority of evidence for adverse effects comes from retrospective observational studies, which cannot fully account for confounding factors. Causality for many associations remains unproven. The key principle is to use PPIs at the lowest effective dose for the shortest necessary duration.
1. Infections
Clostridioides difficile (C. diff)
This is one of the best-supported risks. A 2022 meta-analysis (PMID 35830032) reviewed the evidence and Harrison's 22nd edition confirms a 74% increased risk of C. difficile infection and a 2.5-fold higher risk of reinfection compared to non-users. The FDA has issued a safety alert. The mechanism is thought to involve PPI-induced changes to the gut microbiome - suppressing acid removes a major defense against bacteria entering the GI tract.
Community-Acquired Pneumonia
Long-term acid suppression is associated with higher rates of pneumonia, especially in elderly patients. Reduced gastric acid allows bacterial colonization of the upper GI tract, increasing aspiration risk.
Small Intestinal Bacterial Overgrowth (SIBO)
Meta-analyses report an OR of 2.28 (95% CI 1.24-4.21) for SIBO in PPI users, though the association was strongest in studies using direct culture methods.
2. Nutritional Deficiencies
Vitamin B12
Gastric acid is needed to cleave B12 from food proteins. A 2023 systematic review and meta-analysis (PMID 37060552) of 25 studies found a pooled OR of 1.42 for B12 deficiency in PPI users vs. non-users - a modest but real increased risk. Long-term deficiency can cause megaloblastic anemia and neurological damage (peripheral neuropathy, subacute combined degeneration of the spinal cord).
Magnesium (Hypomagnesemia)
A meta-analysis found a 40% increase in hypomagnesemia in PPI users. Severe hypomagnesemia can cause muscle cramps, arrhythmias, and seizures. This is a known enough risk that the FDA requires a warning label. Checking a magnesium level after 1-2 years of PPI use is reasonable.
Iron Deficiency
Gastric acid is required for converting dietary ferric iron (Fe³⁺) to the absorbable ferrous form (Fe²⁺). Long-term PPI use can contribute to iron deficiency anemia.
Calcium Malabsorption
Elevated gastric pH impairs absorption of calcium carbonate. Calcium citrate is the preferred supplement for long-term PPI users since its absorption is pH-independent.
3. Bone Fractures and Osteoporosis
A meta-analysis found an OR of 1.25 (95% CI 1.14-1.37) for hip fracture in PPI users vs. non-users. A 2024 systematic review (PMID 38458487) examined bone and phosphocalcic metabolism specifically. Reduced calcium absorption is the proposed mechanism. However, prospective studies have not yet confirmed accelerated bone mineral density loss after 5-10 years of PPI use, so while the epidemiological signal is real, the absolute fracture risk increase remains low.
4. Kidney Disease
Multiple studies consistently associate PPI use with:
- Acute interstitial nephritis (an idiosyncratic, hypersensitivity-type reaction)
- Chronic kidney disease (CKD) - especially in the elderly and those with pre-existing kidney disease
Yamada's Textbook notes these appear to be "sporadic idiosyncratic side-effects" in most cases, but the signal in large observational datasets is consistent.
5. Dementia
Long-term PPI use has been reported to be associated with dementia, with an increased risk estimated at 0.07-1.5% per patient per year. Two mechanisms have been proposed:
- Vitamin B12 deficiency leading to neurodegeneration
- Enhanced cerebral beta-amyloid accumulation (PPIs may inhibit enzymes that clear amyloid)
However, the evidence here is inconsistent across studies and causality is widely debated. Confounding (e.g., sicker/older patients taking more PPIs) is hard to rule out.
6. Cardiovascular Effects
Clopidogrel Interaction
Both PPIs and clopidogrel are metabolized by CYP2C19. PPIs can theoretically reduce clopidogrel's antiplatelet effect, increasing cardiovascular risk. Initial observational data suggested this, but a randomized trial did not confirm it. Current guidelines state PPI therapy does not need to be altered in clopidogrel users, though some clinicians separate the dosing of the two drugs by 12-20 hours.
Stroke and Myocardial Infarction
Some meta-analyses have reported a modest increased risk, but this remains contested and is likely confounded by underlying disease severity in PPI users.
7. Rebound Acid Hypersecretion
Stopping PPIs abruptly after long-term use causes a surge in gastric acid above pre-treatment baseline. This happens because:
- Hypergastrinemia during PPI therapy causes parietal cell and ECL cell hyperplasia
- These changes persist for up to 3 months after stopping the PPI
- The result is worsened reflux and dyspepsia, which can trap patients in a cycle of continued use
8. Collagenous Colitis
Diarrhea associated with PPI use can, in some cases, progress to collagenous colitis (hazard ratio ~4.5), particularly with lansoprazole. It usually resolves when the PPI is stopped.
9. Hypergastrinemia and Gastric Tumors (Theoretical)
Chronic hypergastrinemia stimulates ECL cell and parietal cell hyperplasia. In animal models, this has raised concerns about gastric carcinoid development, but population-based studies have not found an increased risk of colorectal or gastric cancer in PPI users. In patients with H. pylori and corpus-predominant gastritis, long-term PPIs may promote atrophic gastritis - some experts recommend testing and treating H. pylori before starting long-term therapy.
Summary Table
| Side Effect | Evidence Strength | Mechanism |
|---|---|---|
| C. difficile infection | Strong (FDA alert) | Gut dysbiosis, lost acid barrier |
| Vitamin B12 deficiency | Moderate (OR ~1.42) | Impaired protein-bound B12 release |
| Hypomagnesemia | Moderate (40% increased risk) | Impaired intestinal Mg transport |
| Iron deficiency | Moderate | Impaired Fe³⁺→Fe²⁺ conversion |
| Hip fracture | Moderate (OR ~1.25) | Reduced calcium absorption |
| Acute interstitial nephritis / CKD | Moderate-consistent | Idiosyncratic/immune mechanism |
| Dementia | Weak-inconsistent | B12 deficiency; amyloid accumulation? |
| Pneumonia | Moderate | Bacterial overgrowth + aspiration |
| Rebound acid hypersecretion | Strong | ECL/parietal cell hyperplasia |
| Clopidogrel interaction | Weak | CYP2C19 competition |
| Collagenous colitis | Moderate (HR ~4.5) | Direct mucosal/collagen effect |
Sources: Yamada's Textbook of Gastroenterology, 7th ed.; Harrison's Principles of Internal Medicine, 22nd ed.; Chinzon et al., Arq Gastroenterol 2022 (PMID 35830032); Choudhury et al., Expert Rev Gastroenterol Hepatol 2023 (PMID 37060552).
This is a shared conversation. Sign in to Orris to start your own chat.